 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Critical Care Medicine, Vol. 8, No. 2, April-June, 2004, pp. 116-119 Review Article Hypothermia in trauma victims - Friend or foe? Søreide Eldar, Smith CharlesE Trauma and Intensive Care, Rogaland Central Hospital, Stavanger Reproduced with permission from Trauma Care, the official journal of International Trauma Care (ITACCS) Code Number: cm04012 LEARNING OBJECTIVES
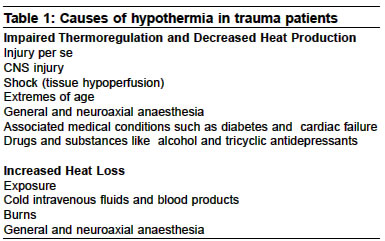
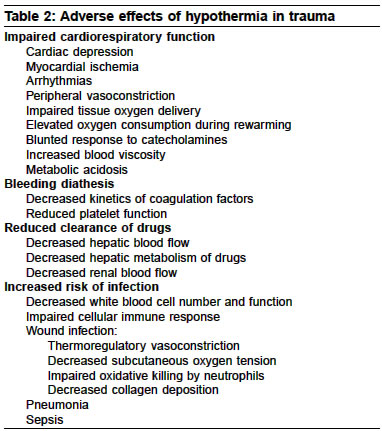
Incidence and causes of hypothermia in trauma patients Hypothermia is a well-recognised and life threatening consequence of injury.[1] In their prehospital study of 302 injured patients, Helm et al[2] found that almost every second patient were hypothermic. There was no connection between season of the year and frequency of hypothermia. Entrapped patients, however, were at higher risk (98% versus 35%; P < 0.001), as were patients older than 65 years (P < 0.001). Clinical symptoms of hypothermia like shivering were only noted in 4%. In 94 tracheally intubated patients brought to one regional trauma centre, Luna et al.[3] found that almost 2/3 of the patients had a core temperature of less than 36° C. Trauma in itself as well as bleeding with tissue hypoperfusion alters thermoregulation and result in hypothermia.[4] Some of the preventable factors that contribute to the high incidence of hypothermia in the trauma population are prolonged exposure in the field and administration of cold intravenous fluids [Table - 1].[1],[2],[3],[4],[5] Patients requiring emergency surgical intervention may suffer additional hypothermic insults from cold surgical preparation solutions and heat loss to the cold operating room environment. Administration of anaesthetic agents impairs the ability to maintain thermal homeostasis and causes internal redistribution of body heat from the warmer core to the cooler peripheral tissue, thereby further reducing core temperature in the exposed patient.[6] Pathophysiological consequences of hypothermia Hypothermia is associated with increased mortality and morbidity,[1],[2],[3],[4] with a dramatic decrease in survival at core temperatures below 34°C. In trauma patient, the traditional severity classification of accidental hypothermia has been revised with 34-36°C classified as mild, 32-34°C as moderate and < 32°C as severe hypothermia.[4] The increased morbidity and mortality is likely due to impaired coagulation, metabolic acidosis from poorly perfused tissues, hemodynamic instability, respiratory problems, and infections. The potential adverse effects of hypothermia in the injured patient are shown in [Table - 2].[1],[2],[3],[4],[5],[6] Decreases in core temperature during the course of initial evaluation and resuscitation are common, and can contribute to poor outcomes in the injured patient. Hypothermia, along with acidosis and coagulopathy, has been identified as a component of the "lethal triad" in injured patients. Intense shivering may occur between 34°C and 36°C with resultant increase in oxygen demand and metabolic rate.[1],[2],[3],[4],[5],[6] During re-warming, there may be release of sequestered cold blood and acid metabolites from peripheral vascular beds, dilation of the systemic vasculature, with resultant cardiac instability. Hemodynamic instability due to "re-warming shock" is characterised by hypotension, myocardial depression, and release of metabolic acids.[7] Hypothermia exerts a negative inotropic effect on the myocardium, and depression of left ventricular contractility occurs with moderate hypothermia.[8] Hypothermia is also associated with atrial and ventricular arrhythmias. The initial ECG change seen with hypothermia is sinus tachycardia. As the core temperature decreases, progressive bradycardia ensues. The cardiac response to catecholamines may also be blunted in hypothermic hearts, and cold cardiac tissue poorly tolerates hypervolemia and hypovolemia.[9],[10] Intraoperative hypothermia increases the incidence of morbid cardiac events such as myocardial ischemia, unstable angina, and ventricular tachycardia.[11] Increased cardiovascular morbidity may, in part, be due to a greater degree of peripheral vasoconstriction, increased norepinephrine levels, and altered alpha-adrenoceptor tone in response to cold. Hypothermia may promote surgical wound infection because of thermoregulatory vasoconstriction, decreased subcutaneous oxygen tension, impaired oxidative killing by neutrophils, and decreased collagen deposition.[6],[12] Blood glucose concentrations increase with hypothermia, which may require intensive insulin therapy to reduce mortality.[13] Hypothermia may lead to a bleeding diathesis as a result of impaired platelet function, inhibition of clotting enzyme kinetics, and activation of the fibrinolytic cascade.[1],[4],[14] Life-threatening coagulopathy in patients with severe injury who required massive transfusion is linked to temperatures below 34°C and a progressive metabolic acidosis.[14] Prevention and treatment of hypothermia in trauma patients Non-intended hypothermia in trauma victims still is a common problem, and occurs early during the resuscitative phase.[1],[2],[3],[4],[5] We are probably still paying too little attention to this. Even basic interventions easily prevent hypothermia.[15] Re-warming methods for the hypothermic trauma patient include both passive re-warming, active external re-warming, and active internal rewarming.[3],[4],[5],[6] Treatment of hypothermia in the trauma patient should begin with prevention of further heat loss. Fluid resuscitation can result in substantial core temperature decreases, mandating the use of efficient fluid-warming devices and pre-warmed fluids. Of the various non-invasive treatment modalities, convective warming is effective in restoring heat to the core,[6] although radiant heat may be easier to apply to the multiply injured trauma patient. Active core re-warming techniques such as CAVR increase core temperature by 1.5°C to 2.5°C/hr, and can be life saving in the hypothermic trauma patient with adequate perfusing rhythm.[16] The role of therapeutic hypothermia in trauma patients Hypothermia may prevent the initiation of the cascade of events after injury that leads to cell death. Further, hypothermia may be protective by decreasing oxygen consumption. Still, the effect of prolonged hypothermia during resuscitation after haemorrhagic shock is as yet unclear.[17] Both in blunt and penetrating injury current accepted practice therefore is to stop bleeding and fluid resuscitate, while simultaneously keeping the patient as close to normothermic as possible. Studies have found mild hypothermia to be protective in anoxic brain injury following resuscitation from prehospital cardiac arrest.[18],[19] The Advanced Life Support Task Force of the International Liaison Committee of Resuscitation (ILCOR) now recommends that unconscious adults with spontaneous circulation after out of hospital cardiac arrest should be cooled to 32-34°C for 12-24 hrs when the initial rhythm was ventricular fibrillation.[20] Studies have also focused on the therapeutic use of mild hypothermia in traumatic head injury and spinal cord ischemia.[21],[22],[23],[24],[25],[26],[27],[28] The role of therapeutic hypothermia (TH) in traumatic brain injury is still debated. Possible reasons for the conflicting results include methodological issues such as excluding patients with hypoxia or hypotension after resuscitation, timing of the hypothermic intervention, and duration of therapeutic hypothermia.[21],[22],[23],[24],[25],[26],[27],[28] It is also possible that longer periods of hypothermia (> 48 hours) is needed, especially in patients with intracranial hypertension.[26],[27],[28] In his excellent review of the potential for TH in different kinds of cerebral injury, Polderman[27],[28] concluded that the successful application of TH in traumatic brain injury depends on strict protocols and close monitoring to avoid complications like hypovolemia, hypotension and hyperglycaemia. Further, he emphasised that hemodynamically stable brain injured patients already mildly hypothermic at admission should not be immediately re-warmed. Finally, after prolonged periods of cooling, re-warming must be slow and controlled.[27],[28] SUMMARY Hypothermia often complicates the management of patients with severe blunt or penetrating injury, and has been associated with increased morbidity and mortality. Early control of bleeding and prevention of further heat loss are key factors to avoid the lethal triad of hypothermia, acidosis and coagulopathy. Hence, hypothermia is still considered a foe in these patients. On the other side, accidental or induced hypothermia may be beneficial ("a friend") in selected patients with traumatic brain injury. Some centres have already brought the latter concept into clinical practice, but more data is needed. REFERENCES
Copyright 2004 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm04012t1.jpg] [cm04012t2.jpg] |
| |||||||||

{kind=link}
{kind=link}