 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
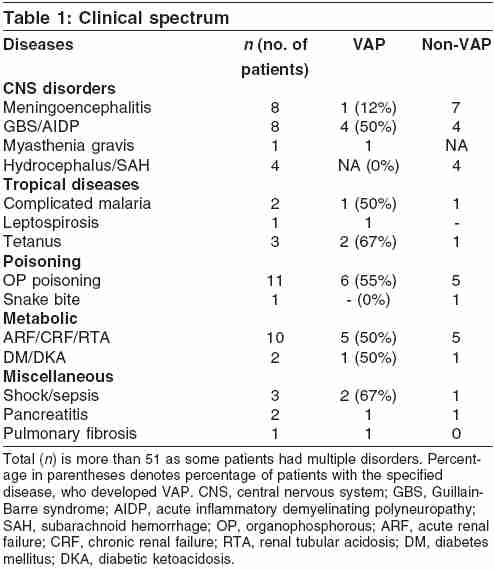
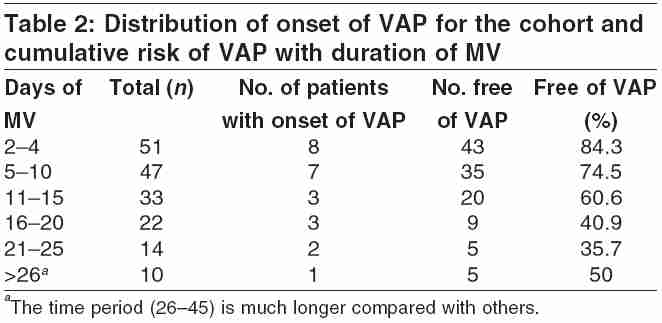
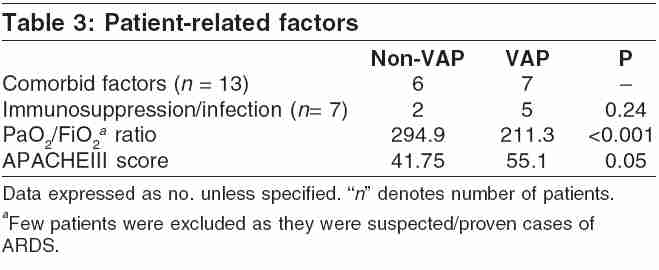
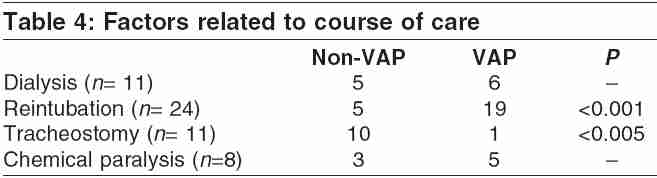
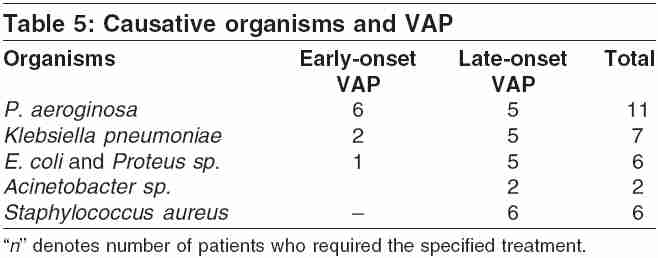
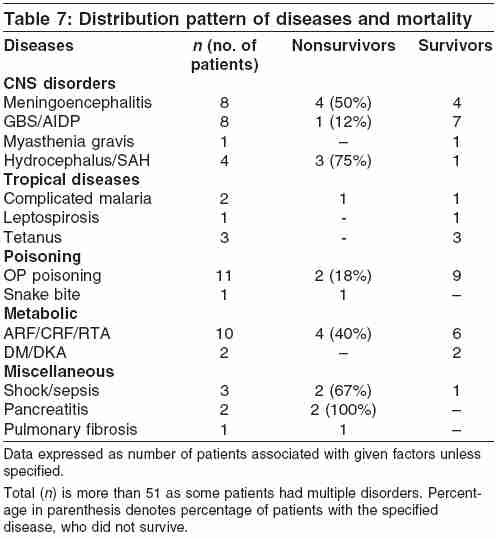
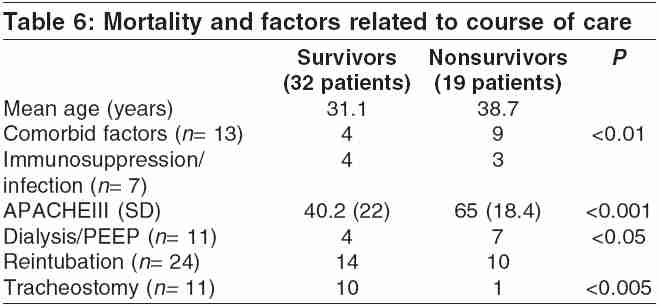
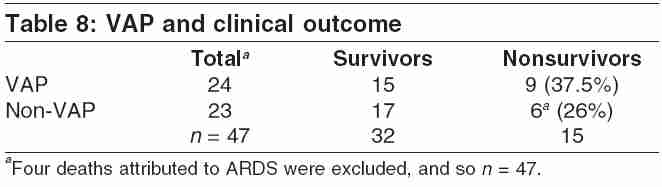
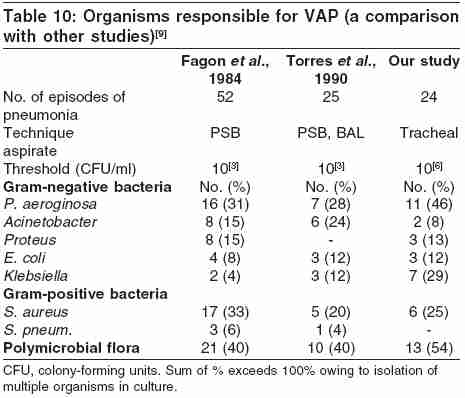
Indian Journal of Critical Care Medicine, Vol. 9, No. 4, October-December, 2005, pp. 211-216 Original Article Incidence, clinical outcome, and risk stratification of ventilator-associated pneumonia-a prospective cohort study Rakshit Panwar, Nagar VidyaS, Deshpande AlakaK Department of Medicine, Grant Medical College, Sir J. J. Group of Government Hospitals, Mumbai Code Number: cm05033 Abstract Context and Aim: Ventilator-associated pneumonia (VAP) remains to be the commonest cause of hospital morbidity and mortality in spite of advances in diagnostic techniques and management. This project aims to study the various risk factors and the common microbial flora associated with VAP. It also evaluates the use of APACHEIII scores for prognostication.Study Design: A prospective cohort study was conducted over 1 year in medical critical care unit (CCU) of a tertiary-care teaching hospital. Methods and Material: VAP was diagnosed using the clinical pulmonary infection score (CPIS) of more than 6. The study cohort comprised 51 patients. All CCU patients requiring mechanical ventilation for more than 48 h formed the study group. Statistical Analysis Used: Univariate analysis, χ 2-test, and paired "t-test." Results: Twenty-four out of fifty-one cases developed VAP. These cases had an average APACHEIII score of more than 55 on admission to critical care unit (CCU). They needed prolonged mechanical ventilation and had lower PaO2/FiO2 ratio as compared with the remaining patients who did not develop VAP. Pseudomonas aeroginosa was the commonest and most lethal organism. The mortality in the VAP group was 37% and correlated very well with higher APACHEIII scores on admission. Conclusions: Longer duration of mechanical ventilation and the need of reintubation are associated with proportionate rise in the incidence of VAP. Deteriorating PaO2/FiO2 ratio correlated well with the onset of VAP. Higher APACHEIII scores on admission stratify the mortality risk. Keywords: APACHE III (Acute Physiology, Age and Chronic Health Evaluation) Scores, Comorbid illnesses, Mechanical ventilation, Mortality, Nonsurvivors, PaO2/FiO2 ratio, Ventilator-associated pneumonia Introduction Ventilator-associated pneumonia (VAP) refers to bacterial pneumonias developing in patients who have been receiving mechanical ventilation (MV) for at least 48 h.[1] VAP is the commonest complication associated with MV reported at the rate of 1-3% per day of MV.[2] Prevalence ranges from 10% to 65% in tertiary-care hospitals with pari passu rise in case fatality rates of more than 20% according to reported studies.[3] Incriminating pathogens vary among hospitals.[4] Therefore, incidence of VAP and the associated local microbial flora needs to be studied in each setting so as to guide more effective and rational utilization of antimicrobial agents.[4] The precise diagnosis of pneumonia is often difficult in critically ill patients. Purulent sputum may follow intubation or leakage of oropharyngeal secretions around the artificial airway. Furthermore, chest roentgenographic changes consistent with pneumonia may be caused by pulmonary edema, pulmonary infarction, atelectasis, or acute respiratory distress syndrome.[5] Lack of an unequivocal gold standard complicates the issue of deciding the best diagnostic technique for suspected VAP. Although the sensitivity of a clinical diagnosis of VAP is high, the specificity is low. But VAP is one entity in which a subjective clinical impression appears to be more accurate than a set of objective criteria.[6] APACHEIII score, which is a further refinement of APACHE system, may help in stratifying hospital mortality risk, which may impact on the scope and intensity of treatment. This study was designed to determine the incidence of VAP, the associated risk factors, the causative microbial flora, and the role of APACHEIII in prognostication of patients at the time of admission to CCU in a tertiary-care centre. Materials and Methods The study spanned a period of 1 year. All cases admitted in CCU in past 1 year requiring MV for longer than 48 h formed the study cohort. Patients who were already on MV before admission to CCU or those who died within 48 h of starting MV were excluded. VAP was considered as a subjective clinical impression. It was further substantiated using clinical pulmonary infection score (CPIS). CPIS of greater than 6 was used as diagnostic criteria for VAP.[7] Pugin et al.[7] developed a CPIS score based on giving 0-2 points each for fever, leukocyte count, oxygenation, quantity, and purulence of tracheal secretions, type of radiographic abnormality, and results of sputum culture and Gram stain. The baseline evaluation of all the cases in this study included the patient-related factors such as age, concomitant diseases, immunosuppression, indication of MV, the ratio of PaO2 to FiO2 prior to onset of VAP, and severity of illness based on APACHEIII scoring system. On admission to CCU, the entire cohort was allotted scores for their age, chronic health status, physiologic parameters, acid-base status, and neurological status, based on APACHEIII scoring system. Total APACHEIII score was deduced by adding all these scores.[8] The risk factors included reintubation, use of chemical paralysis, need for dialysis, duration of MV, and duration of CCU stay. Statistical Analysis Results The study cohort comprised 51 patients with 29 (56.9%) males and 22 (43.1%) females. The mean age of patients in this cohort was 34 years; 24 out of 51 patients (47%) developed VAP during CCU stay. The incidence rate of VAP in our study was 26 per 1000 ventilator days. [Table - 1] shows the clinical spectrum of our cases that includes 21 patients with various neurological disorders, 6 cases of tropical diseases, 12 cases of poisonings, 12 cases of metabolic disorder, 3 cases of sepsis, and others. Some of our patients had multiple disorders. The incidence of VAP was greater either in patients with diseases necessitating prolonged MV (e.g., Guillain-Barre syndrome, tetanus, organophosphorus poisoning, etc.), or in patients with those diseases that predispose to pulmonary infection (such as sepsis, tropical diseases, or immunosuppression) [Table - 1]. It is also significant to note that the incidence of VAP was considerably low in patients with diseases which presumably, had unaffected lungs before admission to CCU, for example, meningoencephalitis (12%), hydrocephalus (0%), snake bite (0%), etc. [Table - 1]. [Table - 2] shows the distribution of onset of VAP for the study cohort. The total ( n ) number of patients on MV who were being followed during each time period is given along with the percentage of those people who did not develop VAP. Also given is the number of cases with onset of VAP during each time period. This table clearly demonstrates the decline in percentage of patients free of VAP as the duration of MV increases. Patients who developed VAP within 96 h of MV were categorized as having "early-onset VAP" and those who developed after 96 h were classified as "late-onset VAP." Eight patients developed early-onset VAP and 16 (31%) patients developed late-onset VAP. The incidence of VAP increased with the duration of MV. The mean duration of MV in cases without VAP was 13.5 days as against 23.4 days in patients with VAP ( P < 0.05). In addition, it may be noted that the mean duration of MV in patients with late-onset VAP was 29.25 days ( P < 0.005). Thus, it emphasizes a direct correlation between the duration of MV and development of VAP. The average length of stay in CCU for patients who developed VAP was 28 days (σ =18), whereas the average for non-VAP patients was appreciably low at 19 days (σ =13) ( P < 0.05). [Table - 3] shows correlation between patient related factors and Incidence of VAP. It also highlights the association between the severity of illness, assessed by APACHEIII scores on admission, and VAP. Patients with VAP had an average APACHEIII score of 55.1, compared with non-VAP group, whose score was 41.75 ( P < 0.05) The comorbid conditions played a major role in CCU complications. Patients who developed VAP were more likely to be suffering from conditions causing immunosuppression, such as chronic renal failure, diabetes mellitus, and steroid therapy. These patients were presumably harbouring infections prior to admission. PaO2/FiO2 ratio was compared in both the groups (VAP and non-VAP) and was significantly lower in VAP group ( P < 0.001). PaO2/FiO2 ratio was assessed daily during the course of ventilatory support and it was observed that the ratio dropped at least 12-24 h prior to onset of clinicoradiologic picture suggestive of VAP. Patients who were diagnosed ARDS on basis of PaO2/FiO2 ratio being less than 200, were excluded from this comparison of PaO2/FiO2 ratio. Thus a decline in PaO2/FiO2 ratio was found to be an early indicator of the onset of VAP. [Table - 4] relates the health-care factors to the VAP. Out of 24 cases, who were reintubated, 19 developed VAP ( P < 0.001), whereas out of 11 patients, who had early and planned tracheostomy, only one developed VAP ( P < 0.005). [Table - 5] reveals the incriminating microbial flora. Gram-negative organisms were isolated from 26 out of 32 cultures. Most common offending organism isolated in cases with Early-onset VAP is Pseudomonas aeroginosa (60%) followed by Klebsiella and Escherichia coli . In patients with late-onset VAP, most common organism isolated was Staphylococcus aureus (26%), followed closely by P. aeroginosa , Klebsiella, E. coli , and Acinetobacter . The overall mortality rates were highest with Pseudomonas (42%), in spite of adequate and proper antimicrobial therapy, followed by S. aureus (33%) and others. Mortality was observed to be low in patients who were suffering from potentially remediable conditions, for example, tropical infections, organophosphorus poisoning, Guillain-Barre syndrome, etc. However, a much poorer prognosis was found to be associated with conditions such as sepsis/shock (67%), pancreatitis (100%), and conditions with CNS complications (e.g., hydrocephalus [75%], cerebral malaria [50%], or meningoencephalitis [50%]) [Table - 7]. [Table - 6] shows the clinical outcome and its relation with the factors related to patient and their course of care, e.g., age, presence of comorbid factors, infection or immunosuppression, reintubation, tracheostomy, and APACHEIII scores on admission. Nineteen patients out of fifty-one (37%) succumbed while being treated in CCU. Patients who died were slightly older in age (mean 38.7 years) as against the survivors (mean 31.1 years). Five patients were more than 60 years old and none of them could survive. Thus, mortality was significantly higher in older age groups. Mortality was also higher in the VAP group [Table - 8], though the difference was not statistically significant. The attributable risk percentage of VAP was 30.4% and the relative risk was 1.44. This analysis [Table - 6] demonstrated that mortality was significantly high in patients with comorbid illnesses ( P < 0.01) such as hypertension, chronic renal failure, metastatic malignancies, obesity, etc. Mortality was found to be predominantly related to underlying severity of disease which was assessed by APACHEIII scores within first 24 h of admission to CCU. Mean APACHEIII score on admission in survivor's group was 40.2, whereas it was significantly higher at 65 in nonsurvivors ( P < 0.001) [Table - 6]. Significantly ( P < 0.005) higher survival rates were found in cases that had early and planned tracheostomy, as compared with those who needed reintubations. Discussion VAP is the commonest nosocomial infection amongst patients receiving MV in CCU. The incidence of VAP in our setting was 47% and the incidence rate of VAP in our study was 26 per 1000 ventilator days. [Table - 9] shows the incidence of VAP, reported by recent studies (Torres, Kollef, and Fagon), ranging from 15.5% by Kollef et al. to 27.5% by Fagon et al. However, it may be noted that both these studies were of 2 and 5 years duration, respectively, with much larger number of patients studied, viz., 277 by Kollef and 1118 by Fagon. The total number of cases in our study is small. The higher incidence of VAP in our study could also be owing to the presence of comorbid conditions. The patients who succumbed were seriously ill with conditions such as septic shock, pancreatitis, cerebral malaria, etc. The health-seeking behavior of our patients is different compared with that in developed world. Owing to limited resources, patients seek medical help only when it is absolutely inevitable. By the time he is referred to the tertiary-care centre, his underlying condition is well advanced and may be irreversible. This may necessitate longer duration of MV, which is directly proportional to development of VAP. The other most important factor leading to higher incidence of VAP in our set-up may be attributed to the paucity of nursing staff that leaves lacunae in the ideal patient care. The patient to nurse ratio in our CCU set-up is 4:1, the desired ratio being 1:1. Reintubation has resulted in a very high incidence of VAP. An early and planned tracheostomy has shown significant reduction in occurrence of VAP, which is also advocated by many other reports in literature. Other risk factors identified were immunosuppression, use of chemical paralysis, and dialysis. This study also signifies that decline in PaO2/FiO2 ratio is an early indicator of onset of VAP. In summary, the significant risk factors for development of VAP were prolonged duration of MV, higher APACHEIII scores on admission signifying severe illness and reintubation. Other positive risk factors identified were presence of comorbid conditions causing immunosuppression/ infection, use of chemical paralysis, and use of dialysis during the course of CCU stay. The patients who acquired VAP had longer lengths of CCU stay as well as greater hospital mortality rates (37%). In our study, VAP was not independently associated with mortality, though mortality rate was higher in patients with VAP [Table - 8]. Mortality was predominantly associated with underlying severity of disease, presence of comorbid factors, and older age groups. APACHEIII scores within first 24 h of admission to CCU were used to address the underlying severity of illness. Patients who developed VAP had statistically higher APACHEIII score at admission (55) as compared with patients without VAP (42). Likewise, patients who died had even higher scores (65), ( P < 0.001). Thus, APACHEIII score at the time of admission was found to be a useful parameter to prognosticate patients on arrival and also during their course of stay. [Table - 10] demonstrates that our CCU has particularly high incidence of pneumonia caused by Pseudomonas and Klebsiella as compared with other studies. Also, we found that incidence of polymicrobial flora was higher in tracheal aspirate culture. Furthermore, mortality rates were higher with Pseudomonas followed by Staphylococcus and Klebsiella . Also, it was observed that pathogens isolated were potentially antibiotic resistant. We could not study Susceptibility profile in detail owing to paucity of clinical microbiology support and unaffording patients but, recounting our experience, our findings are as follows. Pseudomonas was isolated in 11 samples and was found to be maximally susceptible to meropenem and cefpirome. Pseudomonas showed favorable susceptibility pattern to piperacillin, cefoperazone-sulbactam, and amikacin whereas it was fairly resistant to drugs such as levofloxacin, ciprofloxacin, and ceftazidime. K. pneumoniae was isolated in seven samples and showed maximal susceptibility to meropenem, cefpirome, and cefoperazone-sulbactam. Klebsiella was moderately susceptible to piperacillin and ciprofloxacin and was highly resistant to amoxicillin-clavulanate, cefotaxime, ceftriaxone, and ceftazidime. S. aureus was isolated in six samples and all isolates were resistant to methicillin and amoxicillin-clavulanate. Staphylococcus showed excellent sensitivity to vancomycin and teicoplanin. Linezolid was used only in one patient who did not respond well to vancomycin. Conclusions We arrive at the following conclusions:
References
Copyright 2005 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm05033t3.jpg] [cm05033t8.jpg] [cm05033t5.jpg] [cm05033t2.jpg] [cm05033t9.jpg] [cm05033t7.jpg] [cm05033t4.jpg] [cm05033t6.jpg] [cm05033t1.jpg] [cm05033t10.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}