 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
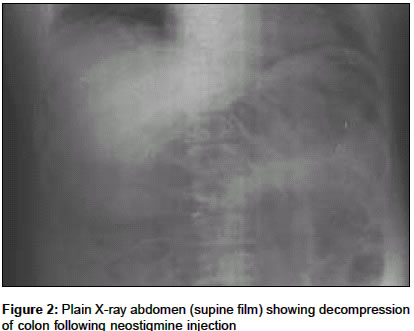
Indian Journal of Critical Care Medicine, Vol. 8, No. 1, January-March, 2004, pp. 43-45 Case Report Acute colonic pseudo-obstruction (Ogilvie's syndrome) in critical care unit Mehta Rajiv, Suvarna Deepak, Sadasivan S, Rajesh G, John Anil Department of Gastroenterology, Amrita Institute of Medical Sciences, Amrita Lane, Elamakkara P. O., Cochin - 682 026 Code Number: cm04008 ABSTRACT Acute Colonic pseudo-obstruction (Ogilvie's syndrome) is common occurrence in both the ICU and long-term acute care units. If not treated in time, it may lead to Colonic perforation or ischemia. Recent report showed that intravenous neostigmine, an acetylcholienastrase inhibitor, produces rapid colonic decompression in patients with acute colonic pseudo-obstruction (ACPO). We report four cases of acute colonic pseudo-obstruction in critical care unit and the response of neostigmine therapy.CASE 1 A 48 year-old male who was known case of systemic arterial hypertension on medication presented with features of right-sided hemiplegia with supra-nuclear facial palsy with global aphasia admitted in stroke unit. CT brain showed features of left middle cerebral territory infarct. Patient was receiving nasogastric feeding, physical therapy, anti-hypertensive and anti-platelet medication. After 3 days in the stroke unit, patient developed sudden distension of abdomen with constipation. Abdominal examination showed gaseous distension with sluggish bowel sounds. Rectal examination showed ballooning of rectum without fecal impaction. No evidence of infection, electrolytes abnormality or narcotic uses. Plain abdominal radiograph showed massive colonic dilatation involving entire colon without air fluid level with cecal diameter 10 cm [Figure - 1]. Thus, a diagnosis of acute colonic pseudo-obstruction was made. Patient was kept nil orally; passage of flatus tube; frequent side-to-side change of posture made. Patient had progressively increasing abdominal girth and plain radiograph after 12 hours showed increased cecal diameter more than 12 cm. He was given injection Neostigmine 2.0 mg intravenously slowly in stroke unit with monitoring of vital signs. Post injection, patient had rapid improvement clinically and plain radiograph taken after 30 minutes of neostigmine therapy showed marked reduction in colonic dilatation [Figure - 2]. Subsequently, patient had no gastrointestinal problem till discharge. CASE 2 A 67-year hypertensive lady on cardio selective beta-blocker, presented with features of acute confusional status. She had no history of head trauma or convulsion. MRI brain showed bilateral thalamic hemorrhage. In ICU she developed abdominal distension with constipation. Abdominal examination showed distended abdomen with absent bowel sound. Routine biochemical tests showed mild hypokalemia. She had no recent history of ingestion of narcotics or any drugs, which reduced intestinal motility, recently. Plain radiograph abdomen showed dilatation of all colonic segments including the rectosigmoid area with cecal diameter of 11 cm. She was managed conservatively including correction of hypokalemia. She did not show any response to conservative management for first 24 hours. She also received 2.0 mg intravenous neostigmine in the same manner as mentioned above. She responded clinically as well as radiologically following neostigmine therapy. But there was recurrence of abdominal distension with dilatation of colonic segments on plain radiograph after 24 hours of initial success. She received second dose of neostigmine in a same manner. She had responded with second dose of neostigmine and had no abdominal symptoms till discharge. CASE 3 A 69-year male case of hypertension, diabetes mellitus and dyslipidemia, presented with generalized tonic clonic seizure with inability to move right side of the body. CT brain plain showed left temporoparietal hematoma with intaventricular extension. He developed features of acute colonic pseudo-obstruction after 2 days. Clinical and radiological picture were same as mentioned in previous two cases. He had no electrolyte abnormality. He responded with 2.0 mg intravenous neostigmine. There was no recurrence of ACPO and had no abdominal symptoms till discharge. CASE 4 A 77-year hypertensive male on amlodepine presented with features of acute confusional state without head trauma or convulsion and was admitted to critical care unit. At the time of admission he had sinus bradycardia of 50 beats/min. with normal blood pressure. CT Scan brain, metabolic parameters and lumber puncture were normal. He was put on broad-spectrum antibiotics with supportive measures. On third day of admission, he developed progressive abdominal distension with absent bowel sounds. Plain radiographs showed features consistent with ACPO. In view of his sinus bradycardia, successful colonoscopic decompression was done, after 24 hours of conservative management. He had no abdominal symptoms till discharge. DISCUSSION Acute colonic pseudo-obstruction (Ogilvie′s syndrome) is characterized by gross dilatation of the colon or part of the colon.[1] Autonomic nervous system dysfunction with inhibition of parasympathetic fibers arising from spinal sacral segments seems to be the causative mechanism for colonic atony.[2],[3] Plain radiographs reveal massive colonic dilation with presence of air in the rectosigmoid area. The absolute diameter of the dilated caecum is not as important as the rate and duration of dilatation.[4] The diagnosis should be made only after adequately excluding mechanical obstruction. Spontaneous resolution in ACPO with conservative treatment was around 85%[1],[4] Recent studies[2],[5],[6] showed intravenous neostigmine (2 mg over 3-5 minutes) produce rapid colonic decompression in most patients. Refractory or recurrence pseudo-obstruction may require colonoscopic decompression with 90% success rate.[1] Surgery is reserved for those who fail medical or endoscopic management and develop signs of peritonitis or perforation. Our first three patients responded to neostigmine. Fourth had contraindication to neostigmine and underwent successful colonoscopic decompression. Two had response with first dose of neostigmine and third required second dose. Patient who did not respond to neostigmine had hypokalemia, which was corrected before neostigmine therapy, so electrolytes imbalance might have influence on out come following neostigmine therapy. None of our patients developed bradycardia after neostigmine therapy. Since all patients were under close monitoring during and after neostigmine therapy, glycopyrrolate was not given. REFERENCES
Copyright 2004 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm04008f1.jpg] [cm04008f2.jpg] |
| |||||||||

{kind=link}
{kind=link}