 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
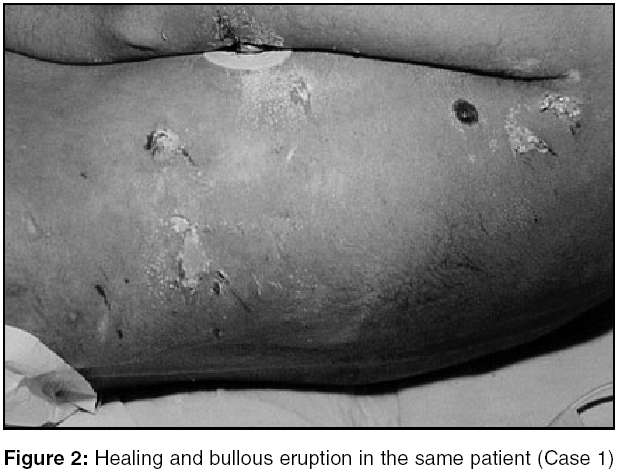
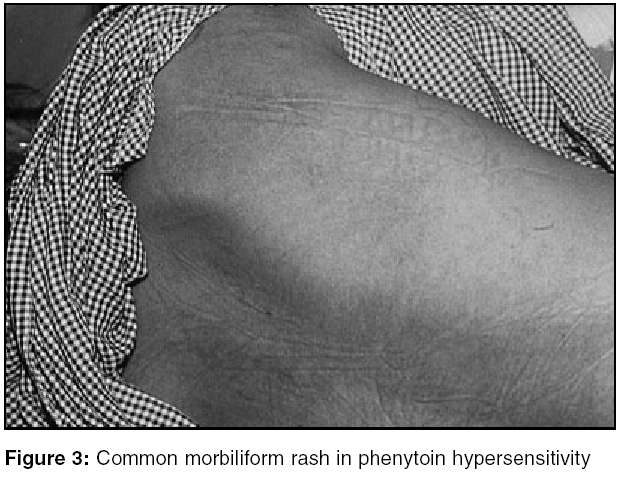
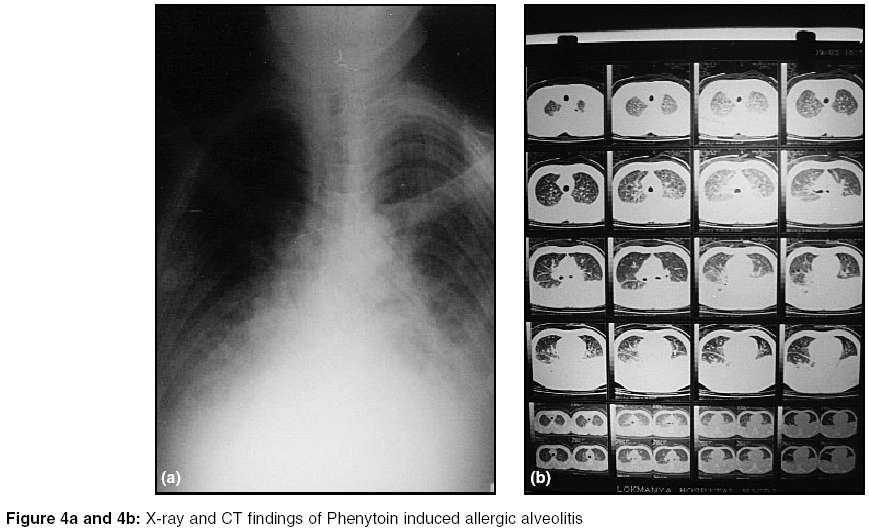
Indian Journal of Critical Care Medicine, Vol. 9, No. 1, January-March, 2005, pp. 22-27 Case Report Hypersensitivity and dose related side effects of phenytoin mimicking critical illness Pillai LalithaV, Ambike DhananjayP, Hussainy SM K, Vishwasrao Sunil, Pataskar Satish, Gaikwad MarutiM Critical Care Department, Lokmanya Hospital, Chinchwad, Pune Code Number: cm05004 Abstract OBJECTIVE: To describe phenytoin-induced rare hypersensitivity and dose related reactions, emphasizing the importance of early omission of drug to achieve clinical improvement.DESIGN: Case series and review of literature. SETTING: Tertiary level medical intensive care unit. PATIENTS: Three cases, two of whom had hypersensitivity reactions and the third had drug-induced dyskinesia. INTERVENTION: Omission of phenytoin and corticosteroid therapy in two cases. RESULTS: Improvement and discharge. CONCLUSION: A high index of suspicion of drug-induced complications is necessary especially when multiple drugs are being administered to critically ill patients. Keywords: Phenytoin, skin lesion, allergic alveolitis, dyskinesia, Phenytoin hypersensitivity syndrome (PHS) Introduction Phenytoin is a widely prescribed anticonvulsant in ICUs. However it is associated with myriad of side effects both idiosyncratic and dose-related. We present three cases each with a characteristic side effect of the drug mimicking critical illness.Case 1 35-year-old man with a history of moderate alcohol consumption was admitted with complaints of vomiting, progressive deterioration in sensorium since six hours and right upper limb focal convulsions since one hour. He was not on any medications and there was no history of trauma. On arrival in ER, patient was unconscious. He had Cheyne Stokes respiration, BP: 180/130 mm/Hg, Pulse: 140/min, temp. 37.8oC, SpO2 on room air was 70%. His pupils equal and bilaterally reacting to light. Neck was supple and other systemic examination was normal. He was intubated and mechanically ventilated. Investigations revealed Hb: 15.5 gm/dl, total leukocyte count (TLC): 12600/cmm, Liver function tests (LFT), Renal function tests (RFT) and coagulation profile were within normal limits. CT scan showed haematoma of 2.4 x 2 cm size in head of right caudate nucleus with mass effect. Initial treatment included Inj. phenytoin in loading dose of 13 mg/kg and maintenance dose of 100 mg 8 hourly, Inj. ceftriaxone, H2 blockers, mannitol, and I.V. fluids. Haematoma was surgically evacuated and he was postoperatively mechanically ventilated. Sensorium improved with spontaneous eye opening and movements of left-sided limbs, but he developed continuous fever from 5th post-operative day. Chest X-ray was normal and no other obvious clinical or laboratory evidence of infection was noted. CSF examination was normal. On 7th Post-operative day blood cultures were sent, which were sterile. Investigation revealed -TLC-23000/cmm with eosinophilia (10%), S. bilirubin: 1.8 mg/dl, AST 504 IU/L, ALT- 286 IU/L, Sr. Creatinine 1.9 mg/dl, and blood urea-80 mg/dl. Patient continued to have fever >39°C. Antibiotic was changed to Inj. Piperacillin and Tazobactam. Repeat CT scan showed resolving haematoma with mild obstructive hydrocephalus. Patient continued to deteriorate clinically. On 10th day CVP line was removed and tracheostomy was performed. In view of the deteriorating clinical picture, severe sepsis with multi organ failure (MOF) was considered and antibiotic was changed to meropenem and Linezolid. Two days later, few blisters over axillae and ears were noted [Figure - 1]. For the first time, a possibility of Phenytoin Hypersensitivity Syndrome (PHS) was considered. Phenytoin was discontinued. Steroids were given and in the next 24 hours patient became afebrile. Over next four days he could be gradually weaned from ventilator and tracheostomy was closed. He became conscious, oriented, was obeying verbal commands. On 5th day of omitting phenytoin, he was shifted out of ICU and discharged after a week. This patient had characteristic features of PHS, such as deranged LFTs, RFTs, vesiculo-bullous eruption [Figure - 2] and persistent fever. These clinical features, absence of a septic focus and the probable response to corticosteroid therapy was compatible with the diagnosis of PHS.Case 2 50-year-old alcohol dependent man was admitted to ICU with history of consumption of 50 tablets of phenytoin (100 mg each), 3-4 hours prior to admission. He was a known epileptic for last ten years, on tablet phenytoin- 100 mg thrice daily. Ten days prior to the admission; he was admitted in another hospital for anaemia with bleeding piles and was discharged after transfusing 3 units of blood. On admission here, he was conscious, haemodynamically stable with gross pallor, rash [Figure - 3] and active bleeding piles. Systemic examination was normal. Investigations showed Hb 5.0 gm/dl with haematocrit 19.5%, TLC: 6500/cmm, Serum electrolytes, RFT, LFT, coagulation profile, urine examination and CXR were normal. Peripheral blood smear showed hypochromic microcytic anemia. Serum phenytoin level was 26.3 mg/ml (therapeutic levels 10-20 mg/ml). Over the next 3 days he was given antibiotics (cefotaxime), H2 blockers, folic acid, B12, sodium valproate and three units of packed cells. Hb improved to 8.2 gm/dl. On 5th day patient appeared breathless, developed fever (38.4oC) with chills, SpO2 was 90%, respiratory rate was 30/min, pulse: 102/min. On auscultation there were bilateral basal crepts. ABG showed PaO2 of 70 mmHg on room air, TLC 6500/cmm with absolute eosinophilic count 500/cmm (normal range 40-440/cmm). Chest X-ray [Figure - 4] showed bilateral lower zone infiltrates with effusion. Echocardiography was normal. Possibility of fluid overload or early ARDS due to multiple transfusions was considered. In spite of diuretics, change of antibiotics and trial of non-invasive ventilator, no clinical or radiological improvement occurred over the next 48 hours. CT Thorax showed lymph nodes in paratracheal, subcarinal regions with bilateral infiltrates in both lower lobes and pleural effusions. Possibility of phenytoin induced allergic alveolitis was considered in view of lymphadenopathy, pleural effusions and bilateral infiltrates with eosinophlia. Steroids were started. Patient gradually improved over next three days and CXR showed marked improvement. Case 3 65-year-old hypertensive, diabetic patient on aspirin developed aspirin-induced gastritis leading to haematemesis and malena for four days. During this period he became drowsy with raised S.bilirubin (3.0 mg/dl), liver enzymes and serum ammonia. CT scan was normal and he was treated as early hepatic encephalopathy. He was given Inj. pantoprazole, lactulose, Vitamin K to which he responded well and LFT and Serum ammonia levels normalized. Sensorium improved. On 6th day he developed complex partial seizures, was given Inj. phenytoin with loading and maintenance dose along with B complex. Serum electrolytes, LFT, Serum ammonia level and EEG were normal. After 24 hrs he was shifted out of ICU. From 10th day onwards he appeared lethargic, non-communicative and developed slurred speech. Hyperammoniacal encephalopathy and electrolyte disturbance were ruled out. MRI brain with venogram also ruled out structural lesion. He developed progressive ataxia without nystagmus, needed support for standing, walking and had scissoring gait. Serum phenytoin level was done on the 5th day of starting phenytoin and found to be 30 mg/ml. Phenytoin was discontinued on the same day. As there was no further deterioration, patient was discharged . At the time of discharge patient needed help for all routine activities like feeding, walking and had severe dysarthria with incomprehensible speech. Over a period of one month he gradually improved and started taking food independently, needed no support for walking and was absolutely normal at the end of two months.Discussion Each of the above cases represented either; hypersensitivity reaction or a dose related side effects to phenytoin. Phenytoin hypersensitivity can present as rashes or Phenytoin hypersensitivity syndrome (PHS). Hypersensitivity rashes are usually like measles or rarely severe exfoliative, purpuric, bullous, lupus erythematosus, Steven Johnson′s lesions and toxic epidermal necrolysis lesions.[1],[2],[3] Unusually aggressive skin reactions have been reported in patients of brain tumors on phenytoin undergoing radiotherapy.[3] Singh G et al in their series of 117 patients started on phenytoin for seizures prophylaxis reported a higher incidence of cutaneous adverse reaction to phenytoin in patients with solitary cysticercus granuloma.[4] Increase incidence of cutaneous hypersensitivity has also been reported in association with viruses such as immunodeficiency, cytomegalo and simplex. Phenytoin should be omitted if rash appears, in mild cases it may be restarted, but if the rash reappears phenytoin medication is contraindicated forever. PHS is a rare syndrome, potentially fatal[1],[5],[6],[7] non-dose related idiosyncratic complication of phenytoin use. In most cases reaction occurs between two weeks to two months after administering the drugs.[2],[6],[7],[8] A broader terminology of Anticonvulsant hypersensitivity syndrome (AHS) has been used as this syndrome can result from usage of any aromatic anti epileptic drug (AED) such as phenytoin, carbamazapine (CBZ), phenobarbitol and occasionally lamotrigine[7],[8] the commonest being carbamazepine and phenytoin. The aromatic AEDs are metabolized to hydroxylate aromatic compounds, such as arene oxide. If detoxification of this toxic metabolite is insufficient, it may bind to cellular macromolecules causing cell necrosis or secondary immunological response.[8] The incidence of AHS is higher among first-degree relatives, may be autosomal dominant, familial and genetically mediated.[1],[7],[8] Cross-reaction among AEDs may be as high as 75%.[1],[8],[9] Our first case mimicked post-operative sepsis with multiorgan failure. The initial blisters on the ears were most inconspicuous and were attributed to friction rub or povidone iodine (paint applied during surgery). Concomitant drugs, which could have produced skin rashes, were cephalosporin antibiotic but this had been stopped on 5th day. Improvement occurred after stopping phenytoin and starting steroids. Clinical presentation of PHS varies but the hallmark features are fever, skin rash, lymphadenopathy, accompanied by multiorgan involvement usually involving the kidney, liver, CNS or lungs, associated with leucocytosis with atypical lymphocytes eosinophilia and edema of face.[1],[7],[9] A generalized maculo-papular eruption with follicles and pustules on face, ears and upper trunk is characteristic.[1] Hepatitis occurs in 75% of the cases with increase in serum aminotransferases, prolongs the stay and mortality increases up to 50%.[1],[2] Interstitial nephritis, renal failure, myopathy, rhabdomyolysis, coombs negative hemolytic anemia and interstitial pulmonary infiltrates have been reported.[1],[2] There is no specific treatment for PHS other than withdrawal of the drug, or substituting it with valproate, gabapentin, topiramate, tiagabine and levetiracetam, which carry a lower risk of cross-reactivity along with supportive care.[10] The second patient developed fever became progressively tachypnoeic five days after taking an overdose of phenytoin tablets. The CT thorax findings of bilateral basal infiltrates and lymph nodes warranted a consideration of allergic alveolitis. This is a rare condition presenting with fever, cough, dyspnoea and peripheral eosinophilia.[11],[12] Chest films shows marked interstitial shadows, occasionally lymphadenopathy and pleural effusion.[13] Generalized lymphadenopathy may also be present and can cause pseudolymphomatous syndrome.[12] Lung biopsies have shown alveolar wall and small vessel infiltration with inflammatory cells.[12] The condition is known to resolve when the drug is stopped. Similar syndrome has been known with CBZ. Phenytion was not the suspect drug initially as this patient was on phenytion for ten years. We feel that the patient had multiple prescriptions in the preceding days, which included H2 blockers, cephalosporins, NSAIDs and CBZ. These drugs have been reported to increase the incidence of hypersensitive cutaneous reaction with phenytoin,[14] and may have induced hypersensitivity to the previously tolerated phenytoin. Klassen[15] reports of previously tolerated phenytoin, subsequently showing hypersensitivity after it, was substituted by CBZ. This phenomenon is unlike cross sensitivity, which is seen amongst the aromatic AEDs in which patient develops hypersensitivity to a drug that was used to replace the drug, for which hypersensitivity had developed.[15] The temporal relation to phenytoin overdose, apparent absence of other causative agents that can induce allergic alveolitis, X-ray and CT findings of pulmonary infiltrates, lymphadenopathy, pleural effusion and recovery after starting steroids compels us to conclude that this was a case of secondary sensitization of phenytoin, causing allergic alveolitis. Phenytoin has a narrow margin between therapeutic and toxic levels and they can be marked variation in phenytoin levels amongst individuals and the associated clinical symptoms, with reports of levels of 50 mg/ml giving rise to no symptoms. The most common dose related side effects manifests as CNS toxicity which are nystagmus on lateral gaze, loss of smooth extraoccular movement and drowsiness at level of 20-30 mg/ml. At levels greater than 30 mg/ml, vertical nystagmus, diplopia, ataxia or lurching gait and alterations in the level of consciousness occurs. Phenytoin can rarely induce dyskinesia including chorea, dystonia tremors and asterixis. The 3rd case of elderly diabetic male developing crippling ataxia was a case of dose related adverse reaction. It was included in this series because it mimicked critical conditions like, thrombo-embolic strokes, hyperammoniacal and other metabolic encephalopathy including B12 deficiency states. Severity of his symptoms and early presentation can be due to his age, previous hepatic derangement and concomitant use of H2 blocker. Liver diseases have been known to cause unusually high levels of serum phenytoin.[14] This case is being presented here to create awareness of the drug interactions, specially in critically ill elderly patients with multiple prescriptions, which can affect the drug levels causing diagnostic and therapeutic confusion increasing, the morbidity, repeated imaging investigations and prolonging the hospital stay. None of our patients had history of drug allergy. All of them had acute presentation, short interval between drug dosing and clinical presentation. This may be because in two patients loading doses of phenytoin had been given and the third was a case of drug overdose. In two of the patients liver function was abnormal, two were alcohol dependent, one was an elderly, and all were on H2 blockers. In two of our cases cephalosporin were co prescribed along with H2 blockers. The other co-prescribed drugs, which have been reported to increase serum phenytoin levels, are diazepam, H2 blockers, phenothiazines and salicyclates.[14] The hypersensitivity and drug reaction increased the morbidity, the costs and prolonged the ICU stay. It also caused diagnostic dilemma. It mimicked sepsis, ARDS and multi-system organ failure. Our patients improved because of the early recognition, omitting phenytoin and starting steroids.[1],[5],[7],[9] Conclusion In spite of the fact that PHS has been known since 1940s,[11] because of infrequent and diverse clinical presentation, it still remains unrecognized and can mimic critical illness. Its timely recognition is important to avoid potentially fatal re-exposure. When diagnosis is in doubt - patch test, lymphocytes transformation test or macrophage migration inhibitor factor can be helpful. Patients with AHS should avoid all aromatic anticonvulsants and benzodiazepines, valproic acid or one of newer anticonvulsants should be used for seizure control. We also recommend frequent monitoring of serum phenytoin levels in elderly critically ill patients with multiple co- prescriptions, those with altered liver function and where loading doses have been used. The purpose of this review was to critically analyze the literature related to the toxicity and side effects of phenytoin. The review was restricted to publications identified by a search of Medline or manufactures database or both. References
Copyright 2005 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm05004f4.jpg] [cm05004f2.jpg] [cm05004f3.jpg] [cm05004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}