 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
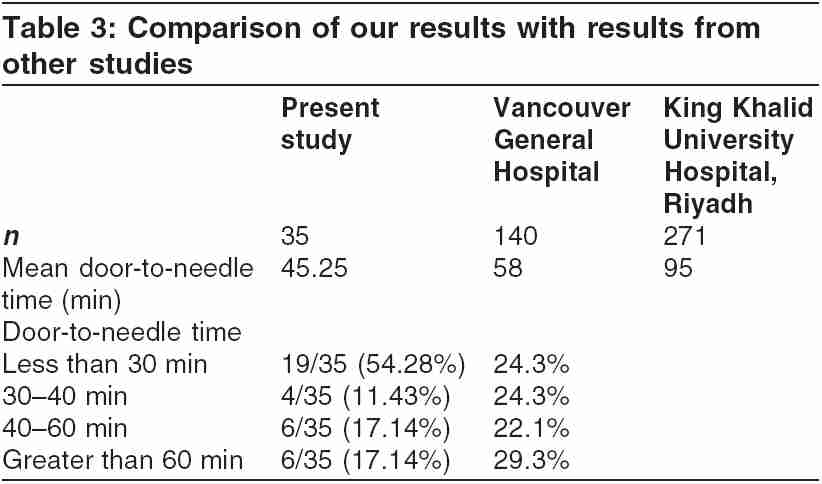
Indian Journal of Critical Care Medicine, Vol. 9, No. 3, July-September, 2005, pp. 137-140 Original Article Evaluation of the door-to-needle time for fibrinolytic administration for acute myocardial infarction Masurkar VA, Kapadia FN, Shirwadkar CG, Shukla U, Sood P Department of Critical Care Medicine, P.D. Hinduja National Hospital and Medical Research Centre, Mumbai Correspondence: Dr. Vikram Masurkar, 4-6/ 19, Talmakiwadi, Javji Dadaji Marg, Tardeo, Code Number: cm05021 Abstract Background: Fibrinolytic therapy has reduced mortality following acute myocardial infarction (AMI) with the major effect coming from early achievement of infarct-related artery patency.Aim: To evaluate the door-to-needle time for fibrinolytic administration for AMI and to identify factors associated with a prolonged door-to-needle time. Materials and Methods: Our study was a prospective audit of patients who were thrombolyzed for AMI at our hospital from July 1, 2004 to March 15, 2005. All patients admitted with AMI, who were candidates for fibrinolysis, were included. We recorded the door-to-needle time. Whenever possible, we tried to find out the reason for prolonged door-to-needle time. Results: A door-to-needle time of <30 min could be achieved in 19 of our 35 patients (54.28%). Mean door-to-needle time was 45.25 min. Discussion: Although most guidelines recommend a door-to-needle time of less than 30 min, most hospitals fail to achieve this in most patients. A study conducted by Zed et al. at the Vancouver General Hospital showed that a door-to-needle time of less than 30 min was achieved in only 24.3%. The door-to-needle time achieved at our center was shorter. In most of our patients who were thrombolyzed late, a delay in taking or interpreting an electrocardiogram was responsible. Transfer to the intensive care unit for thrombolysis also resulted in considerable delay. Conclusions: A door-to-needle time of less than 30 mins could be achieved in 19 of our 35 patients (54.28%). A significant number of AMI patients thrombolyzed did not meet the guideline for door-to-needle time of less than 30 min. Keywords: Acute myocardial infarction, Door-to-needle time, Fibrinolytic therapy Introduction Fibrinolytic therapy has reduced mortality following acute myocardial infarction (AMI), with the major effect coming from early achievement of infarct-related artery patency. The Grampian region early anistreplase trial showed that delaying thrombolytic treatment by 1 h increases the hazard ratio of death by 20%, equivalent to the loss of 43/1000 lives within the next 5 years (95% CI 7-88, P = 0.012). Delaying thrombolytic treatment by 30 min reduces the average expectation of life by approx 1 year.[1] Thus, a short time to treatment interval must be considered as an adjunctive agent to fibrinolytic therapy. There are four components which determine the time between the onset of MI and achievement of reperfusion. (1) delay in seeking medical attention, (2) transport delays, (3) the door-to-needle time (the interval between the patient's arrival at the medical facility and the initiation of fibrinolytic therapy), and (4) fibrinolytic reperfusion time-the time between the administration of fibrinolytic therapy and the achievement of reperfusion. Efforts to reduce each of these components will lead to additive benefits in improving time to reperfusion and survival of patients with acute MI. The door-to-needle time is the easiest to modify. Materials and Methods Our study was a prospective audit of patients who were thrombolyzed for AMI at our hospital from July 01, 2004 to March 15, 2005. We conducted a chart review of these patients. All patients admitted with AMI, who were candidates for fibrinolysis, were included. We recorded the following durations: 1. Time required to transfer the patient from the hospital entrance to the casualty. Whenever possible, we tried to find out the reason for prolonged door-to-needle time. Results A door to needle time of less than 30 min could be achieved in 19 of our 35 patients. [Table - 1] shows the time taken to complete each step, which constitutes the door-to-needle time. Of the patients in whom there was a delay, in five patients the initial ECG showed subtle ST-segment changes which did not merit thrombolysis. Subsequent ECGs showed ST elevation. Two patients were transferred to the intensive care unit (ICU) for thrombolysis. The decision was taken by the casualty medical officer. One of our patients came to the hospital with an ECG taken by a general practitioner. The ECG showed an acute ST-elevation myocardial infarction (STEMI). However, the casualty medical officer did not identify these changes. One patient had a cardiac arrest owing to ventricular fibrillation (VF), which caused a delay. In seven patients, we could not identify any reason for a delay. [Table - 2] shows the door-to-needle time that was achieved in our study. Discussion It has been proven that a shorter door-to-needle time results in better outcome. However, what is the standard of care? To address this question, Shuster and Dickinson[2] brought out recommendations for ensuring fibrinolytic therapy for AMI. They recommended early recognition of AMI symptoms by the public and health-care professionals, early access to emergency medical services, and early action by emergency-care providers in administering thrombolytic therapy (within 30 min after the patient's arrival at the emergency department). Grunfeld[3] responded to this article in the next issue of Can Med Assoc J . He mentioned that door-to-needle time of less than 30 min is probably an unrealistic goal. He also added that, to dogmatically adopt 30 min as the time interval during which all eligible patients are to receive thrombolytic therapy may well result in as many as half the patients receiving less than the recommended care. In 2004, the AHA and ACC jointly brought out guidelines for the management of patients with STEMI. It was recommended that the delay from patient contact with the health-care system (arrival at the ED or contact with paramedics) to initiation of fibrinolytic therapy should be less than 30 min (level of evidence: B).[4] The American College of Chest Physicians (ACCP) guidelines recommend that for patients with acute MI who are candidates for fibrinolytic therapy, the therapy should be administered within 30 min of arrival to the hospital or first contact with the health-care system (grade 1A).[5] Although most guidelines recommend a door-to-needle time of < 30 min, most hospitals fail to achieve this in most patients. A study conducted by Zed et al.[6] at the Vancouver General Hospital showed that a door-to-needle time of < 30 min was achieved in only 24.3%.[Table - 2] shows a comparison of our results with results from studies conducted at the Vancouver General Hospital and King Khalid University Hospital, Riyadh.[7] Zed et al . found that shorter door-to-needle times were achieved when patients were thrombolyzed without a cardiology consult.[6] However, all patients at our center were thrombolyzed after a cardiology consult. Zed also noted that patients who arrived at the hospital during the night shifts were thrombolyzed faster. We found no such difference in our study. In most of our patients who were thrombolyzed late, a delay in taking or interpreting an ECG was responsible. Transfer to ICU for thrombolysis also resulted in considerable delay. The above factors need to be looked into to improve door-to-needle time at our hospital. Conclusions We could achieve a door-to-needle time of less than 30 min in 19 of our 35 patients (54.28%). A significant number of AMI patients thrombolyzed at our hospital do not meet the guideline for door-to-needle time of less than 30 min [Table - 3]. Factors associated with this should be addressed to improve the care of patients with AMI. References
Copyright 2005 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm05021t3.jpg] [cm05021t2.jpg] [cm05021t1.jpg] |
| |||||||||

![[Table - 1]](/showimage?cm/photo/cm05021t1.jpg){kind=link}
![[Table - 2]](/showimage?cm/photo/cm05021t2.jpg){kind=link}
{kind=link}