 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
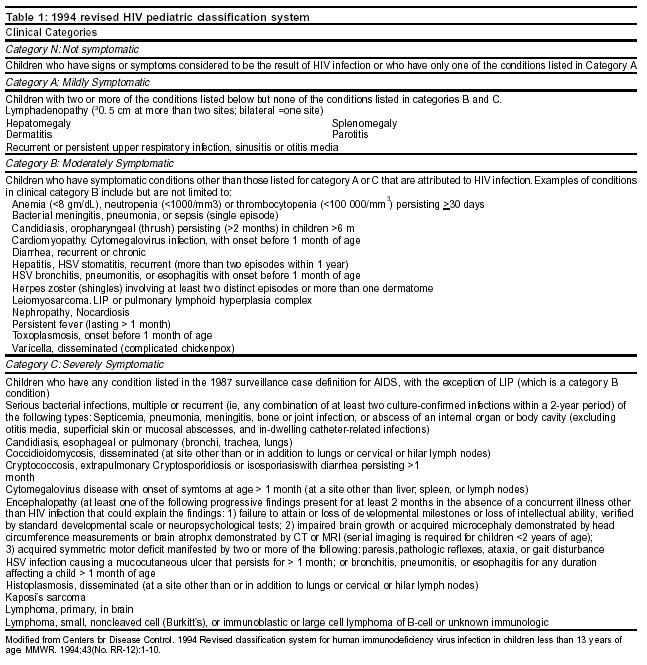
Indian Journal of Critical Care Medicine, Vol. 7, No. 4, , 2003, pp. 257-272 Review Article Pediatric Aids – Part 1 Khilnani P, Rajdev SK, Uttam R Department of Paediatrics, Indraprastha Apollo Hospital, Sarita Vihar, New Delhi - 110044, Code Number: cm03005 Abstract Much progress has been made in the therapy of pediatric HIV infection, which has been transformed from a usually fatal disease into that of a chronic disease model. Early, aggressive therapy with the goal of complete suppression of viral replication (undetectable plasma virus) should be the therapeutic goal, but this new, more hopeful environment has been created at the cost of complexity and compromises in quality of life. The rapid pace of new developments and therapeutic complexities argue strongly for care in specialized centers or, at least, frequent consultation. Principles of therapy in the pediatric intensive care unit remain unchanged. Efforts are ongoing to develop simpler, more effective therapeutic regimens that suppress and ultimately eradicate infection and that stimulate immune reconstitution and reduces need for frequent hospitalization.AIDS Definition Magnitude of the problem Opportunistic infections and other clinical manifestations of HIV disease in children Pneumocystis carinii pneumoniaHallmark opportunistic infection of Pediatrics AIDS epidemic. Known as "AIDS pneumonia" this opportunistic infection is the most common AIDS defining illness in children. PCP is an infection of early infancy and most children are affected at between 4 and 6 months of age. The risk of PCP in the first year of life for perinatally infected children not receiving prophylaxis is estimated to be approximately 12%. The revised guidelines recommend prophylaxis for all HIV infected infants, independent of CD4 count and HIV infection status starting at 4 to 6 weeks of life until 4 months of age, when a more definite diagnosis of HIV infection can be made using PCR.[1] Pathogenesis of Pneumocystis carinii infection: P. Carinii thought to be protozoan is now believed to be more closely related to fungi. P. Carinii is not easily cultured, making diagnosis dependent on the demonstration of organisms in tissues or secretions. P. Carinii establishes infection within the alveoli, where it proliferates as an extracellular parasite. Clinical and radiological presentation of PCP: Children with PCP present with a tetrad of findings; tachypnea, dyspnea, cough and fever. Physical examination findings include tachycardia and respiratory distress, accelerating tachypnea and diffuse retractions. Pulmonary auscultation is typically non specific. PCP is characerised by rapidly progressive hypoxemia. Early radiographic findings may be normal or can include hyperinflation with peribronchial thickening. As the disease progresses, the chest radiographic findings typically evolve to reveal bilateral alveolar or interstital infiltrates usually spreading peripherally from the perihilar region to involve both lung fields. Further progression results in coalescent bilateral airspace disease with air bronchogram. Less typical radiographic findings include focal or patchy infiltrates, cavities or effusions. Diagnosis The wright-geimsa procedure stains trophozoite and intracystic sporozoite forms of P. Carinii and is commonly used as rapid screening test. The Papanicolaou stain which identifies the alveolar exudates of PCP rather than the organism can be used for screening. The Methenamine silver stain and direct immuno- flouroscent staining with monoclonal antibody detect cyst forms of the organism and can be used for the confirmation of screening results. Treatment and prognosis for children with pneumocystis carinii Comprehensive respiratory support, including supplemental oxygen, ventilatory support and good pulmonary toilet is essential to ensure a satisfactory outcome for patients with this disease. Children are at risk for respiratory distress syndrome and secondary complications including pneumothorax. Characteristically oxygen requirement increases inconsistent with radiological correlation of infiltrates necessitating mechanical ventilation with high fiO2 and positive endexpiratory pressures. Secondary bacterial complications may also complicate the course of disease. Prophylaxis of PCP HIV infected children aged: All HIV infected children treated for PCP Recurrent bacterial infections In 1987, recurrent bacterial infections defined as 2 or more bacteriologically documented systemic bacterial infections including septicemia or bacterimia, meningitis, pneumonia, osteomyelitis, septic arthritis, or abscess of an internal organ or body cavity that occurred within a 2-year period were included as AIDS -defining illness for children. Recurrent bacterial infection constitute the second most common ′opportunistic cause of IDS in children. Also minor and "presumed" (those without bacteriological confirmation) bacterial infections further contribute to the clinical complexity of pediatric HIV disease.Bacteriological pathogens: Summarising the experience of many investigators, Krasinski[2] noted that the major bacterial pathogens in children with HIV were similar to those in immunologically healthy children and that the spectrum of bacterial isolates can be predicted from the site of infection or the clinical infection syndrome. Clinical manifestations Pneumonia-Although bacteremia is the most common laboratory documented bacterial infection, clinically diagnosed bacterial infections, major and minor are far more frequently diagnosed in children with HIV infection. The diagnosis of acute pneumonia was the most common clinically diagnosed severe bacterial infection. Sinusitis was found to be the second most common clinically diagnosed severe infection. Other major bacterial infections- Meningitis, osteomyelitis, septic arthritis, purulent pericarditis and periorbital cellulites have been reported in children with HIV disease. Sinusitis- Sinusitis is the second most common clinically diagnosed bacterial infection. The disease presents as a subacute or chronic indolent process and is commonly recurrent. Radiographic evaluations revealed primary involvement of the maxillary and ethmoid sinuses and one third of cases involved 2 or more sinuses. A history of nasal discharge and persistent cough for more than 2 weeks should prompt the diagnosis of sinusitis. Bacterial infections associated with central venous catheters Diagnosis and treatment of bacterial infections Prophylaxis against bacterial infections: Prophylaxis against bacterial infections should include vaccination against conjugate H. Influenze Type B vaccine during infancy and with the 23-valent polysaccharide at 2 years of age. A second dose of pneumococcal vaccine should be administered after 3 to 5 years for children less than 10 years of age and after 5 years for children more than 10 years of age. Children with recurrent bacterial infections may benefit from daily prophylaxis with TMP-SMX (150 mg/M2. TMP divided into 2 daily doses). IVIG is indicated for children with hypogammaglobulinemia (400 mg/Kg/Mo.) and should be considered for children with 2 or more invasive bacterial infections in a 1-year period especially for those who have failed or are intolerant to antibiotic prophylaxis.[4] Mycobacterium avium infection (MAC) Pathogenesis: M. Avium complex includes 2 closely related species, M. Avium and Mycobacterium Intercellulare. Mycobacteria are intracellular parasites that proliferate within macrophages. A high tissue burden can be found in organs, including lungs, liver, spleen, intestines, bone marrow and lymph nodes. Clinical presentation: Clinical presentation can be indolent and slowly progressive. Most children have a conglomeration of signs and symptoms, including fever, weight loss and poor weight gain, abdominal pain and anemia. Night sweats, diarrhea, malaise, neutropenia and hepatomegaly have also been described. Fever can be quite high 40.5°C or more and surprisingly well tolerated. Death ois generally not attributed to M. Avium infection but rather to advanced HIV disease or other infectious agents. Diagnosis of disseminated MAC infection: The diagnosis of M. Avium infection requires cultivation from blood or tissue. Blood cultures are usually done using the Bactec radiometric mycobacterial growth system which can yield a positive culture within 2 weeks. DNA hybridization with species specific probes is then used to identify the species of mycobacteria. Bone marrow and lymph nodes biopsies can be useful in the evaluation of M. Avium disease. Characteristic histologic findings of acid-fast bacilli within macrophages are highly suggestive of M. Avium infection and may hasten the start of therapy in children with a suspected diagnosis but cultures are imperative to distinguish species. Treatment of disseminated MAC infection: Monotherapy for MAC results in rapid development of resistance,so combination therapy with 2 or more drugs is indicated for the treatment of disseminated MAC infection. The initial regime for the treatment of disseminated MAC infection should include: Clarithromycin 15 mg/Kg daily in 2 divided doses; maximum 500mg or Azithromycin 10 mg/Kg once daily PO; maximum 500mg with Ethambutol 15 to 20 mg/Kg once daily PO; maximum 1600 mg and /or Rifabutin 5-10 mg/Kg once daily PO, maximum 300 mg. Ethambutol is not recommended for children less than 12 years old and may cause optic neuritis. Mycobacterium tuberculosis Clinical presentation: Although most children seem to have primary pulmonary infection, extrapulmonary disease has been reported in 10 to 50% of children with tuberculosis.[5] Most children have a history of fever and commonly, cough. Tuberculin skin test results are commonly negative in patients with advanced immunosuppression and chest radiograph findings can be variable. Children with low CD4+ counts may be at highest risk for tuberculosis, but children at all stages of HIV infection can become infected. High rates of resistance to antitubercular drugs have been reported in HIV-infected children with tuberculosis. Diagnosis: The diagnosis of tuberculosis in HIV infected children is complicated by several factors. Clinical manifestations although predominantly pulmonary, commonly involve extrapulmonary sites. For children with pulmonary tuberculosis, chest radiographs are often abnormal, but a wide array of abnormalities have been described, including diffuse interstitial disease and lobar infiltrates. Many children with tuberculosis have a history of chronic lung disease and abnormal chest radiographs further obscuring the diagnosis. A careful medical history with attention to potential household and community contacts may be the first clue to the diagnosis of this infection. The differential diagnosis for any child with pulmonary disease undergoing diagnostic evaluation should include tuberculosis. The Mantoux test, 5 tuberculin units of purified protein derivative, 0.1 ml (5 TU, PPD) should be planted; 5 mm of induration is considered a positive result in HIV infected individuals, but imperative of skin test results, specimens for cultures are imperative if a child is suspected of having tuberculosis. Samples can be obtained with gastric washings or bronchoalveolar lavage. All specimens should be cultured and antimycobacterial susceptibility should be performed on all isolates. Treatment: Investigators recommend that children with tuberculosis disease begin therapy with a 4 drug regimen consisting of Isoniazid (10-20 mg/kg/day; max 300 mg), Rifampicin (10-20 mg/kg/day; max 600 mg), Pyrazinamide (30 mg/kg/day) and Ethambutol (15 mg/kg/day) or Streptomycin (20-30 mg/kg/dayIM). Children with pulmonary disease should be treated for 6 to 12 months whereas those with extrapulmonary disease are likely to require a minimum of 12 months of therapy. Fungal infections Although systemic fungal infection are relatively rare in children with HIV disease, mucosal and cutaneous fungal infections are commonly diagnosed. Most HIV infected children develop oral candidiasis during their lifetime and many children have recurrent episodes.Candida infections Oral candidiasis: Candidiasis is acquired during passage through the birth canal and is commonly diagnosed in otherwise healthy infants. Severe oral candidiasis may be the first clinical indication of HIV infection in HIV exposed infants. Children may complaint of discomfort and decreased oral intake in the presence of candidiasis. Diagnosis may be made on inspection. Laboratory confirmation is typically unnecessary. Initial treatment should begin with topical nystatin or clotrimazole. Topical Amphoteracin B and intraoral use of vaginal suppositories may also be effective therapies. Children with recurrent disease may benefit from daily prophylaxis with fluconazole.Esophageal candidiasis Children with esophagitis complain of substernal or abdominal pain or burning and difficulty swallowing. Weight loss and oral candidiasis are common findings on physical examination. Endoscopy is generally recommended to confirm the diagnosis of candida esophagitis in children and exclude other pathogens including herpes simplex and CMV. Many clinicians treat children who have oral candidiasis and symptoms consistent with esophagitis and reserve endoscopy for cases unresponsive to therapy.Fluconazole 3-6 mg/kg (max. 200) once daily for 21 days is the treatment of choice for esophageal candidiasis. Other fungal infections Cryptococcus Neoformans, Aspergillius Sp., Histoplasma Capsulatum and Coccidiodes immitis are other fungal pathogens.Toxoplasma gondii infection CNS Infection: Headache, change in cognitive status, fever, and focal neurologic deficits are the most common clinical findings in patients with CNS toxoplasmosis. Focal neurologic deficits include hemiparesis, ataxia, cranial nerve palsies, and seizures. Diagnosis is usually based on clinical presentation, the presence of IgG antibodies, and characteristic findings on imaging studies. MR imaging and CT scanning typically reveal multiple ring-enhancing lesions located in the frontal, basal ganglia, or parietal regions. Cerebral edema is often present and commonly result in a mass effect. Treatment is typically initiated based on these findings, and the diagnosis is considered confirmed if a patient responds to therapy. Brain biopsy is the only method to provide a definitive diagnosis and is reserved for patients who fail to respond to therapy. Treatment: Therapy for toxoplasmosis in children includes sulfadiazine (85-120/mg/kg/d in two to four divided doses), pyrimethamine (1 mg/kg/d or 15 mg/m2/d as a single dose; maximum dose, 25 mg), and folinic acid (5-10 mg every 3 days). Treatment must be continued after the resolution of symptomatic disease to prevent recurrence. Investigators recommend that lifelong suppression be administered at these same doses. Herpes virus infections Cytomegalovirus infections (CMV)CMV infections is a significant cause of morbidity and mortality in HIV infected children. The most common clinical manifestations of CMV in children include chorioretinitis, esophagitis, pneumonitis and colitis. Cytomegalovirus generally occurs in HIV infected children with advanced immunosuppresion. Cytomegalovirus colitis is characterized by non specific complaints of diarrohoea , abdominal pain ,weight loss ,anemia and fever. Patients with CMV pneumonitis present with cough,shortness of breath and progressive hypoxemia. Clinical, laboratory and radiological findings are simillar to those of PCP. Demonstrations of intracellular inclusions in lung tissue or bronchoalveolar macrophage in the absence of other pulmonary pathogens supports the diagnosis of CMV pneumonitis. Treatment Varicella zoster infections Prophylaxis: HIV infected children who have not had chicken pox or shingles and who report significant exposure to varicella should receive varicella zoster imune globulin (1 vial /10 kg, 5 vials maximum) within 96 hours. Diagnosis of HIV infection in infants HIV infection can be diagnosed definitively in most infected infants by age 1 month and in virtually all infected infants by age 6 months using viral diagnostic assays. A positive virological test result (i.e. detection of HIV by culture, DNA or RNA polymerase chain reaction [PCR] indicates possible HIV infection and should be confirmed by a repeat virological test on a second specimen as soon as possible after the results of the second test become available. Diagnostic testing should be performed before the infant is 48 hours of age, at 1 to 2 months and 3 to 6 months. Testing at age 14 days may also be advantageous for early detection of infection. HIV DNA PCR is the preferred virologic method for diagnosing HIV infection during infancy. Assays that detect HIV RNA in plasma also may be useful for diagnosis of perinatal infection. HIV culture has sensitivity similar to that of DNA PCR for diagnosis of infection. However HIV culture is more complex and expensive to perform than is DNA PCR and definitive results may not be available for 2 to 4 weeks. Although use of standard and immune-complex dissociated p-24 antigens tests are specific for HIV infection and have been used to diagnose infection in children, the sensitivity is less than that of other virologic tests.Initial testing is recommended by 48 hours because nearly 40% of infected infants can be identified by this time. Blood samples from the umbilical cord should not be used for diagnostic evaluation. Repeat diagnostic evaluation can also be considered at age 14 days in infants with negative tests at birth, because the diagnostic sensitivity of virologic assays increases rapidly by age 2 weeks and early identification of infection would permit modification of antiretroviral therapy from the standard 6 week course of neonatal ZDV chemoprophylaxis to more aggressive combination antiretroviral therapy. Infants with initially negative virologic results should be retested at 1 to 2 months. With increasing use of ZDV to reduce perinatal transmission, most HIV exposed neonates will receive 6 weeks of antiretroviral chemoprophylaxis. Although antiretroviral chemoprophylaxis could theoretically affect the predictive value of HIV virologic testing, ZDV monotherapy did not delay the detection of HIV by culture in infants in PACTG 076 and has not decreased the sensitivity and predictive value of many virologic assays. HIV exposed children with repeated negative virologic assays at birth and at age 1 to 2 months should be retested at 3 to 6 months of age. HIV infection is diagnosed by two positive HIV virologic test results from separate blood samples. HIV infection can be reasonably excluded among children with 2 or more negative results, Two performed at age >1 month and one performed at age >4 months. Two or more negative HIV IgG antibody test results obtained at age >6 months with an interval of at least 1 month between tests also can be used to reasonably exclude HIV infection in children with no clinical evidence of HIV infection. HIV infection can be excluded definitively if HIV IgG antibody is negative in the absence of hypogamma-globulinemia at age 18 months and if the child has both no clinical symptoms of HIV infection and negative HIV virologic assays. Immunologic parameters in children Clinicians interpreting CD4+ T lymphocyte number in children must consider age as a variable. CD4+ T lymphocyte count and percentage values in healthy infants who are not infected with HIV are considerably higher than those observed in uninfected adults and slowly decline to adult values by age 6. A pediatric clinical and immunologic staging system for HIV infection has been developed that includes age-related definitions of immune suppression [Table - 1].[8] Although the CD4+ absolute number that identifies a specific level of immune suppression changes with age, the CD4+ percentage that defines each immunologic category does not. Thus, a change in CD4+ percentage, not number, may be a better marker to identify disease progression in children. In infected children and adults, CD4+ cell count declines as HIV infection progresses, and patients with lower CD4+ cell counts have a poorer prognosis than do patients with higher counts. Because knowledge of immune status (i.e. CD4+ T lymphocyte count and percentage) is essential when caring for HIV -infected infants and children, CD4+ T -lymphocyte values should be obtained as soon as possible after a child has a positive virologic test for HIV and every 3 months thereafter. The CD4+ T lymphocyte count or percentage value is used in conjunction with other measurements to guide antiretroviral treatment decisions and primary prophylaxis of PCP after age 1 year. Medical management of HIV disease in children Efforts are shifting from caring for children with advanced immunosuppression and severe opportunistic infections to early "Highly Active Anti Retroviral Therapy" (HAART), maintenance of the immune system, and prevention of opportunistic infections. Physicians who have been working with this population have observed a dramatic improvement in the quality of life and length of survival of these patients. Unfortunately, this progress is not shared by developing countries where resources are minimal and antiretroviral agents are commonly unavailable. Although efforts to develop a vaccine to prevent HIV infection are ongoing, progress has been slow. Education and awareness continue to be the most powerful weapons against HIV. Pediatric HIV infection in the United States has evolved from a rapidly progressive, fatal disease in the early years of the epidemic to a chronic infection with prolonged survival. Many children with perinatally acquired infection survive to 8 years of age and older. Management of infants at risk for HIV infection Obstetric standards and published guidelines strongly recommend offering HIV testing to all pregnant women[9] This allows women to become informed about HIV, receive care for their disease, and participate in decision making regarding mode of delivery and chemoprophylaxis to reduce the risk for the perinatal transmission of HIV. These women and their families should be counseled about the schedule of care visits; diagnostic testing for HIV; and chemoprophylaxis with zidovudine (ZDV) and trimethoprim-sulfamethoxazole (TMP-SMX), which are recommended for at-risk infants [Table - 2].[10],[11] A DNA polymerase chain reaction for the detection of HIV is recommended before hospital discharge. Diagnostic tests for HIV in the infants detects 30% to 50% of infected infants at birth, with more than 95% diagnosed by 2 months of age, so physicians should follow up these infants closely during the first several months of life. Their mothers should be counseled against breast-feeding their infants because of the additional risk for transmission of HIV to infants. If the HIV DNA PCR was not done at birth, it is performed at this visit. During the second visit, at 6 weeks of age, ZDV is discontinued if the HIV DNA PCR tests have been negative. At this visit, complete blood count, T-cell subsets, and DNA HIV PCR results are obtained. TMP-SMX is begun at a dose of 150 mg/m2/dose given three times a week for prophylaxis against Pneumocystis carinii pneumonia (PCP), and the first set of immunizations is given. PCP prophylaxis is started empirically in at-risk infants less than 1 year of age, independent of the CD4+ cell count and percentage, because HIV status may be uncertain and, in infected infants with rapid progression of disease, CD4+ cell counts can decrease precipitously in the first months of life, predisposing to PCP. At-risk infants are seen at 4 and 6 months of age for routine care and immunizations and appropriate immune and diagnostic tests. When an at-risk infant has had two negative HIV DNA PCR test results after 2 months of age and is clinically and immunologically normal, PCP prophylaxis is discontinued. These children are considered presumptively HIV negative, but an HIV enzyme-linked immunosorbent assay test is performed after 1 year of age to monitor for the disappearance of maternal antibody. If the HIV enzyme-linked immunosorbent assay and western blot are negative, the ELISA test is repeated and, if the result is negative, the child is considered uninfected and a seroreverter. Care of HIV-infected children Children with HIV should receive routine pediatric care and monitoring of their HIV disease status. Experts recommend that HIV-infected children have consultation with an HIV specialist. HIV-infected children should be seen at least every 3 months. The medications should be reviewed, doses adjusted for growth, and compliance assessed. Children should be assigned a classification [Table - 1] and laboratory studies done to monitor the immunologic and virologic status of the disease. outlines the clinical and laboratory studies and assessments that should be done at baseline and thereafter at periodic intervals. These studies are done to identify any acute problems and to assess the risk for opportunistic infections or other HIV-related complications and monitoring for medication side effects. Studies have shown that prognosis in children is related independently to viral burden and immune status.[12] Also, a direct relationship exists between the development of certain opportunistic infections and the degree of immune suppression.Complications AnemiaAnemia in patients with HIV is multifactorial. The most common causes include nutritional deficiencies; iron; folic acid; and, less commonly, vitamin B12; immune hemolysis; hemorrhage; drug toxicities; and bone marrow suppression caused by the HIV virus, other infectious agents, or malignancy. Anemia with few or absent reticulocytes is common. When secondary to iron deficiency, iron sulfate at 6 mg/kg/d of elemental iron is usually sufficient to correct the hemoglobin level, but sometimes the solution is not that easy. If the erythropoietin level is less than 500 IU/L, a trial of erythropoietin at 100 U/kg/dose, three times a week, is suggested. On the other hand, if the erythropoietin is more than 500 IU/L, no evidence of iron, vitamin B12 or folic acid deficiency is present, and the patient is reticulocytopenic, alternative diagnoses need to be investigated. Parvovirus B-19 infection can cause an aplastic anemia with a low or absent reticulocyte count and normal or high erythropoietin levels. If this infection is confirmed, IV immunoglobulin (IVIG), 1 g/kg/dose for 5 to 10 days, should be administered. This initial therapy is followed by monthly doses of IVIG at 400 mg/kg/dose. Another common opportunistic infection that causes bone marrow suppression and anemia is disseminated infection with Mycobacterium avium complex (MAC) infection. When a specific cause for anemia cannot be elucidated, a bone marrow aspiration may be necessary. Neutropenia Thrombocytopenia Intervention is not required, especially if the platelet count exceeds 50,000 platelets/mL. In some cases, the thrombocytopenia has responded to the initiation or change of antiretroviral therapy. ZDV has been shown to be beneficial in the treatment of patients with thrombocytopenia. The role of other antiretroviral agents is less clear. When the platelet count is less than 20,000 platelets/mL or when bleeding is present, treatment should be instituted. Platelets are short-lived cells, and transfused platelets have even a shorter life span. The use of platelet transfusions is reserved for patients who are actively bleeding. IVIG has been beneficial in the treatment of immune thrombocytopenia. A total of 2 g/kg is administered over 2 to 4 days. If a response to the IVIG occurs, then this is given at 3-week or 4-week intervals. If a patient has maintained a normal platelet count for 6 to 12 months, the interval between doses is increased, and the treatment is eventually discontinued. Corticosteroids are another alternative treatment. Prednisone is usually started at a dose of 2 mg/kg/d for 2 to 4 weeks and then tapered and discontinued, but the thrombocytopenia may relapse when the steroids have been discontinued. Interferon alfa is reported to be effective in patients with severe thrombocytopenia that is resistant to antiretroviral therapy. Splenectomy is an option to consider if other treatments fail and usually results in the resolution of thrombocytopenia, but the lack of a spleen will predispose these children to encapsulated bacterial infections. Gastrointestinal complications The occurrence of ulcers in the oral cavity presents a diagnostic dilemma because viral infections, such as HSV, CMV, and Coxsackie A infection, as well as bacteria, may be causative agents. Biopsy and culture of lesions that are persistent or increasing in size or number is recommended. Cultures are tested for viral, bacterial (aerobic and anerobic cultures), mycobacterial and fungal infection. If results are negative and the biopsy is not diagnostic, it is assumed that these are aphthous ulcerations and treat patients accordingly.Most cases of esophagitis are diagnosed by clinical symptoms and confirmed with a barium swallow study. In such cases, treatment is begun empirically for candida esophagitis, especially in the presence of oral candidiasis. Fluconazole is the drug of choice and is given at a dose of 6 mg/kg/d in once daily dose. If a patient does not respond to empiric treatment after 3 days, then endoscopy with biopsy and culture of the esophageal mucosa should be done. If the biopsy results are compatible with fungal infection, parenteral amphotericin B is the drug of choice because some Candida albicans and Torulopsis glabrata and Candida krusei are resistant to fluconazole. Esophagitis secondary to HSV is treated with IV acyclovir, 750 mg/m2 /d divided into three doses. If CMV is the cause, then IV ganciclovir is used. Patients with recurrent esophagitis are at risk for esophageal stenosis. Development of chronic bilateral enlargement of the parotid glands may occur in as many as 15% of children with HIV infection and usually does not require any treatment, but sometimes parotid pain and fever develop in these patients. In this instance, infection is suspected, frequently with Staphylococcus aureus, although mouth flora may also be present. This complication is easily managed with a course of oral antibiotics, using antistaphylococcal agents. On the rare occasion when suppuration is suspected, an otolaryngologist should be consulted to evaluate the need for surgical treatment. Lymphomas and other tumors should be included in the differential diagnosis, especially in children with increasing parotid size. Diarrhea is a common manifestation of HIV infection.[13] Although an infectious cause is frequently suspected, other important causes include side effects of medications, malignancies, and HIV enteropathy. Antibacterial agents are indicated in the treatment of diarrhea associated with enteric pathogens, such as shigelle, salmonelle, and campylobacter. Adult patients commonly improve with fluoroquinolones, but in children, other alternatives (e.g., ampicillin, third-generation cephalosporins, or TMP-SMX) are used. HIV-infected patients, especially those with low CD4+ cell counts and frequent exposure to antibiotics, are at risk for diarrhea caused by Clostridium difficile. The treatment of choice is metronidazole with orally administered vancomycin used as an alternative drug. Relapse should not be considered a treatment failure because as many as 20% of patients relapse, and these patients should be retreated with metronidazole. Many viruses, including rotavirus, calicivirus, adenovirus, coronavirus, and astrovirus, can cause diarrhea. Specific treatment is available only for colitis associated with CMV (ganciclovir) or HSV (acyclovir). When pathogens cannot be identified, a consultation with a pediatric gastroenterologist is indicated for possible endoscopy and biopsy. Children who are immunosuppressed and have high viral loads benefit from HAART. Pulmonary complications Lymphoid interstitial pneumonitis is a chronic lymphocytic infiltrative disease of the lung.[14] The diagnosis of LIP in children is usually based on a typical chest radiograph with persistent reticulondular bilateral infiltrates. In more severe cases, significant clubbing occurs. In asymptomatic children with LIP and normal oxygen saturation, a chest radiograph should be obtained at least once a year, and the oxygen saturation should be monitored using pulse oximetry at each clinic visit. If a patient is hypoxic, steroids are indicated. Prednisone is given at a dose of 2 mg/kg/d for 2 to 4 weeks, with subsequent tapering to 1 mg/kg/d, and therapy is continued until the oxygen saturation becomes normal. Most children respond to this treatment within the first few weeks. In general, when an adequate response has occurred, the steroids may be weaned and discontinued. In some cases, repeated courses of steroids may be warranted. A few children with severe, advanced lung disease may not respond to steroid therapy, and if no response occurs after 4 to 6 months, the steroids should be discontinued. In addition, bronchodilators and chest physical therapy are helpful adjunctive therapies. The use of low doses of diuretics may also improve the respiratory status.When dealing with suspected bacterial pneumonia, an aggressive approach should be taken in patients with chronic lung disease. When possible, the treatment should be directed to the specific pathogen causing the infection. Treatment is usually empiric because noninvasive diagnostic procedures, such as blood and sputum cultures, yield an organism in approximately 30% of cases. Therapy is directed at the usual pathogens (i.e., Streptococcus pneumonie, H. influenze, and Staphylococcus aureus), but in patients with chronic lung disease, gram-negative organisms, especially P. eruginosa, must be considered potential pathogens. If a patient does not improve or his or her condition deteriorates on treatment, a bronchoalveolar lavage is indicated for diagnosis. The length of therapy is dependent on the cause and severity of the illness. Although 10 to 14 days of systemic antibiotic therapy is usually recommend, some children benefit from a longer course of treatment. In patients with chronic lung disease, pulmonary function tests may be beneficial at the onset of treatment and can be used as an indicator for length of therapy. If the pulmonary function tests continue to improve after 14 days of antibiotic therapy, treatment is continued until a return to baseline or a new plateau is reached. Children with HIV infection who have bronchiectasis or frequent episodes of bacterial pneumonia may benefit from daily prophylaxis with TMP-SMX. If this is not successful in decreasing the frequency of infection, monthly infusions of IVIG at 400 mg/kg/d may be beneficial. HIV nephropathy HIV-associated nephropathy in children presents as a spectrum of disease that ranges from mild to moderate proteinuria that is persistent, hematuria, renal tubular acidosis, and end-stage renal disease (ESRD). Because a timed urine collection is difficult to perform in children, the ratio of urine creatinine and urine protein is used to calculate the degree of proteinuria. A normal creatine-protein ratio is less than 0.2. A ratio more than 0.2 is abnormal and is consistent with nephrotic range proteinuria. If this finding persists, it can lead to hypoalbuminemia and edema but without elevation of serum triglycerides as occurs in patients with idiopathic nephrotic syndrome. Renal function deteriorates more slowly in children than in adults. Renal sonography shows increased echogenicity and provides details of the function of the kidneys. Biopsy of the kidney usually shows focal segmental glomerulosclerosis or diffuse mesangial hyperplasia and, less frequently, minimal change or systemic lupus erythematous-like nephropathy.Renal tubular acidosis is corrected with alkalinizing agents. Sodium or potassium citrate can be used depending on other electrolyte abnormalities. One milli-equivalent of citrate is equivalent to one milli-equivalent of bicarbonate. Start with 2 to 3 mEq/kg/d divided in 2 or 3 doses and adjust the dose to maintain a normal serum Ph. Patients with renal tubular acidosis may also need supplements of other minerals, such as calcium, magnesium, and phosphorus. Therapy for patients with proteinuria is divided in two categories: (1) treatment of incipient renal disease to slow the progression to ESRD and (2) the treatment of ESRD. Because the progression of disease in children is not as rapid as in adults, the first approach is to observe these patients over a period of time, monitoring electrolytes, blood urea nitrogen (BUN), and creatinine. The use of nephrotoxic agents should be avoided. Since the pathogenesis of the disease has been linked to immune complex deposition, an initial approach has been to use immunosuppressive agents. Steroids represent another option. The use of steroids in children has not been as beneficial as in adults. As with every other manifestation of HIV infection, HAART may have a significant role in the prevention or treatment of nephropathy. When ESRD has developed, a decision regarding dialysis must be made. The availability of HAART and the improved prognosis and extended survival time mandates an aggressive approach. Cardiomyopathy The spectrum of cardiac disease ranges from clinically silent lesions to fatal disease, and the severity of disease correlates with the degree of immune suppression. Cardiomyopathy seems to affect survival in HIV-infected children.[15] Depressed left ventricular function is common and progressive in children. Cardiac lesions described in patients with HIV include pericardial effusions; pericarditis; myocarditis; dilated cardiomyopathy; endocarditis; and vascular lesions, such as aneurysms, atherosclerosis, and pulmonary hypertension. Infiltrative neoplasm (i.e., Kaposi′s sarcoma and lymphoma) has also been reported. The cause of cardiomyopathy is mutifactorial. HIV cardiomyopathy starts early in life. The most common clinical manifestation of cardiomyopathy is sinus tachycardia. Other associated manifestations include bradycardia, dysrhythmias, abnormal blood pressure (i.e., hypotension or hypertension), left ventricular hypertrophy, pulmonary hypertension, pericardial effusion, and congestive heart failure (CHF).Evaluation of cardiac status includes a thorough history and physical examination followed by specific diagnostic tests when clinically indicated. Initial testing should include chest radiography and ECG. Noncardiac predictors of hemodynamic abnormalities are AIDS, wasting, LIP, recurrent bacterial infections, encephalopathy, anemia, positive CMV and Epstein-Barr virus serology, and age of less than 1 year. Treatment of HIV cardiomyopathy starts with early detection. Specific therapy of infectious causes of HIV-associated heart disease, such as CMV, Mycobacterium avium complex disease, tuberculosis, toxoplasmosis, and salmonellosis, have significant effect on outcome. Problems such as anemia, nutritional deficiency, hypoxemia, and electrolyte deficiencies need correction. Nonpharmaceutical therapeutic measures include limitation of physical activity, restriction of salt and fluid intake, and oxygen support. Pharmacologic treatment should be done in steps. The mildest manifestations of CHF are treated with angiotensin-converting enzyme inhibitors. The two most commonly used agents are enalapril and captopril. Renal function, serum electrolytes, and blood pressure must be monitored closely when using this class of drug. The next step is diuretics. Loop diuretics (e.g. furosemide) are preferred because thiazides are less potent and their efficiency decreases with decreased glomerular filtration rate. Patients who remain symptomatic despite these measures may benefit from the use of digoxin. Antihypertensive and antdysrhythmic agents are prescribed when appropriate in conjunction with a pediatric cardiologist. IVIG has been reported to be effective in patients with Kawasaki syndrome, CHF refractory to anticongestive therapy, and acute myocarditis. Because pericardial effusion is usually an incidental ECG finding, treatment depends on its severity and cause. When tamponade is present, pericardiocentesis is necessary. Pericardiocentesis is also indicated when bacterial infection is suspected. Nonsteroidal anti-inflammatory agents are useful in the management of patients with pain. Another issue is the management of patients with hypercholesterolemia and hypertriglyceridemia secondary to the use of protease inhibitors. The recommendation for the treatment of these side effects is modification of the diet and pharmacologic treatment with a lipid-lowering agent, if necessary. HIV encephalopathy Progressive and static encephalopathy with cognitive, behavioral, and motor manifestations has been described in HIV-infected children.[16] Although most children with neurologic impairment have no identifiable pathogen other than HIV, encephalopathy may occur as a result of opportunistic infections, inflammatory disease, vascular disease, or neoplastic changes. The workup of children with HIV and encephalopathy is as follows.
Pediatric intensive care issues Children with pulmonary PCP infections present with hypoxemia out of proportion to the interstitial lung disease seen on the chest x ray. They can rapidly progress to a clinical picture consistent with acute respiratory distress syndrome (ARDS) requiring 100 percent oxygen,mechanical ventilation requiring high positive end expiratory pressures (PEEP). Diagnosis is made by bronchoalveolar lavage (BAL)and transbronchial biopsy is no longer considered mandatory. Silver methanamine staining is positive for PCP on BAL specimen. These patients have concurrent hepatosplenomegaly, ascietis with hepatic dysfunction,elevated liver enzymes and deranged clotting. Jaundice is uncommon. Management is essentially supportive and identical to standard therapy for ARDS. Antiretroviral therapy and intravenous trimethoprim remains the treatment of choice as discussed previously. In addition treatment for fungal infections,atypical mycobacterial infection is carried out as guided by the cultures. With aggressive supportive management ARDS secondary to PCP pneumonia has a better prognosis and up to 60 percent survival has been reported. Occasionally neutropenic patients present with sepsis and multiorgan system failure. These patients have greater than 70 percent mortality. Anti retroviral drug therapy Following are the CDC 2003 guidelines for therapy of HIV infected children. [Table - 4] & [Table - 5] show indications of antiretroviral therapy and recommended regimen. [Table - 6] lists the indications for changing the therapy based on response to initial therapy. Currently available antiretroviral agents Two classes of drugs target the reverse transcriptase enzyme-the nucleoside reverse transcriptase inhibitors (NRTIs)and the non-nucleoside reverse transcriptase inhibitors (NNRTIs) while a third class, the protease inhibitors, target the viral protease. Although some drugs have been approved for the pediatric age group, identifying the optimal dosing regimen may still be an ongoing process. The recommended dosing schedules listed in [Table - 7] are specific to pediatric populations. For infants less than 2 years of age and especially for newborns, specialized dosing schedules may be necessary and are still in the process of evaluation for many of the newer antiretroviral agents. In addition, transition from childhood to adolescence to adulthood regarding recommended dosing may not be smooth or uniform, and caution must be exercised when approaching these transition periods. General features of antiretroviral agents Nucleoside reverse transcriptase inhibitors References
Copyright 2003 - Indian Journal of Critical Care Medicine Free full text also available from: http://www.ijccm.org/article.asp?issn=0972-5229;year=2003;volume=7;issue=4;spage=257;epage=272;aulast=Khilnani The following images related to this document are available:Photo images[cm03005t7.jpg] [cm03005t5.jpg] [cm03005t4.jpg] [cm03005t3.jpg] [cm03005t6.jpg] [cm03005t2.jpg] [cm03005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}