 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
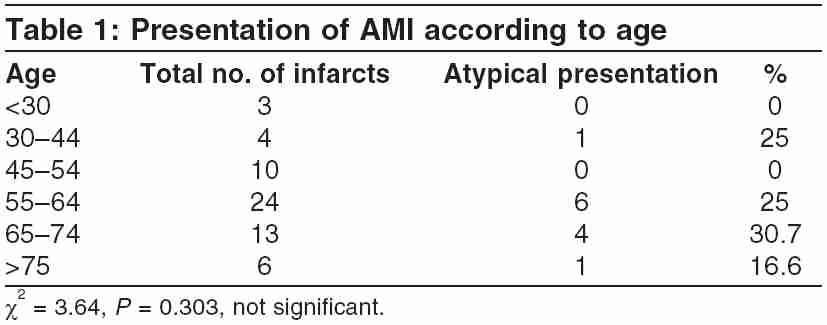
Indian Journal of Critical Care Medicine, Vol. 9, No. 3, July-September, 2005, pp. 151-154 Original Article Modes of presentation of acute myocardial infarction Chowta KN, Prijith PD, Chowta MN* Department of Medicine, Kasturba Medical College, Mangalore * Department of Pharmacology, Kasturba Medical College, Mangalore Correspondence: Dr. Nithyananda Chowta K, Department of Medicine, Kasturba Medical College Hospital, Attavar, Mangalore-575001. E-mail: knchowta@yahoo.com Code Number: cm05024 Abstract Aim: To study the various modes of presentation of acute myocardial infarction (AMI).Methods: A total number of 60 patients of AMI admitted in various teaching hospitals of Kasturba Medical College, Mangalore, were studied. The following factors were evaluated: onset of symptoms, mode of presentation, site of infarction, and hospital outcome. Results: Out of 60 patients, 12 (20%) presented with atypical symptoms. The maximum incidence AMI with atypical symptoms was in the age group of 65-74 yr (30.7 %), followed by the age group of 55-64 yr (25%). No patient presented with atypical symptoms below 30 yr. Patients experiencing MI without chest pain tended to be older (mean age 61 vs 58 yr) and were women (35% vs 12.5%); 80% of patients presented with chest pain followed by dyspnea (28.3%) and vomiting (13.3%). The in-hospital mortality of MI patients who presented with typical and atypical symptoms were 16.6% and 33.3%, respectively. In this study, anteroseptal infarction was most common (31.6%). Fifty percent of inferior-wall MI patients presented with atypical symptoms. Conclusion: In this study, there was no significant association between onset of MI and circadian pattern. Keywords: Atypical symptoms, Chest pain, Myocardial infarction Introduction Acute myocardial infarction (AMI) continues to be a major public health problem in the industrialized world, despite the impressive strides in the diagnosis and management over the past three decades. Although the death rate from AMI has declined by approx 30% over the last decade, its development is still a fatal event in approximately one-third of the patients.[1] It is well known that presentation of AMI may have many variants. The classic syndrome of chest pain described by Henrick is by no means pathognomonic and Henrick himself admitted that in some cases there might be no pain at all.[1],[2],[3]The population of the AMI patient presenting no chest pain has not been well characterized. Although it is widely known that patients with diabetes mellitus may not have chest pain during AMI possibly secondary to autonomic dysfunction, other clinical features associated in patients who do not experience chest pain remain largely undefined. Understanding the factors associated with atypical presentation may help in the earliest identification and treatment of these patients with MI. [1],[2],[3] Among the symptoms shown to be associated with unrecognized AMI are dyspnea, nonproductive cough, fatigue, abdominal or epigastric pain, nausea, vomiting, syncope, or palpitation.[4],[5],[6] Identifying the symptoms and signs of acute AMI is paramount for successful management and early treatment. Patients must realize that their symptoms may be consistent with cardiac disease and numerous reports have shown that patients may delay seeking care if they do not know that their symptoms may be consistent with MI. The problem is further compounded if patients believe that chest pain is a necessary hallmark feature of acute MI. [7],[8],[9] In the studies confined to the local population, work done on the modes of presentation of AMI was insufficient. The present study has been undertaken to evaluate various modes of presentation in patients with AMI and finds out whether there is a circadian pattern in the onset of AMI. Materials and Methods Patients with AMI admitted in various teaching hospitals of Kasturba Medical College, Mangalore, were studied. The diagnosis was confirmed by electrocardiogram (ECG) changes and/or enzyme abnormalities. A total of 60 cases were studied. The criteria of ECG changes are as follows. 1. Presence of pathological Q-wave. The following factors were considered: (1) onset of symptoms, (2) modes of presentation, (3) site of infarction, and (4) hospital outcome. Results Out of 60 patients 40 were males (66.66%) and 20 were females (33.33%). Mean age of the patients was 59.5 years. Out of 60 patients, 12 (20%) presented with atypical symptoms. The maximum incidence AMI atypical symptoms was in the age group of 65-74 years (30.7%) [Table - 1], followed by the age group of 55-64 years (25%). No patient presented with atypical symptoms below 30 years. Patients experienced myocardial infarction MI without chest pain tended to be older (mean age 61 vs 58 years) and were women (35% vs 12.5%) [Table - 2]. [Table - 3] shows the presenting symptoms of AMI. Eighty percent of patients presented with chest pain, followed by dyspnea (28.3%), sweating (21.7%), and vomiting (13.3%). Epigastric pain was the presenting symptom in 10% of patients. Three patients gave history of syncopal attack as the presenting symptom. Three patients complained palpitation. Only one patient with atypical symptom had previous history of angina (8.33%) compared with patients with typical symptoms with history of angina (20.83%). The in-hospital mortality of MI patients who presented with typical and atypical symptoms were 16.6% and 33.3%, respectively [Table - 4]. The anteroseptal infarction was most common (31.6%) and mortality was high in anterior-wall MI. Among the inferior-wall MI patients 50% presented with atypical symptoms [Table - 5]. Discussion Chest pain has been reported as the cardinal feature in patients with AMI. The WHO requires the presence of chest pain as one of the cornerstone feature for the diagnosis of chest pain.[1] In the present study, approx 20% of patients with AMI presented without chest pain on initial clinical evaluation. Patients experienced AMI without chest pain tended to be older (mean age 61 vs 58 years) and were women (35% vs 12.5%). In the Reykjavik study,[1] approx 30% of MI patients presented with atypical symptoms. Results from other population studies have shown that 20-60% of all MI are presented with atypical symptoms. According to Canto and Shlipak,[2] patients presented with atypical symptoms were older and were women. In the present study, there is a slight increase in the incidence of painless infarction with increasing age. In the group between 55 and 64 years, 25% patients presented with atypical symptoms and 31% in 65-74 years age group. This is comparable with Kennel[3] and others, where the values were 27% and 31%, respectively. In contrast to earlier studies in which patients who were 70 years or older were more likely to present without chest pain, in this study only one patient out of six presented with atypical symptoms. An increase in the proportion of atypical MI with advancing age was not statistically significant although it is not commonly seen before the age of 55. A much larger sample would be required to prove or disprove the possibility. We have documented a pronounced gender difference with females far outnumbering males in the incidence of painless infarction. In the present study only one patient with previous history of angina presented with atypical symptoms of AMI, showing a lower prevalence of angina among those with unrecognized MI group. This is in comparison with Framingham Study[8] and Honolulu Heart Program Study,[7] which also showed a low prevalence of angina pectoris among unrecognized MIs. In this study a higher percentage (50%) of inferior-wall MI patients presented with atypical symptoms, which is statistically significant. The Honolulu Hawai Heart Program Study[7] also demonstrated a pronounced increase in painless infarction with inferior-wall MI patients (51%). A higher proportion of inferior-wall MI tends to cause atypical symptoms, such as epigastric pain or abdominal distress, which would be failed to be recognized as MI. However, the study by Kennel[3] and others showed that there was no difference in the electrocardiographic location of the infarct between those with atypical and typical symptoms of MI. In the Framingham Study[8] also, the proportion of atypical MI did not appear to vary with electrographic location of the infarct. Patients with atypical MI group showed a higher in-hospital mortality than did the typical MI group (33% vs 16%), though statistically insignificant. When only the age at MI, the most important determinant of mortality, was adjusted, the atypical MI had approx 16% higher mortality from all causes. In the Framinham study[8] also, age adjusted long-term mortality for all cases were slightly worse among unrecognized MI case than among recognized MIs. This is in contrast with the Reykjavik study,[1] in which the prognosis for the patients with atypical MI is no better than that for patients with unrecognized MI. To conclude, only a comparative small number of patients had atypical presentation. Although there was a notable difference regarding age and sex, it was statistically insignificant because of the limited sample population. Patients with inferior-wall MI presented more often with atypical symptoms. Mortality was higher in atypical group, though statistically insignificant. References
Copyright 2005 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm05024t3.jpg] [cm05024t1.jpg] [cm05024t4.jpg] [cm05024t5.jpg] [cm05024t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
![[Table - 3]](/showimage?cm/photo/cm05024t3.jpg){kind=link}
![[Table - 4]](/showimage?cm/photo/cm05024t4.jpg){kind=link}
![[Table - 5]](/showimage?cm/photo/cm05024t5.jpg){kind=link}