 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Biokemistri, Vol. 23, No. 3, Dec, 2011, pp. 108-117 Review Article Towards the management of hypertension: Modulation of the renin-angiotensin system by food protein hydrolysates and peptides Chibuike C. Udenigwe1*, Chukwunonso E.C.C. Ejike2, Joycelyn K. Quansah1,3, Michael O. Eze4 1Department
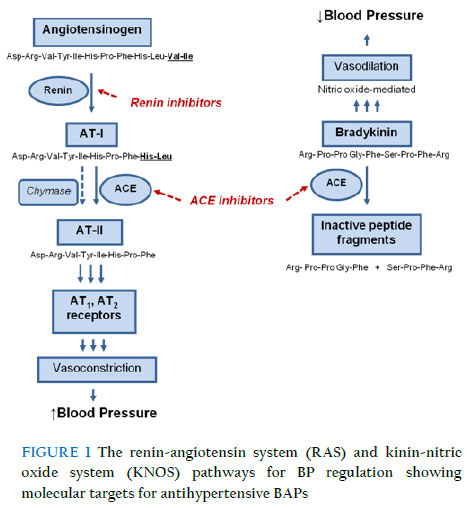
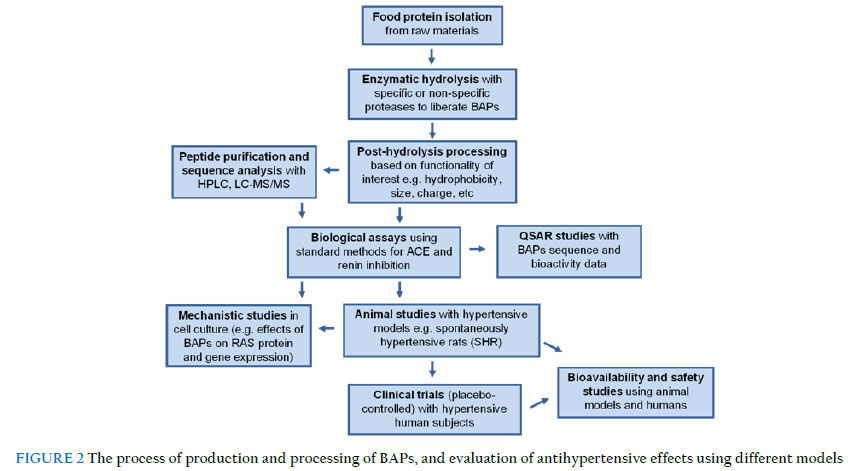
of Food Science, University of Guelph, Guelph, Ontario, N1G 2W1, Canada; Received: 22 November 2011 ABSTRACT In response to the side effects of antihypertensive drugs, dietary and lifestyle modification approaches have become alternative strategies for prevention and modulation of mild hypertension. Moreover, the use of low molecular size bioactive peptides (BAPs) as antihypertensive agents has gained particular attention as a result of the safety, low cost, and consumer preference for natural health products compared to drugs. BAPs are produced by enzymatic hydrolysis of food proteins followed by post-hydrolysis processing to fractionate the active peptides. Antihypertensive BAPs exert their effect mostly by modulating the renin-angiotensin system pathway leading to decrease in vasoactive peptides with concomitant reduction of elevated blood pressure associated with hypertension in animal models and humans. This review revisits the prevalence of hypertension and the molecular basis of activity, bioavailability and safety of BAPS as well as contradictions and controversies on the use of peptides as antihypertensive agents. KEYWORDS: Angiotensin I-converting enzyme; Bioactive peptides; Hypertension; Renin; Enzymatic protein hydrolysates INTRODUCTION Hypertension is a controllable risk factor for developing cardiovascular disease and a major global public health concern. The prevalent treatment and management strategy against severe cases of hypertension involve the use of synthetic antihypertensive drugs, but the various side effects associated with therapeutic use of these drugs supports the need to discover alternative approaches to treatment and management of hypertension. The strategic use of food-derived natural compounds against molecular disease targets can provide safe and effective modulation of aberrant human health processes and diseases. Consequently, food protein-derived bioactive peptides (BAPs) have emerged as safer health-promoting agents that can be used to manage hypertension in humans. These peptides are liberated from native food proteins by specific and non-specific enzymatic proteolysis, and have shown tremendous prospects in modulating key physiological processes that lead to hypertension depending on their bioavailability in target tissues. This paper reviews the literature on the prevalence of hypertension in various populations as well as the molecular and clinical aspects of intervention against hypertension using BAPs, based mainly on modulation of the renin angiotensin system (RAS) pathway. Current research on the safety and bioavailability of BAPs in target cellular locations, and potential application as functional food ingredients for prevention and management of hypertension are also discussed. Definition and Classification of Hypertension Hypertension is currently defined by the presence of a sustained elevation of systemic arterial pressure above systolic (SBP) and diastolic blood pressure (DBP) ratio of 140/90 mmHg. It is usually induced by physiologic and/or psychologic stressors. Hypertension is a progressive cardiovascular syndrome that results from an array of distinct but interrelated etiologies.1 The sustained elevation of blood pressure (BP) is usually sequel to the presence of early markers of the disease. Hypertension is the most common non-communicable disease in the world.2 It is also the world’s leading cause of cardiovascular diseases.3 This is largely because the progression of hypertension is strongly associated with cardiac and vascular abnormalities that negatively affect the functions and structures of target organs like the heart, kidneys, brain, vasculature, etc, leading to premature and high levels of morbidity and mortality.1,4 The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, in its most recent report (JNC 7 report) classifies BP into four categories – normal, prehypertension, stage 1 hypertension and stage 2 hypertension.5 Normal BP (<120/80 mmHg) is described as a case of blood pressure elevations and the absence of any identifiable cardiovascular disease. Prehypertension (120/80–139/89 mmHg) is characterized by occasional or intermittent blood pressure elevations and early cardiovascular disease. Stage 1 hypertension (140/90–159/99 mmHg) is defined as a case of sustained blood pressure elevations or progressive cardiovascular disease. It comes with overt early disease markers and early signs of target organ disease. This stage develops as a result of persistent structural and functional alterations in blood pressure control mechanisms. Stage 2 hypertension (≥160/100 mmHg) is characterized by a marked and sustained blood pressure elevation or advanced cardiovascular disease. Cardiovascular disease risk factors, early disease markers and target organ disease are not only present, but are also progressive with or without cardiovascular disease events. The advanced stage of the hypertension continuum is exacerbated by aging, BP elevations and persistent disease risk factors.1,5 Epidemiology Risk factors Elevated BP is the single most important modifiable risk factor for hypertension. Randomized trials have established that reducing BP can prevent cardiovascular events, especially stroke.6,7 Overweight and obesity are the next important modifiable risk factors for hypertension.8,9 The strongest risk factor for incident hypertension is overweight/obesity and both are independent and significant predictors of the level of blood pressure.10 In fact, according to the JNC report,5 a 10 kg weight loss promotes a 5 to 20 mmHg reduction in blood pressure. A western-styled diet – high fat, high sugar, low fibre diet – is another modifiable risk factor for hypertension. The Dietary Approaches to Stop Hypertension (DASH) trial illustrated for the first time that dietary intervention alone (using the DASH diet that is low in fat, low in sugar, and high in fibre among others) significantly lowers SBP and DBP by an average of 11.4 and 5.5 mmHg in hypertensive subjects and by 3.5 and 2.1 mmHg in non-hypertensive subjects, respectively.11 The above magnitude is comparable to that achieved by mono-pharmacotherapy for mild hypertension. Moreover, there is considerable scientific evidence linking high sodium intake (consumed as table salt) to hypertension and increased cardiovascular events,12 whereas a high intake of potassium, calcium and magnesium reportedly has a BP-lowering effect.10,11 Furthermore, there is a direct dose-response relationship between alcohol consumption and hypertension. This is more so when alcohol consumption is in excess of 2 drinks per day.13 The reduction of alcohol consumption to less than 2 drinks a day can lower blood pressure by up to 4 mmHg.14 Physical inactivity is also a modifiable risk factor for hypertension. There is an established inverse relationship between physical activity level and blood pressure, and higher physical activity levels reduce the risk of hypertension by about 15%.15,16 The major non-modifiable risk factors for hypertension are age, gender and genetics. Hypertension and cardiovascular events occur more frequently during and after age 50 years. Hypertension is however thought to originate in childhood and adolescence and tracks into adulthood.17,18 The hypertension risk advantage that premenopausal women have, and lose after menopause is thought to be linked to hormones involved in renal salt handling.19 Sex differences in the frequency of hypertension is put at 4% in the United States, 8% in Canada and 11% in Western Europe.20 However, from age 61 years onwards, the prevalence of hypertension becomes higher in women than in men.21 The prevalence of hypertension from a racial/ethnic point of view is highest among African Americans. Hypertension in blacks is more prevalent (though the incidence of hypertension has been shown to differ between blacks and whites only before age 74 years)22, and more severe, starts earlier in life, and has higher target organ morbidity.23 Blacks have higher peripheral vascular resistance, greater salt sensitivity and lower circulating levels of renin. About 30% of all deaths among African Americans are attributable to hypertension.24 Conversion from prehypertension to hypertension is also accelerated in blacks25 Other identifiable causes of hypertension include sleep apnea, drug induced or related causes, chronic kidney disease, primary aldosteronism, renovascular disease, chronic steroid therapy and Cushing’s syndrome, pheochromocytoma, coarctation of the aorta, and thyroid or parathyroid disease.5 Prevalence of hypertension Kearney et al.3 reported that 26.4% of the adult population (26.6% of men and 26.1% of women) in 2000 had hypertension and 29.2% (29.0% of men and 29.5% of women) were projected to have this condition by 2025, an increase to a total of 1.56 billion people. Accordingly, the total number of adults with hypertension in 2000 was estimated at 972 million; 333 million in developed countries and 639 million in developing countries. The global hypertension prevalence is reportedly lowest in rural India (3.4% in men and 6.8% in women) and highest in Poland (68.9% in men and 72.5% in women).2 In the United States, the prevalence of hypertension increased from 23.9% in the period 1988-1994, to 28.5% in the period 1999-2000, and to 29% in the period 2007-2008.26 A recent report put the figure for American adults with elevated blood pressure requiring treatment, at 150 million (32%).27 An analysis of data from the Canadian Heart Health Surveys (CHHS) reported a prevalence of 21.1% for Canadians aged 18-74 years.28 A very recent report29 shows that the prevalence of hypertension in Canada has been fairly stable (19.7% to 21.6%) between 1992 and 2009. The latter report shows that 21.6% of the adult population (25.5% of men and 17.8% of women) in 1992 had hypertension; 21.3% (23.8% of men and 19.0% of women) had the disease in 2006; while 19.7% (19.9% of men and 19.4% of women) had hypertension in 2009. In sub-Saharan Africa, the prevalence of hypertension is higher in the urban areas compared to the rural areas. Hypertension is nevertheless age-dependent irrespective of place of domicile. A review by Addo et al.30 shows that the prevalence of hypertension (using the JNC 7 criteria) was lowest in rural Nigeria and Eritrea (14.5% each) and highest in urban Tanzania (39.1% for women and 37.3% for men). The prevalence of hypertension in Nigeria has risen from 10% in 198731 to 17-20% in 199932 and 32.8% in 2010.33 The small sample size of the last mentioned study33 especially in the rural areas (n = 370), however, warrants a cautious comparison of the data to larger studies. There is yet (to our knowledge) no standardized nationally representative study of hypertension in Nigeria. In Ghana, the prevalence of hypertension has risen from 2-5% in 197334 to 28.7% in 200335 and 25.4% in 2006.36 In a recent review of more than 70 published studies on hypertension in Ghana, it was reported that “most studies reported a crude prevalence of hypertension between 25% and 48% using the newer threshold of 140/90 mmHg” and “only four studies reported a prevalence of less than 20%”.37 Hypertension is without doubts, a very important global public health problem that cuts across ethnic and geographic differences, albeit to varying degrees. Physiological Blood Pressure Regulation and Hypertension As with other cellular processes, the human physiological processes possess strong regulatory mechanisms for controlling vascular tone and BP. The renin-angiotensin system (RAS) and the kinin-nitric oxide system (KNOS) are the major pathways for physiological BP regulation. As shown in Fig. 1, in the RAS pathway, angiotensinogen is hydrolyzed to release a decapeptide angiotensin (AT)-I by the cleavage of the C-terminal of Leu10 located at the C-terminal region of the protein in the rate limiting step catalyzed by renin (E.C. 3.4.23.15; produced by renal cells). Mature renin is a 37 kDa 340 amino acid-residue enzyme that belongs to the aspartate protease family, uniquely characterized by the presence of two Asp residues in their active sites. In the second step of RAS, AT-I is converted to a potent octapeptide vasoconstrictor, AT-II, by cleavage of His-Leu from C-terminal by zinc metallopeptidase, angiotensin I-converting enzyme (ACE; E.C. 3.4.15.1), which is produced predominantly in the lungs.38 Subsequently, AT-II binds its receptors to trigger a physiological cascade that induces vasoconstriction, aldosterone secretion, salt reabsorption and water retention.38 On the other hand, the KNOS pathway plays a role in the regulation of bradykinin (a vasodilator), which elicits physiological processes that lead to increased intracellular Ca2+ that forms a complex with calmodulin to activate endothelial nitric oxide synthase (NOS), which catalyzes the synthesis of nitric oxide (NO) from L-arginine; NO is responsible for the vasoregulatory effect of bradykinin.38,39 In addition to AT-II synthesis, ACE also catalyzes the hydrolysis of bradykinin into inactive fragments leading to additional effects in BP elevation (Fig. 1). Excessive enzymatic activity due to over-expression of ACE can lead to elevation of BP followed by hypertension. Thus, the modulation of physiological ACE activity has since been exploited towards the discovery of antihypertensive agents (e.g. captopril) because its inhibition in hypertensive subjects will lead to decreased AT-II and elevated bradykinin concentrations with concomitant decrease in BP. Moreover, the inhibition of ACE activity does not guarantee effective reduction of elevated BP during hypertension because formation of vasoactive AT-II can also occur in some tissues via ACE-independent pathway catalyzed by chymase, tonin or cathepsin.38,40,41 Consequently, the inhibition of renin activity with drugs (e.g. aliskiren) has been developed as a more effective and selective approach towards treatment and management of hypertension.41 Modulation of the Renin-Angiotensin System by Bioactive Peptides (BAPs) BAPs-induced ACE inhibition The activity of ACE has been widely targeted for antihypertensive therapy. The use of peptides as ACE inhibitors was first reported for insect venom peptides 42,43 and these reports were followed by numerous studies that discovered ACE-inhibiting peptides from an enormous list of proteins from plant, animal and marine sources (see review articles by Hartman & Meisel44 and Udenigwe & Aluko45). Fig. 2 shows a schematic representation of the processes involved in the production and characterization of BAPs from food proteins and evaluation of their relevant biological properties. Of particular interest to several research groups are the milk-derived tripeptides or lactotripeptides (LTPs), IPP and VPP, derived from β-casein (f74-76 and f84-86, respectively), which have been widely evaluated for antihypertensive properties due to their potent ACE-inhibitory activities (IC50 of 5 and 9 µM, respectively).46 The LTPs were liberated from β-casein during fermentation with Lactobacillus helveticus and Saccharomyces cerevisiae.46 Other ACE inhibiting BAPs have been derived from fish and egg proteins but the abundance of plant proteins provides an advantage over animal proteins as sources of BAPs. In addition to purified peptides, crude enzymatic protein hydrolysates have also shown ACE-inhibitory properties, and their use as antihypertensive agents is encouraged to reduce cost and labour-intensive peptide purification steps. However, the use of peptide mixtures in modulating ACE activity might not lead to potent activity due to the possible low abundance of the active principles within the mixture. Marine-derived proteins have shown excellent potential due to the large amount of processing by-products, and these underutilized products are now exploited as sources of ACE inhibiting BAPs.47 For example, Alcalase-catalyzed hydrolysis of Atlantic salmon collagen followed by RP-HPLC purification resulted in the isolation of dipeptides (AP and VR), which inhibited ACE activity with IC50 of 0.06 and 0.33 mg/ml representing 20- and 4-fold enhancement, respectively compared to the activity of the crude hydrolysates48; this highlights the need for extensive purification for increased potency of BAPs. A comprehensive library of food protein-derived ACE-inhibiting peptides can be found in BIOPEP database (http://www.uwm.edu.pl/biochemia/index.php/en/biopep). In fact, a bioinformatic-based approach using the BIOPEP program can be used for production of potent ACE inhibitors by in silico hydrolysis of primary sequence of the proteins for optimization of the enzymatic process. This approach showed excellent potential in identifying appropriate proteolytic enzymes and food protein raw materials, based on preponderance of active peptide sequences within the primary structure of the protein49; however, the use of this approach is limited to proteins with known primary sequence, and sound knowledge about the structure-function properties of peptides is often required. Since most points in evidence on the ACE-inhibitory activities of BAPs are based on in vitro evaluations, there are concerns as to whether the observed interactions between ACE and BAPs can be replicated in vivo especially for unstable and poorly absorbed BAPs. BAPs-induced renin inhibition Recent studies have shown evidence that some food protein-derived BAPs possess the ability to inhibit renin activity. The initial study demonstrated that low molecular size peptides derived from enzymatic hydrolysis of flaxseed proteins exhibited low to moderate renin-inhibitory activities via mixed-type inhibition pattern, possibly due to multiple interactions of renin with various components of the peptide mixtures.50 The fact that these BAPs showed multifunctional property by inhibiting both renin and ACE activities suggests possible in vivo potency as antihypertensive agents. Similar studies have also reported the release of renin inhibitors (IC50 0.81 mg/ml) by simulated gastrointestinal digestion of hempseed proteins with pepsin and pancreatin51, which indicates that beneficial BP-reducing effects can potentially result from consumption of native hempseed proteins depending on bioavailability of the resulting BAPs. Furthermore, a number of dipeptides have been identified from a pea protein hydrolysate fraction as renin inhibitors45,52, including dipeptides IR, KF and EF with IC50 values of 9.2, 17.8 and 22.6 mM, respectively.52 The wide range of activities observed for these peptides and their distinct structural properties provided a platform for the study of their structure-function relationships, and it is expected that such studies will provide fundamental knowledge of inhibitory mechanisms and peptide templates for the design of peptidomimetics with enhanced potency and bioavailability. Structural requirements of BAPs for inhibition of RAS enzymes The mechanism of ACE inhibition by BAPs has been studied using both synthetic and natural peptides. Most ACE-inhibiting BAPs exert their activities by competitive inhibition but some peptides have also exhibited non-competitive (e.g. LW and IY) and uncompetitive (e.g. IW and FY) inhibition.53,54 Structural properties such as chain length, steric properties, net charge and hydrophobicity constitute important factors that determine potency of BAPs in inhibiting ACE.55 Consequently, detailed knowledge of the structure-activity relationship of BAPs can enhance the discovery of more potent BAPs. It was earlier proposed that ACE inhibition by BAPs involves three circular hydrophobic clefts located at ACE catalytic site, which were designated as the major sites for interaction of C-terminal residues of BAPs.56 This implies that BAPs containing hydrophobic amino acid residues could effectively bind these hydrophobic pockets, depending on structural conformation, where they are held together by hydrophobic interaction. As a result, it was observed that most competitive ACE-inhibiting BAPs contain hydrophobic amino acid residues in their sequence.53,56 Quantitative structure-activity relationship (QSAR) studies have been conducted in attempt to elucidate the structure-function properties of BAPs. The prevalent method utilizes a chemometric approach – the partial least squares projection of latent structure (PLS) – to design models that relate bioactivity data to the physicochemical properties of BAPs. Using the z-scale amino acid descriptors (z1, hydrophobicity; z2, molecular size/steric effects; z3, electronic properties), a library of BAPs was used to develop PLS models that showed that, for di- and tripeptides to exhibit potent ACE inhibition, the C-terminal amino acid residues must be hydrophobic and bulky (e.g. Phe, Trp, Pro, Tyr) whereas the N-terminal amino acid residues should preferably be aliphatic (e.g. Ile, Leu, Val).57 Typical examples of BAPs with such structural features include potent antihypertensive LTPs, which possess N-terminal Ile or Val and C-terminal Pro residues. Moreover, for oligopeptides with four or more (up to 10) amino acid residues, other QSAR PLS models demonstrated that the last four amino acid residues at the C-terminal of the peptides should be hydrophobic for potency and that these residues play major roles in determining the ACE–inhibitory activities of these peptides.58 These findings indicate that the ACE-inhibiting BAPs with strong hydrophobicity act possibly by interacting with the hydrophobic pockets of the catalytic site of the enzyme. Using short peptide fragments derived from ACE-inhibiting decapeptide (VTVNPYKWLP), the presence of Trp (W) in BAPs has been demonstrated to promote ACE inhibition59 possibly based on hydrophobicity and steric effects. Although there is a strong positive correlation between hydrophobicity and bitterness of BAPs, a limiting factor in nutraceutical application of BAPs, there was no significant statistical relationship between bitterness property and ability of di- and tripeptides to inhibit ACE60; therefore, the low-molecular size peptides can potentially be incorporated into health-promoting functional foods with little concern about negative sensory quality. As with ACE inhibition, a recent QSAR study reported similar structural requirements for dipeptide inhibitors of renin although there is no similarity in the primary and 3-dimensional structures of ACE and renin, and no correlation was observed between the activities of the peptides in inhibiting the two RAS enzymes.45 In fact, similarity in structural requirements increases the feasibility of using a single peptide (e.g. IW) to modulate the activities of both ACE and renin leading to more pronounced reduction in BP compared to peptides that inhibit the activity of only ACE or renin.45,53 Animal Studies with Antihypertensive BAPs Spontaneously hypertensive rats (SHR) have been widely used as animal model of essential hypertension for studying the BP-lowering effects of BAPs. The LTPs (IPP/VPP) independently lowered elevated SBP by maximum values of 28.3 and 32.1 mmHg, respectively, in SHR; several other bovine casein-derived peptides with 2−12 amino acids in their sequence induced ΔSBP ranging from −2 to −34 mmHg with the maximum activity displayed by αS1-casein-derived FFVAPFPEVFGK (f23−34).61 These effects on BP were attributed to ACE inhibition by the BAPs; moreover, calcium present in fermented milk products has been suggested to promote BP-lowering effect of the BAPs product in SHR.62 Apart from the lactopeptides, a pea protein-derived peptide product demonstrated both short-term BP reduction in SHR following oral gavage (ΔSBP, −19 mmHg after 4 h) and long-term effects in hypertensive chronic kidney disease (Han:SPRD-cy) rats (SBP, −29 mmHg; DBP, −25 mmHg after 8 wks) although the peptides were poorly active during in vitro evaluation.63 In the Han:SPRD-cy rats, the pea peptide product induced reduction of renal renin mRNA expression and plasma AT-II level but showed no effect on renal expression of ACE or plasma ACE activity.63 This pattern of activity indicates that the pea-derived BAPs modulated renin, not ACE, thereby reducing the amount of AT-II with concomitant lowering of elevated BP in the hypertensive rats. Moreover, other studies have reported substantial BP-lowering effects of crude enzymatic hydrolysates of hempseed51, apricot almonds64, soy, wheat gliadin, casein, and whey65 after short-term oral gavage of the products to SHR (Table 1). Despite the potent antihypertensive activities of the food-derived BAPs in animals, these data cannot be directly applied to hypertensive humans due to complexity of the human physiology; thus, BP-lowering potential of BAPs needs to be evaluated in hypertensive humans prior to health claims and commercialization of the products. TABLE 1 Short-term maximum systolic blood pressure (SBP)-lowering activity of BAPs-containing enzymatic protein hydrolysates in spontaneously hypertensive rats
Human Clinical Trials with Anti-hypertensive BAPs Physiological BAPs-induced inhibition of ACE and renin activities during hypertension will ultimately result in decrease in the amount of circulating AT-II, and increased amount of bradykinin; and these would consequently lead to decrease in elevated BP. Several human clinical trials have shown evidence that BAPs in fermented milk possess antihypertensive effects in human subjects with mild hypertension.70-72 A recent study reported that consumption of milk protein hydrolysates enriched with the LTPs, IPP/VPP, induced −3.8 and −2.3 mmHg change in SBP and DBP, respectively, in prehypertensive and stage 1 hypertensive subjects using office BP measurements.73 Moreover, no significant decrease in BP was observed in the study in prehypertensive subjects compared to placebo indicating that substantial BP elevation is prerequisite for the antihypertensive effects of the peptides. Moreover, LTPs-based peptide product (AmealPeptide) was found to induce decrease in daytime ambulatory SBP (−3.6 mmHg) and mean 24-h SBP (−2 mmHg) in treated and newly diagnosed (treatment-naive) stage 1 and stage 2 hypertensive subjects that consumed a 150-mg dose of the product daily for 6 wks; more pronounced effects on daytime SBP was observed for treatment-naive subjects compared to placebo.74 Apart from milk-derived peptides, plant protein-derived BAPs have also shown prospects for management of human hypertension. In hypertensive humans, a pea protein-derived peptide product was recently reported to have reduced SBP by 6 mmHg after 3 wks of treatment with 1.5 g/day of the peptides consumed with orange juice as delivery vehicle.63 Although studies have demonstrated correlation between BAPs-induced BP reduction and decreased activity of plasma RAS enzymes or amounts of vasoactive peptides75, there is evidence that the antihypertensive activity of certain BAPs occurred without changes in renin activity, AT-I or AT-II levels.73 Thus, there may be alternative routes for BP lowering by BAPs other than RAS modulation. For example, amaranth protein-derived BAPs with in vitro ACE-inhibitory activity was found to induce activation of endothelial NOS by phosphorylation at the Ser117 residue leading to smooth muscle relaxation in isolated rat aortic segments76; the observed effect was due to the synthesis of vasodilator, NO, that mediates lowering of BP during hypertension. In contrast, some studies have reported lack of substantial BAPs-induced decrease in elevated BP. In a multicentre crossover study with untreated hypertensive white subjects (n=162), Van Mierlo and co-workers77 reported that LTPs (IPP/VPP) administered in form of dairy drink did not significantly affect mean 24-h ambulatory BP compared to placebo. Likewise, administration of LTPs-containing fermented milk or placebo to 94 prehypertensive and borderline hypertensive subjects daily for 8 wks did not result in any significant difference in SBP and DBP between the groups.78 Actually, the latter study observed that the slight change in BP due to the LTPs was not better than BP decreases that result from lifestyle intervention for lowering BP, which raises concerns with respect to balance between cost and efficacy/benefits of the BAPs. The contrasting findings on BP-lowering effects of BAPs can be attributed to a number of factors including genetic, dietary and lifestyle variations in the different populations, study design, vehicle of delivery of the peptides and mode of BP measurement. Therefore, there is need to develop standardized protocols for clinical intervention trials with BAPs and precise tools for BP measurements (e.g. ambulatory BP measurement) for comparison of data conducted in various locations. To the best of our knowledge, there is dearth of literature information on studies that evaluated the potential use of food-derived BAPs for the management of hypertension in an African population; this approach towards the reduction of elevated BP is encouraged considering the abundance of potential raw materials on the African continent for the production of BAPs. Meta-analyses of Clinical Trials TABLE 2 Summary of meta-analyses of placebo-controlled clinical trials conducted with food protein hydrolysates and peptides in human subjects with different stages of hypertension
Due to conflicting results from human intervention studies with food-derived peptides, meta-analyses of several placebo-controlled trials have been conducted to confirm the presence or absence of BP-lowering effects by the peptides. As shown in Table 2, meta-analyses of human clinical trials showed that food protein hydrolysates and peptides have the ability to reduce both SBP and DBP in subjects with different stages of hypertension. As much as −5.13 and −2.4 mmHg change in SBP and DBP, respectively were observed in 423 subjects with high-normal BP or mild hypertension after receiving various enzymatic protein hydrolysates and peptides derived from milk (LTPs) and fish.81 These values are encouraging since −5 and −2.5 mmHg change in SBP and DBP, respectively can reduce the risk of coronary artery disease and stroke by 12% and 20%, respectively, irrespective of the mode of intervention.7 Moreover, it was demonstrated that the LTPs showed more pronounced reduction of BP in hypertensive subjects compared to those with mild cases of hypertension.80 This observation indicates that the BAPs may have modulated the increased levels of BP-regulating molecules with little or no effect on their basal levels. In addition, Cicero and co-workers79 reported based on meta-analysis that efficacy of the LTPs in lowering elevated blood pressure is dependent on ethnic factors, since Asian subjects (ΔSBP, −6.93 mmHg; ΔDBP, −3.98 mmHg) were found to be more responsive to the BAPs-based intervention than Caucasian subjects (ΔSBP, −1.17 mmHg; ΔDBP, −0.52 mmHg). This discrepancy could be attributed to genetic variation or different dietary lifestyles of the populations; however, there is need to conduct appropriate studies to explain these responses. Furthermore, LTPs-induced BP-lowering effects in human subjects were observed to be independent of baseline BP, treatment duration, peptide dose and age of subjects.79 BAPs-based interventions in some populations clearly show prospects for the control of hypertension and associated vascular disease since the slight BP reduction induced by the potent peptides can be combined with lifestyle modification practices to potentially produce substantial reduction in elevated BP during hypertension. Bioavailability and Safety of Food-derived Antihypertensive Peptides Oral consumption of BAPs increases their susceptibility to degradation into inactive fragments by gastrointestinal, brush border and serum peptidases. Therefore, antihypertensive BAPs must withstand proteolytic inactivation and be absorbed through the enterocytes into circulation in order to exert their BP-lowering effects during hypertension. There is considerable evidence that antihypertensive di- and tripeptides are absorbed intact in humans83-85 since their transepithelial movement can be facilitated by peptide transporters (PepT) that are expressed in enterocytes; small oligopeptides can sometimes escape peptidolysis and cross the enterocytes through hydrophobic regions of intestinal membrane epithelia or tight junctions.86 After consumption of yogurt containing the antihypertensive LTP by normotensive subjects, IPP was detected in nanomolar concentrations in the plasma of subjects indicating efficient absorption and bioavailability.83 In addition to chain length, other factors that influence bioavailability include charge, lipophilicity and solubility of BAPs.86 Based on the literature, food protein-derived BAPs are considered safe for human consumption since studies in animals and human subjects demonstrated lack of adverse effects of the peptides compared to placebo. For example, Anadon and co-workers demonstrated that a single dose of 2000 mg/kg BW and repeated daily doses of 1000 mg/kg BW (higher than typical therapeutic doses) of antihypertensive lactopeptide (αs1-casein f90–94 and f143–149)-containing hydolysates had no negative effects on clinical parameters and mortality in rats.87 Moreover, LTP-rich products were reported to have no significant adverse effects on serum and urine chemistry in prehypertensive and hypertensive human subjects compared to placebo.73,74 It appears that BAPs also showed no adverse effect in normotensive subjects.85 These points in evidence indicate that food protein-derived antihypertensive BAPs are safer for human consumption compared to synthetic antihypertensive drugs. Commercial BAPs-based Antihypertensive Products A number of BAPs-based food products with antihypertensive properties have been commercialized and marketed by international food companies. Table 3 shows a list of some of these products, their food sources and, in some products, the sequence of the active peptides. Most of the peptide products are derived from milk proteins; Calpis AMEEL and Evolus are formulated with LTPs (IPP/VPP) whereas BioZate and Peptide Soup are composed of a mixture of peptides.44 These BAPs products have demonstrated a wide range of BP-lowering activity in hypertensive human subjects in certain populations with ΔSBP of −4.5 to −14.9 mmHg and ΔDBP of −3.6 to −8.8 mmHg.61 TABLE 3 Commercial antihypertensive peptide productsa
Conclusion Based on available evidence, there are prospects in the use of food-derived BAPs and protein hydrolysates for the management of hypertension in some human populations although contradictory evidence indicates otherwise in other populations. The mild BP-reductions observed for these peptide products are generally lower than the activity of antihypertensive drugs but the natural form of food protein-derived BAPs can promote their use as safe antihypertensive agents. Moreover, future studies are needed to elucidate the long-term systemic molecular interactions of antihypertensive BAPs with the human genome, proteome and other cellular processes to ensure absolute safety, and possibly to explain the observed variation in potency of the peptides in different populations. It would also be economically beneficial to discover approaches that will yield high amounts of crude protein hydrolysates with potent BP-lowering effects to obviate the need for extensive peptide purification, which may alter the natural integrity and safety of BAPs. Finally, the economic and health-promoting values of protein-rich foods and food processing by-products in African countries can be potentially increased by using these products as raw materials for the production of antihypertensive BAPs. Acknowledgement The Natural Sciences and Engineering Research Council of Canada (NSERC) is acknowledged for awarding a postdoctoral fellowship to CCU. References
Copyright © 2011 Klobex Academic Publishers The following images related to this document are available:Photo images[bk11015f2.jpg] [bk11015f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}