 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Critical Care Medicine, Vol. 8, No. 2, April-June, 2004, pp. 98-105 Review Article Airway management in trauma Rao BK, Singh VinodK, Ray Sumit, Mehra Manju Department of Critical Care Medicine, Sir Ganga Ram
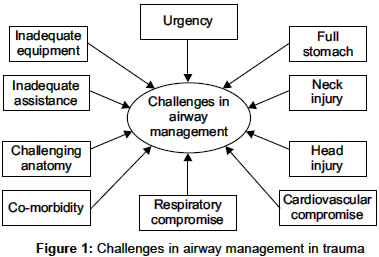
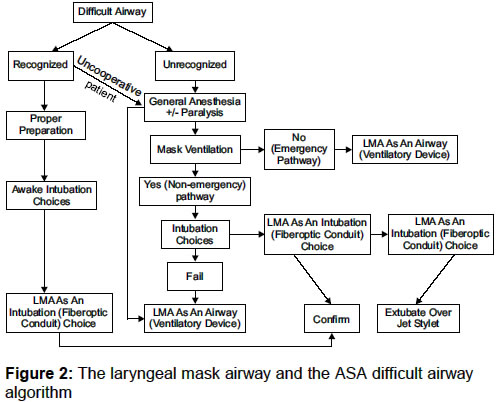
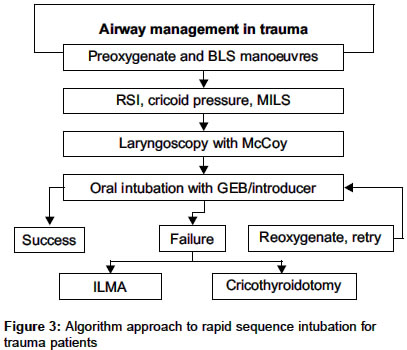
Hospital, *Department of Anaesthesia, L.N. Hospital, New Delhi Code Number: cm04019 ABSTRACT Airway Management for the victims of major trauma is the first priority in the care of the trauma victim and is a core skill in emergency medicine and critical care. Endotracheal intubation remains the gold standard for trauma airway management. Airway management in trauma patients is not just the capability to insert an oral/nasal airway or endotracheal tube beyond the vocal cords. The five components integral to modern, sophisticated airway management in trauma patients include equipment, pharmacologic adjuncts, manual techniques, physical circumstances, and patient profile. A trauma patient may require airway management in a variety of physical circumstances. Whereas, the commonly used airway management algorithms may not suffice in all these situations, the construction of a truly complete decision tree is also virtually impossible. There is consensus that it is not the intervention per se but rather the conditions, skills, and performance that might be the possible variables that affect outcome. Paramedics have only limited experience and on-the-job skills for invasive airway management. Difficult airway management is best left for the experienced physicians to handle.Key Words: Airway, Trauma, Endotracheal Intubation. The treatment of the seriously injured patient requires rapid assessment of the injuries and institution of life-preserving therapy. Inadequate delivery of oxygenated blood to the brain and other vital structures is the quickest killer of the injured. Ensuring an unobstructed airway and adequate oxygenation are first priorities in the resuscitation of the trauma patient. Unlike the elective surgical patient the trauma patients present many challenges [Figure - 1]. A diverse array of equipment and skills are necessary for optimal airway management.[1] These include: a. Application of supplemental oxygen (100% oxygen by partial or non-rebreather mask). 2. Advanced (nonsurgical): a. Bag-valve devices with masks 3. Surgical airway: a. Cricothyroidotomy (open or Percutaneous with dilators) Basic airway management While maintaining the airway and oxygenation of trauma patient care must be taken to avoid movement of the cervical spine, which runs the risk of producing a spinal cord injury.[2] When a patient requires manual manoeuvre to open the airway, the most appropriate methods must be determined. Of the three generally accepted manoeuvres, only two are acceptable to trauma patients[3] (head tilt manoeuvre should be avoided). The "Chin Lift" manoeuvre is performed by grasping the anterior base of mandible and gently lifting upward to move the chin forward. At the same time the lower lip is displaced downward to open the mouth. An assistant should firmly grasp the patient's head during this manoeuvre to prevent any displacement of cervical spine from its neutral position. An alternative method to open the airway is the "Jaw Thrust" (using both hands to push the angle of mandible forward bilaterally). Studies have shown that both these techniques cause less movement of the cervical spine than head tilt and have been demonstrated to be superior method for opening of obstructed airway.[3] It is standard practice to maintain head and neck immobilization with the use of a semi-rigid collar, lateral head support and taping or by manual in-line stabilization (MILS) if these devices are removed. Oral airways mechanically displace the tongue forward, clearing the posterior pharynx and restore airway patency. However, improperly placed oral airway actually worsens airway obstruction by folding the tongue back on itself. Once the airway has been cleared, oxygen should be administered via facemask or if necessary with bag-valve-mask ventilation. If positive pressure ventilation is required, cricoid pressure should be maintained, both to prevent aspiration and to prevent a significant amount of air insufflation to stomach. In spontaneously breathing patients basic airway manoeuvre can establish airway patency and restore adequate respirations. Intubation is reserved for those patients who continue to show signs of inadequate respiration after basic interventions or patients in whom these interventions alone are not likely to sustain adequate respiration. This may be present in patients with severe head injury, severe maxillofacial fractures, risk of aspiration of blood or vomitus, neck haematoma, laryngeal injury, tracheal injury, stridor, hypoxia, hypercarbia, tachypnea, cyanosis.[1] Prehospital advanced airway management Prehospital airway management can be fraught with complications related to hemodynamic alterations and difficulty with oxygenation and ventilation. Esophageal intubation, pneumothorax, and pulmonary aspiration, as well as other major complications, are reported to occur relatively frequently during emergency tracheal intubation outside of the operating room (OR).[4],[5] The ideal solution for airway of trauma patient would be a simple technique that provides effective ventilation and which does not had adverse haemodynamic effects on hypovolemic or head injury patients and there should be no or minimal risk of gastric insufflation and pulmonary aspiration. Considerable controversy persists regarding the optimal means and indications for airway management, the utility of paralytic agents to facilitate intubation, and the indications for advanced airway access techniques in the prehospital setting. Endotracheal intubation is an accepted standard in prehospital pediatric care. This standard exists with marginal support in published literature.[6] An intubation failure rate of 11.6% has been reported.[7] Prehospital intubation has been reported to improve survival in severe head injury patients.[8],[9],[10] Prehospital intubation did not improve survival in many studies.[11],[12],[13] A recent study has raised greater concern with suggestions that paramedics RSI protocols used in the USA to facilitate endotracheal intubations of head-injury patient was associated with an increased mortality and decrease in good outcomes versus matched historical control.[14] Large prospective randomized studies in the prehospital setting addressing the effects of hypoxia, abnormal ventilation, and inadequate airway and possible benefits of invasive airway management have not been conducted in either adult or pediatric populations and the whole issue lacks consensus. It is not the intervention per se (i.e., endotracheal intubation) but rather the conditions, skills, and performance that might be the possible variables that affect outcome.[15] For paramedic-based systems, bag-valve-mask ventilation or noninvasive airway devices like the laryngeal mask airway or the new laryngeal tube may be advantageous.[16],[17],[18] Personnel who are well experienced in the everyday clinical routines of assessing and managing difficult airway scenarios are the only individuals who should perform endotracheal intubation in the hostile prehospital environment. As difficulty arises with securing the airway and the number of laryngoscopic attempts increases, the occurrence of hypoxemia, esophageal intubation, regurgitation, airway trauma, and cardiac arrest are more common.[19],[20] The ASA Task Force on the Management of the Difficult Airway has made a recommendation, based on the consultant's consensus opinion, that an alternative method should be pursued to secure the airway when difficulty with intubation is encountered.[21],[22] [Figure - 2]. Methods of securing definitive airway in trauma patient Tracheal intubation is often referred to as the gold standard for maintaining a definitive airway but can be difficult in the trauma patient for a variety of reasons. Adequate pre-oxygenation is not always possible, particularly in patients with facial fractures or those who are agitated and combative. Cervical spine immobilization provides a less than ideal position for laryngoscopy and the presence of vomitus tissue debris and local edema all make visualization of the larynx more difficult. If the patient requires intubation, this is usually performed orally using direct visualization of glottis while maintaining in-line stabilization of cervical spine. The recommended approach to airway management is to initially treat all trauma patients as if they have an unstable cervical spine even if the initial plain cervical spine x-rays are normal. End-tidal carbon dioxide (PetCO2) is used as an aid for confirming endotracheal intubation in both the ED and the out-of-hospital setting.[23] Rapid sequence intubation (RSI) Patient combativeness, lack of practice, and the concomitant need for in-line cervical stabilization are common hazards for successful invasive airway management.[24],[25],[26] RSI is the most commonly used first line technique for ED airway management in trauma. Laryngoscopy and intubation are very powerful stimuli and are frequently associated with hypertension, tachycardia, laryngospasm and bronchospasm, especially in individuals who are inadequately paralysed or not deeply unconscious. This cardiovascular response may be life threatening to those with critical cardiac disease or raised intracranial pressure. Rapid-sequence intubation (RSI) is the technique for emergency airway control designed to maximize successful endotracheal intubation while minimizing the adverse physiologic effects of this procedure. [Figure - 3] Abbreviations: MILS = manual in-line stabilisation, GEB = gum elastic bougie/introducer, ILMA = Intubating Laryngeal Mask Airway [Courtesy: Dr. Michael JA Parr. Difficult airway management in trauma. Trauma Criticare 2003: Page 59. 7th Conference of International Trauma Anaesthesia and Critical Care Society (Indian Chapter), New Delhi, India.] Even in patients with a Glasgow Coma Scale score of 3, there is airway reactivity (gag and cough reflexes) with a considerable potential to promote intubation failure.[27] RSI with a sedative induction agent (e.g., thiopental, ketamine, or etomidate) followed by administration of a rapidly acting neuromuscular blocking agent (e.g., succinylcholine) to induce unconsciousness and motor paralysis is associated with a decrease in intubation failures and complications[28],[29] and is the gold standard for emergency intubation attempts.[30] RSI requires familiarity with patient evaluation, airway-management techniques, sedation agents, neuromuscular blocking agents, additional adjunctive agents, and postintubation management techniques. While the medications for airway management generally are administered intravenously, it should be kept in mind that in paediatric patients intraosseous access is an acceptable alternative for the administration of several different agents, including those used for endotracheal intubation.[31] The use of succinylcholine may result in fewer difficult intubations in the trauma patient than when a nondepolarizing neuromuscular blocking agent is used.[32] Rocuronium used with propofol creates intubation conditions equivalent to those with succinylcholine.[33] but a "can not intubate, can not ventilate" situation may become disastrous due to prolonged blockade produced by rocuronium.[34] The unanticipated difficult airway is arguably the most severe complication of RSI, and all individuals performing the technique must prepare in advance a specific plan for this scenario. The intubating laryngeal-mask airway (ILMA) may be an ideal device for airway control if other techniques fail. The ILMA causes less hemodynamic change and less injury to the teeth and lips than direct laryngoscopy.[35],[36] Surgical airway Surgical airways are required when basic interventions and intubation are not likely to succeed (e.g., severe upper airway anatomic distortion from mid or lower facial trauma) or have failed, and is best performed early (before hypoxemia, hypercarbia, apnea occurs). Cricothyroidotomy and translaryngeal jet ventilation are safe and more readily applicable. Tracheostomy is generally reserved for non-emergent situation with the exception of patients with laryngeal fracture. While there is ample literature concerning these techniques in adults, their use in children has been limited. Most importantly, considerable practice may be required to become and stay facile with many of these "alternative techniques" of airway management.[31] In situations of difficult endotracheal intubation, rapid sequence protocols frequently include the use of paralytic agents and cricothyrotomy for airway management. There has been some concern about the use of prehospital cricothyrotomy because of higher complication rates compared to the emergency department.[37] With better intubation skills, the incidence is now decreasing.[38] Given the increasing rarity of this procedure, it is likely that many EM, surgical, and anesthesiology residents will not acquire clinical experience with this technique during training.[39] Which will deprive them of a very useful and effective tool of difficult airway management. The cervical spine trauma is assumed to be relative contraindications for percutaneous tracheostomy. In a recent report the safety of modified Grigg's technique was reported in trauma patients after failure to accomplish orotracheal intubation.[40] Percutaneous tracheostomy can also be safely performed in trauma patients without cervical spine clearance and neck extension, including patients with stabilized cervical spine or spinal cord injury in the critical care setting.[41] Airway management in special situation Cervical spine fracture (CSF) Airway management in the blunt trauma patient is complicated by the potential for causing or exacerbating an injury to the cervical cord if an unstable cervical fracture is present. In a cadaver model of a destabilized third cervical vertebrae, Brimacombe J et al showed that significant displacement of the injured segment occurs during airway management with the face mask, laryngoscope-guided oral intubation, the esophageal tracheal Combitube (Kendall-Sheridan, Neustadt, Germany), the intubating and standard laryngeal mask airway; but not with fiberscope-guided nasal intubation.[42] The choice of airway control in the trauma patient with CSF differs between anesthesiologists and surgeons, the trauma surgeons being more familiar with surgical airway. The technique utilized is dependent upon the judgment and experience of the intubator. However, the method selected does not have an adverse affect on neurological status as long as in-line stabilization is maintained. The recommendations of the American College of Surgeons Committee on Trauma for airway control with suspected cervical spine injury details the methods, which are safe, effective, and acceptable.[1],[43] The technique of choice for emergency intubation of a patient with a potential cervical spine injury is direct laryngoscopy and oral intubation with manual in-line stabilization, following a period of pre-oxygenation, intravenous induction of anaesthesia, paralysis with suxamethonium and application of cricoid pressure.[44],[45] Placing the patient's head and neck in neutral alignment will tend to make the view at laryngoscopy worse,[46] but intubation will be aided greatly by the use of a gum-elastic bougie.[47] If intubation of the patient proves impossible, a laryngeal mask[48] may provide temporary oxygenation and ventilation while a surgical cricothyroidotomy is performed. Because difficulty with intubation can be expected in this situation additional airway adjuncts and equipment should be immediately at hand. The likelihood of successful and smooth intubation is likely to be increased by use of the McCoy laryngoscope, a gum elastic bougie/bougie and skilled assistance. In case of difficulty or failure the only two airway adjunct devices of choice are the Intubating Laryngeal Mask Airway and the Combitube. The Intubating Laryngeal Mask Airway are useful because of their ease of insertion, and ability to allow effective ventilation. They are likely to cause less gastric insufflation than ventilation with a Bag Mask and to some extent may protect the airway from aspiration/contamination from above which. It also allows blind or fibre-optic guided intubation and is likely to represent the 'back-up' device of choice.[49],[50] With adequate precautions and care commonly used methods of airway management rarely lead to neurologic deterioration.[51] It is impossible to intubate a patient if he or she has a correctly fitting cervical collar-the collar then must be removed and manual inline stabilization used before attempts at intubation. Patients with cervical spine injuries treated with halo fixation present unique challenges in terms of airway control. Emergent intubation in the setting of halo fixation in trauma patients is difficult and often deadly. Heightened vigilance regarding the airway and early tracheostomy may be considered in high risk patients.[52] Laryngotracheal injury and tracheobronchial disruption Diagnosis of injuries to the larynx depends on inquiring to mechanism of injury and examining the anterior neck for subcutaneous emphysema, swelling, contusion and localized tenderness. CT can reveal tracheal injury and can be used to select trauma patients with pneumomediastinum for bronchoscopy, leading to early confirmation and treatment.[53],[54],[55] Diagnosis of tracheal rupture may be delayed as a result of its rare incidence, subtle and nonspecific clinical and radiologic manifestations, and the much more overt clinical signs of other more common associated injuries. If suspected, the airway should be examined in awake, spontaneously breathing patient with a bronchoscope, and an endotracheal tube can be advanced over bronchoscope to secure airway.[56],[57],[58] Severe airway compromise will require intubation, emergency tracheostomy, intubation of a tracheal injury[58] or a tracheostomy should be created below the laryngeal injury.[59] Although intubation over a flexible fiberoptic bronchoscope is desirable in cases of suspected tracheobronchial injury, it may not be feasible. Blind nasal or direct orotracheal intubation is usually not indicated in laryngeal trauma, as the endotracheal tube may not traverse the lesion, can create a false passage leading to fatal airway obstruction.[60] Elective intubation should be attempted only with a surgical team present and prepared for emergency tracheostomy.[61] Maxillofacial trauma The oropharynx and nasopharynx are frequently compromised in severe maxillofacial trauma, posing an immediate threat to airway from resulting deformity or from aspiration of teeth, dentures bone and blood. Reduced level of consciousness form associated closed head injury or shock, may progressively result in airway obstruction.[62] Airway problems are particularly evident with the fractures of mandible. Bilateral fracture may result in a floating mandible. Such victims must sit upright, leaning forward so that suspended tongue and suprahyoid muscles should not fall out of the airway. In a seated, cooperative patient suction of the airway, and oral intubation may secure the airway. Intravenous low dose ketamine (20-70 mg), which is a potent analgesic that maintains muscle tone and aspiration, can be used to relieve pain. Maxillary fractures are less often associated with direct airway obstruction but may compromise the airway by causing severe bleeding from fracture sites or from lasceration of ethmoidal arteries. Lefort III fractures (separation of cranial and facial skeletons) are usually associated with basal skull fractures. Attempts at nasal intubation may force the endotracheal or nasogastric tube through the cribrifom plate into subarachanoidal space or into brain.[63] Airway obstruction involving Lefort III are usually managed by awake tracheostomy. Submandibular transmylohyoid intubation has been suggested as an alternative to tracheostomy.[64],[57] Conclusion All equipment, including oxygen, suction, tubes, stylets, laryngoscopes, and blades, cricothyroidotomy and jet insufflation trays must be ready before patient arrival. The vast majority of trauma patients will be managed by rapid sequence induction/intubation. Preoxygenation and only short attempts at laryngoscopy are part of the procedure. Therefore careful planning and preparation are essential. The most experienced person should perform any airway procedure. In difficult airway scenarios, as for midfacial fractures, endotracheal intubation should be performed only with immediately available tracheostomy. Cricoid pressure, awareness of drug kinetics and pharmacodynamics in hypovolemic patients, and reliable assessment of tube position are necessary; additional pharmacotherapy (ongoing sedation, continuous muscle relaxation with nondepolarizing neuromuscular blockade) will be required. The ability to find rapid and effective solution to airway may ultimately determine the patient's survival. References
Copyright 2004 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm04019f3.jpg] [cm04019f2.jpg] [cm04019f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}