 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Biokemistri, Vol. 21, No. 2, Dec, 2009, pp. 71-77 Alteration of Plasma Lipid Profiles and Atherogenic Indices by Stachytarpheta jamaicensis L. (Vahl) Chigozie Jude Ikewuchi* and Chidinma Catherine Ikewuchi Department
of Biochemistry, Faculty of Science, University of Port Harcourt, P.M.B. 5323,
Port Harcourt, Nigeria. Received July 15, 2009 Code Number: bk09010 Abstract The effects of Stachytarpheta jamaicensis tea on the plasma lipid profile and atherogenic indices were investigated in rabbits. The test group received daily, by intra-gastric gavages, 15mg/kg of aqueous extract. The treatment led to significant decreases (p<0.05) in plasma levels of total, LDL- and VLDL-cholesterol and triglycerides, and increase (p<0.05) in plasma HDL cholesterol level. It also produced significant (p<0.05) decreases in the atherogenic indices; cardiac risk ratio, atherogenic coefficient and atherogenic index of plasma. These results suggest the use of Stachytarpheta jamaicensis tea in the management of dyslipidemia whether primary or secondary to obesity, diabetes mellitus and hypertension, and by extension, the reduction of the risk of cardiovascular diseases Keywords:Coronary heart disease, diabetes mellitus, dyslipidemia, hypertension, Stachytarpheta jamaicensis
INTRODUCTION Cardiovascular disease is one of the world’s leading causes of death. One of the major risk factors for the development of cardiovascular disease is dyslipidemia, which may be primary or associated with hypertension, diabetes mellitus and obesity1-9.Dyslipidemia usually involve elevated plasma levels of triglycerides, total, LDL and VLDL cholesterol and a low level of HDL cholesterol1-3,9.Therefore, any nutritional and pharmacologic intervention that improves or normalizes abnormal lipid metabolism may be useful for reducing the risk of cardiovascular diseases2,9.Several drugs are at present, available for the management of dyslipidemia. However, there is renewed interest in the use of herbal products10,11. This may be attributable to the down turn in the economy, as traditional medicine is perceived to be a cheaper means of treatment10,12. No wonder, WHO in 1991, developed guidelines for the assessment of herbal medicine10. In Nigeria, a great number of plants are currently used in the management of a wide range of illnesses by traditional medical practitioners. Stachytarpheta jamaicensis is one of such plants. It is used in traditional medicine as an analgesic, antacid, anti-inflammatory, antispasmodic, antiulcerogenic, digestion stimulant, diuretic, febrifuge, gastroprotective, hepatoprotective, hypoglycemic, hypotensive, sedative and tonic13-16.Its phytochemical constituents include flavonoids, triterpenes, monoterpenes, iridoids, phytosterols, aromatic acids, GABA, dopamine and alkanes15,17. In spite of this multitude of ethnomedical applications, we found nothing in biochemical literature, relating to the effect of the plant on plasma lipid profiles. In view of this, we undertook a preliminary investigation in which we found that the aqueous infusion (tea) of Stachytarpheta jamaicensis significantly reduced the weight and plasma total cholesterol of normal rabbits18.Therefore, as a follow up, the present study was designed to investigate the effect of the tea on plasma lipid profile and some atherogenic indices of rabbits, with a view to finding any therapeutic benefit in the management of dyslipidemia – a risk factor for development of cardiovascular disease and a common characteristic of diabetes mellitus and hypertension – especially in view of the reports that the treatment of hypertension with thiazide diuretics accentuates hyperlipidemia19. MATERIALS AND METHODS Preparation of the Leaves The tea bags were collected from the Integrated Services Unit of Benson Idahosa University, Benin City, Nigeria. See Idu et al 20 for a description of how to prepare the leaf powder. The tea bags were used to prepare aqueous infusions by placing a tea bag containing 1.8g of dried powdered plant (Stachytarpheta jamaicensis) in 250ml of boiled water for 8h to simulate the traditional procedure for preparing the tea. The resultant aqueous extract was stored for subsequent use. A known volume of this extract was evaporated to dryness, and the weight of the residue used to determine the concentration of the filtrate, which was in turn used to determine the dose of administration of the extract to the test animals. The dosage of dispensation/administration of the tea adopted in this study was extrapolated from that recommended on the tea packs (as administered by the traditional medical practitioners). Experimental Design Three-month old New Zealand white rabbits weighing between 0.85-1.5kg was obtained from a breeder in Benin City. The animals were housed in clean, disinfected hutches and acclimatized on guinea growers mash (Bendel Feed and Flour Mills Ltd., Ewu, Nigeria) for a week after which fasting blood samples were collected for the assay of baseline plasma lipid profiles. They were subsequently weighed and randomly assigned into two groups. The test group received by intra-gastric gavages, 15mg of aqueous extract/kg of body weight, while the control group received appropriate volumes of water by the same route. Fresh feed was provided daily, while stale remnants were discarded. The animals had free access to mash and water. The rabbits were weighed weekly to allow for adjustment in administration of the extract. The treatment lasted for 8 days. The fasting blood samples were collected on day 0 (baseline), 1 and 8, for determination of plasma lipid profiles. Determination of the Plasma Lipid Profiles/Indices Plasma total cholesterol (TC), HDL-cholesterol (HDLC) and triglyceride (TG) were assayed enzymatically with commercial test kits (Randox Laboratories, Crumlin, England), at the Chemical Pathology Department, University of Benin Teaching Hospital (UBTH), Benin City, Nigeria. Plasma LDL-cholesterol was calculated using the Friedewald equation21, as follows:
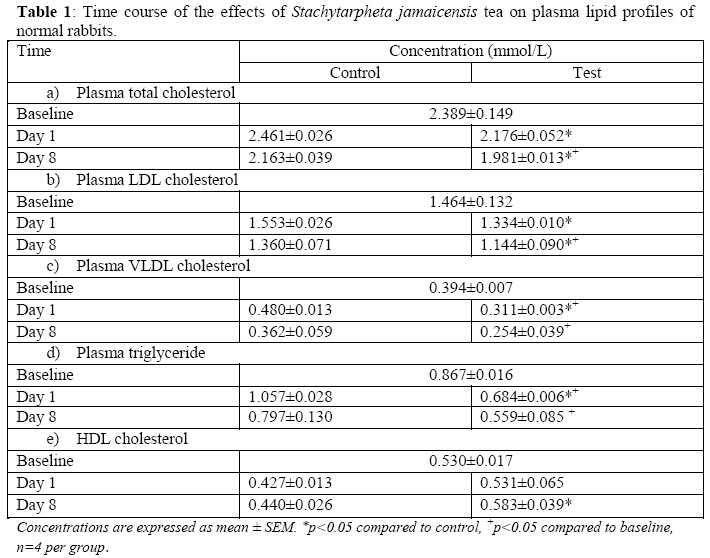
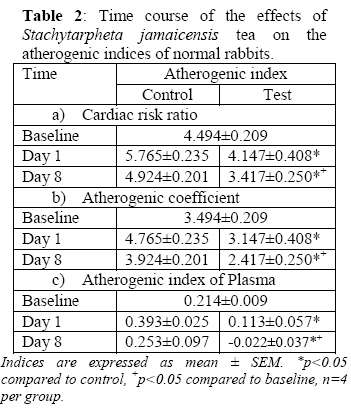
Statistical Analysis of Data All values are quoted as the mean ± S.E.M. The values of the various parameters for the test and control groups were analyzed for statistical significant differences using the student’s t-test. p<0.05 was assumed to be significant. RESULTS The treatment led to significantly lower (p<0.05) plasma levels of total, LDL- and VLDL-cholesterol, and triglycerides. These parameters were significantly lower in the test group compared to the control and baseline values (Table 1). The treatment produced a gradual rise (p<0.10 on day 1 to p<0.005 on day 8) in plasma HDL-cholesterol levels; although these values were only significant at p<0.10 when compared to the baseline HDL-cholesterol levels. The treatment also significantly lowered (p<0.05) the following atherogenic indices; cardiac risk ratio (CRR), atherogenic coefficient (AC) and atherogenic index of plasma (AIP) (Table 2). After treatment, the values of each of these parameters in the test group, were significantly lower (p<0.05), compared to the control and baseline values. DISCUSSION Epidemiological studies have shown that an elevated concentration of total cholesterol in the blood is a powerful risk factor for coronary disease26,27. In this study, the tea significantly lowered plasma total cholesterol of the rabbits (Table 1a). This corroborates our earlier report18.Presently, though the constituent(s) of this decoction that possesses the hypocholesterolemic effect is yet to be specifically identified, there is evidence that the plant contains monoterpenoids, isoflavones, esters of triterpene alcohols and phytosterols. Since monoterpenoids, isoflavones, esters of triterpene alcohols and phytosterols8,28-32 from other plants sources, have all been independently reported to exert hypocholesterolemic effects, any one or a combination of these phytochemicals may be responsible for the effect observed in this study. Increased plasma levels of LDL and VLDL cholesterol is often found in hypertension2,33 and diabetes mellitus1,3,7,9 and is a risk factor for cardiovascular disease11,26,27,34,35. In this study, we observed a significantly lower plasma LDL and VLDL cholesterol levels in the treated animals (Table 1b,c). This effect may be attributable to the flavonoid content of the plant. Middleton et al.36 had earlier reported that citrus flavonoids lower plasma LDL cholesterol in both normolipidemic and hyperlipidemic rats. Plant sterols are also known to lower plasma LDL cholesterol30. Decreases in plasma LDL cholesterol have been considered to reduce risk of coronary heart disease7,9. A high plasma triglyceride level is both an independent and synergistic risk factor for cardiovascular diseases8,25,37; and is often associated with hypertension2,33, abnormal lipoprotein metabolism, obesity, insulin resistance and diabetes mellitus3,9,37. The tea significantly reduced plasma levels of triglycerides (Table 1d). This effect may have been mediated by the flavonoid content of the plant. Flavonoids decrease plasma levels of triglycerides36. Low plasma HDL cholesterol is a risk factor for cardiovascular diseases7,8,34,35,38 and is often found in hypertension2,33 and diabetes mellitus1,3,7,9. In this study, the tea increased plasma HDL cholesterol levels (Table 1e), an effect that may again be mediated by the flavonoids; since according to Middleton et al.36 flavonoids increased plasma HDL cholesterol in both normolipidemic and hyperlipidemic rats. Increases in plasma HDL cholesterol have been considered to reduce risk in coronary heart disease7,38. High HDL exerts a protective effect by enhancing reverse cholesterol transport by scavenging excess cholesterol from peripheral tissues, which it esterifies with the aid of lecithin: cholesterol acyltransferase, and delivers to the liver and steroidogenic organs for subsequent synthesis of bile acids and lipoproteins, and eventual elimination from the body27,38,39; and inhibiting the oxidation of LDL as well as the atherogenic effects of oxidized LDL by virtue of its antioxidant27,38,39,40 and anti-inflammatory property27,41. Atherogenic indices are powerful indicators of the risk of heart disease: the higher the value, the higher the risk of developing cardiovascular disease and vice versa8,22-25,42. In this study, we observed that the tea significantly reduced atherogenic indices CRR (Table 2a), AC (Table 2b) and AIP (Table 2c). According to Usoro et al.42 lower atherogenic index is protective against coronary heart disease. All of these results indicate a possible protective mechanism of the tea against the development of atherosclerosis and coronary heart disease, as well as the dyslipidemic conditions that characterize hypertension and diabetes mellitus. Provided animal to human extrapolation is allowed, the therapeutic implication of this result to the management of hypertension cannot be overemphasized, especially in view of the reports that some commonly used antihypertensive diuretic drugs (e.g. thiazides), accentuate hyperlipidemia19. REFERENCES
© 2009 Nigerian Society for Experimental Biology The following images related to this document are available:Photo images[bk09010t2.jpg] [bk09010t1.jpg] |
| |||||||||

{kind=link}
{kind=link}