 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
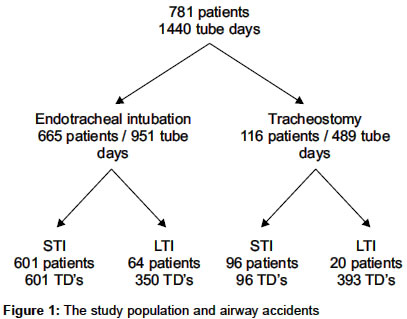
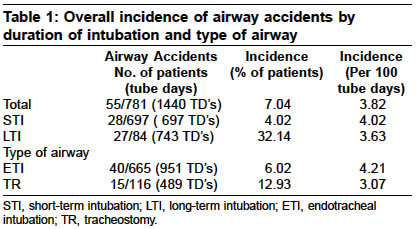
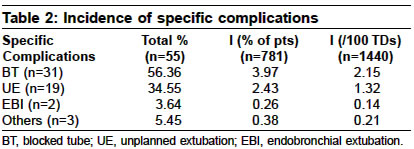
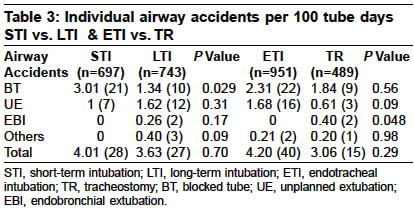
Indian Journal of Critical Care Medicine, Vol. 8, No. 1, January-March, 2004, pp. 36-39 Original Article Airway accidents in an intensive care unit Chatterjee Aparna, Islam Saeeda, Divatia JV Department of Anaesthesia, Critical Care and Pain Management, Tata Memorial Hospital, Mumbai Code Number: cm04006 ABSTRACT AIM: To document the incidence of airway accidents in the Intensive Care Unit, and to identify the difference in accident rates between short term and long term intubated patients, and between endotracheal intubation and tracheostomy. Key Words: Airway accidents, Critical Care, blocked tube, unplanned extubations, endobronchial intubation Control of the airway with the help of a tracheal tube is an important aspect of intensive care. The use of tracheal tubes however is not without complications. The longer a tube stays in-situ, the greater the chances of kinking, blockade and unplanned extubations. All of the above can lead to hypoventilation and hypoxia which are potentially life threatening. The few studies on unplanned extubations have reported an incidence ranging from 0.3 - 30%.[1],[2] Significant proportions of those who have an unplanned extubation tolerate it well and do not require reintubation.[6],[8] Most of these are associated with minimal or no morbidity.[4] One study of 53 patients however recorded three deaths at the time of unplanned extubations.[2] Tata Memorial Hospital is a tertiary level referral center for the comprehensive management of cancer in Mumbai and has a 22-bed ICU. A majority of the ICU admissions are from Surgical oncology, with selective referral from the medical and radiation oncology services. A large number of patients undergoing major head and neck surgery remain intubated in the ICU for airway protection for periods less than 24 hours. We undertook a study to document the incidence of airway accidents in our ICU, and to identify differences, if any, in airway accident rates between short term and long term-intubated patients and also between those who have an endotracheal tube compared to those with a tracheostomy. DESIGN Prospective observational, non-interventional study carried out in the 22-bed intensive care unit (ICU) over a 7.5-months period. MATERIALS AND METHODS Between June 2001 and January 2002, all adult patients admitted to the ICU with either an endotracheal tube or tracheostomy were included in the study. They were divided into those that required intubation for > 4 hours but < /= 24 hours {short-term intubation (STI)} and those who required a tube for > 24 hours {Long-term intubation, (LTI)}. Tube days (TD) were calculated from the day of intubation till the day of extubation or discharge from, or death in the ICU. The airway accidents occurring during this period were noted. The airway accidents taken into consideration were; blocked tube (BT), unplanned extubation (UE) including both self and accidental extubations, endobronchial intubation (EBI), kinked tube and leaking cuff. Tubes were considered blocked if resistance was felt on passing a suction catheter down the tube or if the lumen was found narrowed at extubation. All ventilated patients (LTI) were sedated with infusions of midazolam or propofol and morphine or fentanyl. Sedation was intermittently stopped every morning to assess neurological status. Patients undergoing STI (but not ventilated) for airway protection after major head and neck surgery received bolus doses of narcotics and anxiolytics (buprenorphine and midazolam) with or without a background infusion. Restraints are seldom used. Endotracheal tubes were fixed with adhesive tape applied to the lower chin and cheek for orotracheal tubes and to the nose and forehead for nasotracheal tubes. Polyvinyl chloride tubes with high volume-low pressure cuffs were used. PVC, reinforced latex or metal tubes were used for tracheostomies. They were secured either with a tape tied around the neck or sutured in place. Heat and moisture exchange filters (HMEF′s) or heated humidifiers were used for humidification[12] in LTI and intermittent saline nebulisation was used in STI. The duration for which the tube was in situ, date and time of the airway accident, description of the type of accident, severity of the accident and it′s impact on the course of the patient′s illness, whether preventable and if needed to be reintubated were noted. The severity of the airway accident was graded as follows: Mild: Little or no physiological consequence/ managed by resident on call. RESULTS 781 patients (1440 tube days) required either an endotracheal tube or a tracheostomy over the 7.5-months period. Details of patients are shown in [Figure - 1]. During this period there were a total of 55 airway accidents with an incidence of 3.8/100 tube days and 7.04% of patients. The incidence of airway accidents by duration of intubation and the type of airway is as detailed in [Table - 1]. The incidence of specific complications is detailed in [Table - 2] and [Table - 3] compares the incidence of complications in patients with STI vs. LTI, and endotracheal intubation (ETI) vs,. Tracheostomy (TR). On comparing the incidence of overall airway accidents per 100 tube days between STI and LTI, we found no significant difference except in the incidence of blocked tubes, which were found to be higher in the case of STI (P Value = 0.029). In STI all blocked tubes were removed while, in LTI the tubes were changed. There was no difference in the incidence of airway accidents (per 100 TD′s) between those with endotracheal intubation (ETI) as opposed to those with a tracheostomy (TR), except in the case of endobronchial intubations (EBI), the incidence of which was surprisingly found to be higher in the tracheostomy group (P Value = 0.048). Endotracheal tubes or tracheostomies that slipped out or were displaced during either change of patients position, sponging or due to patient′s agitation were included under the title of unplanned extubations. The incidence of unplanned extubations was 2.43% overall, and 1.32/100 tube days. Of the 55 cases of airway accidents, 48 were minor, 6 were moderate and 1 was a major accident, wherein the patient self-extubated and suffered a cardiac arrest due to hypoxia. DISCUSSION The overall incidence of airway accidents was found to be 3.82/100 tube days. No difference was noted between short-term group (STI) vs long-term intubation group (LTI) or the endotracheal tube group (ETI) vs tracheostomy group (TR). The incidence of blocked tubes was found to be significantly higher in the group that required short-term intubation (STI). The STI group comprised of patients who had undergone head and neck surgery and were kept under observation in the ICU. These patients were allowed to breathe spontaneously with a nasotracheal tube in situ, received oxygen via a T-piece arrangement and intermittent saline nebulisations to humidify the inspired gases. Most of the tubes were blocked either by blood or thick secretions that made it difficult to pass a suction catheter down these tubes. At extubation some endotracheal tubes were noted to have a significant narrowing of the lumen due to encrustations. We attribute this to inadequate humidification[12] and have started using continuous saline nebulisations in STI. In LTI, heated humidifiers or heat and moisture exchange filters (HMEF) were used. HMEF′s were changed every 24-48 hours. HMEF′s are known to provide efficient humidification with no tracheal tube occlusion for upto 48 hours and in some studies for upto 7 days without changing the filter.[13],[14] The rate of unplanned extubations in our study was found to be 1.32/100 tube days (1.32%). This value is significantly higher in comparison with Kapadia et al[3] (0.14%) and lower as compared to Epstein et al[4] (1.6%) and Carrion et al[5] (1.5-2.4%). This study was performed to document the incidence of various airway accidents. We did not systematically record data on causes and factors that may have lead to an increased incidence of airway accidents, such as the actual nurse: patient ratio at the time of the accident, time of accident, effect of weaning, and other such factors. The nurse-patient ratio in our ICU ranges from 1:2 to 1:4 and depends on the time of the day. We attribute this higher incidence of unplanned extubations to a combination of lack of 1:1 nursing staff in our ICU, inadequate sedation of our intubated patients, and lack of adequate communication and reassurance of our intubated patients as they wake up from sedation. Unplanned extubation can be a serious complication associated with mortality and is a quality of care concern.[9] All the patients who had an unplanned extubation were reintubated. Although few studies have advocated close observation following unplanned extubations as many may not require reintubation.[6],[7] With the use of better tube fixations, changing sedation protocols,[10] better communication with patients as they wake up from sedation, regular humidification of inspired gases and more vigilance by the medical and nursing staff,[11] we hope to reduce this incidence of airway accidents. We have implemented the above-mentioned strategies in our ICU in the form of a new airway protocol. An audit to assess this new airway protocol is underway at the moment. REFERENCES
Copyright 2004 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm04006f1.jpg] [cm04006t3.jpg] [cm04006t1.jpg] [cm04006t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}