 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
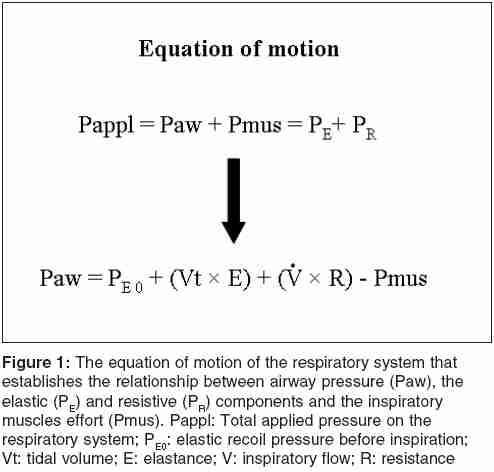
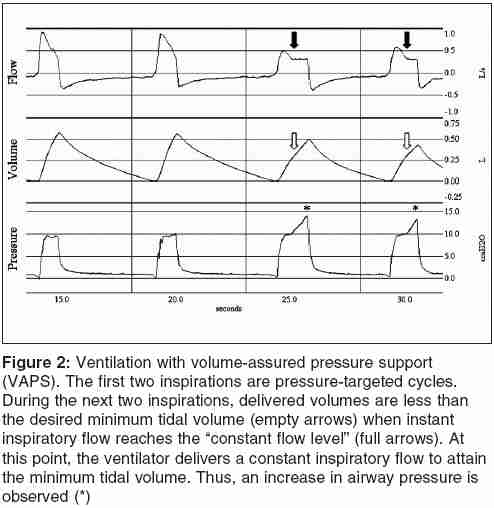
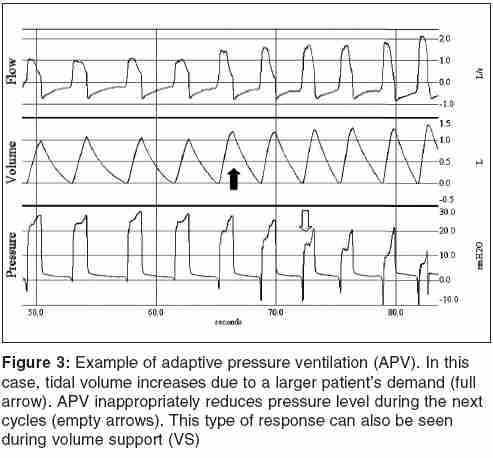
Indian Journal of Critical Care Medicine, Vol. 9, No. 4, October-December, 2005, pp. 235-243 Review Article Mechanical ventilation: changing concepts Rodriguez Pablo,1 Dojat Michel,2 Brochard Laurent1 Service de Réanimation Médicale, Hôpital Henri Mondor; INSERM U615, Université Paris 12, Creteil Code Number: cm05036 Abstract Mechanical ventilation is routinely delivered to patients admitted in intensive care units to reduce work of breathing, improve oxygenation, or correct respiratory acidosis. Although traditional modes of mechanical ventilation achieve many of these goals, they have important limitations. Alternative modes are supposed to handle some of these limitations and are now available on modern ventilators. This article reviews general aspects of functioning and limitations of traditional modes of mechanical ventilation, and the potential interest of some new promising modes.Keywords: Acute respiratory failure, Mechanical ventilation, Ventilator modes Introduction Mechanical ventilation is frequently delivered to patients admitted in intensive care units (ICU) to reduce work of breathing, improve oxygenation, or correct respiratory acidosis. Common indications, according to a multinational survey involving more than 5000 patients, are acute respiratory failure (69%), coma (17%), acute on chronic respiratory failure (13%), and neuromuscular disorders (2%).[1] In most cases, ventilator is set to completely control patient's ventilation shortly after intubation. The objective is to improve oxygenation without inducing damage to the lungs and to put the respiratory muscles at rest. Afterwards, when patient's condition begins to improve, his or her ventilation is assisted by the ventilator until extubation. This can be done with all traditional modes at variables degrees.[2] Although this seems logical, there is no clear consensus about when, how and at which level patient's work of breathing should be reduced. Insufficient assistance may induce diaphragmatic fatigue or weakness and force the recruitment of accessory inspiratory muscles, sometimes leading to respiratory acidosis.[3],[4] Excess in assistance may induce respiratory alkalosis and reduce respiratory drive, facilitating the appearance of patient-ventilator asynchronies and sleep disruptions.[2],[5],[6],[7] In this article, we will review new insights in some new promising alternative modes of ventilation aimed to improve the adaptation of the ventilator to patient's respiratory demand, including proportional assist ventilation, adaptative support ventilation, and knowledge-based systems. Traditional Modes of Mechanical Ventilation Modes of ventilation summarize the way assistance is applied to patient's respiratory system by the ventilator. They are usually defined by control and phase variables.[8] Control variables are flow (or volume) or pressure. When using traditional modes, ventilators control only one variable (flow/volume or pressure). The other one (pressure or volume) reflects patient's effort and respiratory system mechanical properties according to the equation of motion of the respiratory system [Figure - 1]. Phase variables refer to how respiratory cycle is "handled" by the ventilator: change from expiration to inspiration, inspiration, change from inspiration to expiration and expiration.[8] Inspiration starts when a signal reaches a specific threshold value: time (set respiratory rate) in the case of controlled ventilation and pressure or flow trigger for assisted ventilation. Thereafter, the control variable (flow or pressure) increases up to a predefined limit and is maintained at this level until the end of inspiration. In the case of flow control mode, inspiration finishes after a fixed inspiratory time or after delivering a defined volume. On the other hand, the end of inspiration in pressure modes is defined by time pressure controlled ventilation (PCV) or when inspiratory flow reaches a predefined threshold pressure support ventilation (PSV). Finally, pressure during expiration can be controlled until next inspiratory cycle, allowing the delivery of positive end expiratory pressure (PEEP). "Traditional" modes are frequently chosen by clinicians. According to international surveys, assist control ventilation (ACV), PCV, synchronized intermittent mandatory ventilation (SIMV) and PSV are largely preferred.[1],[9] ACV, the most frequently used mode, allows a precise control of tidal volume and minute ventilation.[10] This is especially important during the initial phase of mechanical ventilation, when patient's effort must be largely reduced and oxygenation needs be improved. ACV is a flow (or volume) controlled and time (or volume) cycled mode. Consequently, airway pressure is not controlled during inspiration, and depends on the equation of motion of the respiratory system. This is not very troublesome during controlled ventilation, because airways pressures, especially plateau pressure, can be easily monitored. Adaptation is usually facilitated by sedation at the beginning of mechanical ventilation. Sedation is also needed to facilitate tolerance to particular settings such as small tidal volumes used in patient suffering from acute respiratory distress syndrome.[11],[12] However, continuous and deep sedation has been associated with increased duration of mechanical ventilation and length of stay in the ICU.[13] Fixed settings of inspiratory time, flow, and tidal volume during assisted ventilation with ACV can be very difficult to tolerate for patients having a high respiratory drive. For example, early auto-triggering (double cycling) may happen if patient's inspiratory time is larger than ventilator time.[14] Insufficient flow during ACV may be perceived as a resistance to inflow by the patient and increases patient's effort.[15] Pressure-targeted modes, such as PSV, can overcome some of the limitations observed during ACV. PSV is a patient-initiated, pressure controlled and flow cycled mode.[16] This means that pressure assistance is constant whatever patient's effort is and proportional to the level of pressure support.[2] Inspiratory flow is variable and decelerating. It depends on patient's effort and on his (or her) respiratory mechanics (airway resistance and respiratory system elastance). Cycling off criteria (from inspiration to expiration) is usually reached when inspiratory flow attains a predefined threshold. This value is usually expressed as a percentage of peak inspiratory flow and can be manually set in some ventilators. Standard setting is 25% of peak inspiratory flow. Additionally, a maximal inspiratory time can be set in some ventilators, introducing a conditional time cycling variable, similar to PCV. This may be of interest in the presence of leaks, as shown during non invasive mechanical ventilation for avoiding prolonged inspirations and patient-ventilator asynchrony.[17] Altogether, these features may give the patient the opportunity for choosing his (or her) tidal volume, inspiratory time, and flow. This makes PSV suitable for assisted mechanical ventilation. It has also been proved to been useful for weaning.[18],[19] Several drawbacks related to its characteristics have been stressed for PSV, making setting not so easy as previously envisaged.[20] First, setting the level of pressure support is still a matter of discussion. Normally, it is set to obtain a respiratory rate within a desired interval, a certain tidal volume and to abolish accessory muscle utilization.[16] This is furthermore complicated by the fact that severe and maybe unacceptable patient-ventilator asynchronies have been reported with high level of assistance.[2],[21] Second, without intervention pressure support will be always the same whatever patient's respiratory demand. This prompts to a frequent need for re-evaluations of the patient's and monitoring of alveolar ventilation (minute ventilation and PaCO2). Third, pressure rise time is also important. Low pressurization rates increase patient's effort, whereas very high rates may induce cough and are frequently experienced as uncomfortable.[22] Finally, cycling off criteria (also called expiratory trigger) may also play a role in terms of patient-ventilator interaction.[14] As previously stated, some ventilators allow changing the cycling off criteria. Although it is not still clear which flow value must be used, some ventilator only propose fixed algorithms that may increase the risk of delayed cycling (e.g., 5 l/min for Puritan Bennett 7200 [Tyco Healthcare, Mansfield, MA] and 5% for Siemens 300 [Siemens Medical Systems Inc, Lund, Sweden]).[16] Different criteria may be needed in patients showing a high respiratory drive and shorter neural inspiratory times, such as patients with obstructive lung disease.[14] Additionally, these patients may show recruitment of expiratory muscle during late ventilator inspiration.[23] This may further promote an increase in dynamic intrinsic PEEP and, as a consequence, may decrease the likelihood to recognize next patient's effort.[24] Improving Patient and Ventilator Matching "Alternative" modes were developed to improve matching between patient's ventilation demand and ventilator supply. In the vast majority, they are modification of "traditional" modes, which take advantage of ventilator microprocessor to adapt assistance to reach specific objectives. This can represent different levels of complexity, from just assuring a predefined minute ventilation or tidal volume to a complex adaptation of assistance according to respiratory pattern or physiological variables. In the next paragraph, we discuss the interest, clinical evaluation, and limitation of alternative modes aimed to improve the interaction between patient and assistance delivered by the ventilator. Dual-control Modes Dual-control modes can be seen as basic algorithm based closed-loop modes. In almost all cases, airway pressure is the controlled variable, which is adjusted to attain a specific tidal volume. This can be done within one single inspiration or in a breath-to-breath fashion. The objective is simple: better adaptation to changes in respiratory mechanics in case of assisted ventilation, and control of airway pressure while assuring minute ventilation. Potentially, this can improve patient's comfort and reduce the necessity of frequent modification in ventilator settings. However, as we will below, basic dual-control modes present several problems sometimes putting patients at risk. Additionally, published clinical experience with these modes is scarce. Volume-assured pressure support (VAPS) is an example of dual mode, which adapts within one cycle. It has been described more than 10 years ago and has been included in Bird 8400 and T-Bird (Bird Corp, Palm Springs, CA).[26] Specific settings are minimum tidal volume, respiratory rate, pressure support and "constant flow" level. Inspiration can be triggered by time (controlled cycle) or by the patient. At the beginning, the ventilator delivers gas to increase airway pressure, behaving as in PCV or PSV. As in pressure controlled modes, flow decreases progressively until a predefined level ("constant flow"). At this point, if inspiratory tidal volume is equal or greater than predefined minimum tidal volume, then inspiratory valve closes and expiration begins as in PSV. However, if inspiratory tidal volume is smaller, then inspiration will continue with a constant flow until the minimum tidal volume is delivered without further pressure control.[25],[26] This may dangerously increase inspiratory time, predisposing the patient to gas trapping (intrinsic PEEP) and phase asynchronies when patient's effort is reduced [Figure - 2]. Although one short term physiological study showed improvements in work of breathing and synchronisation compared with ACV,[26] there are no data about long term utilisation of this mode. Volume support adjusts pressure support to attain a predetermined tidal volume and while maintaining minute ventilation in a breath-to-breath basis. It was originally included in Servo 300 (Siemens Medical Systems Inc, Lund, Sweden) and is actually available in Servoi (Maquet Inc, Solna, Sweden). It is an assisted, pressure controlled and flow cycled mode as PSV. Specific settings are desired tidal volume and respiratory rate. Initially, ventilator calculates patient's dynamic compliance during a test breath with 5 cm H2O of pressure support. Thereafter based on this "constant," it calculates the pressure needed to produce set tidal volume. Changes cycle to cycle can be less than 3 cm H2O, going from PEEP to 5 cm H2O below maximal peak inspiratory pressure. Another rule can increase target tidal volume when patient's respiratory rate is less than set respiratory rate to keep minimum minute ventilation constant. Volume support "correctly" increases assistance when tidal volume is reduced, as can be observed in patients with increasing airway resistance or rapid shallow breathing. If, however, the patient increases his or her effort (and tidal volume) to compensate an increment in respiratory demand as can be seen in fever or acidosis, it will paradoxically decrease assistance [Figure - 3]. The latter has been recently showed in a physiological study conducted in patients exposed to increases in dead space.[27] Some pressure controlled and time cycle modes have been introduced by manufacturers. They share many characteristics of volume support. Some examples are pressure-regulated volume control (PRVC) available in Servo ventilators, Adaptive Pressure Ventilation from Galileo (Hamilton Medical AG, Bonaduz, Switzerland) and Autoflow from Evita 4 (Dr&δger, Lübeck, Germany). They just adjust airway pressure to attain specific target tidal volume and minute ventilation. As in volume support, when faced with increases in patient respiratory effort that may increase tidal volume, the ventilator will actually reduce assistance [Figure - 3]. Similarly to the other dual-control modes, published experience is very limited.[28],[29]
Proportional Assist Ventilation Several physiological studies showed that PAV efficiently decreases respiratory effort.[31], [33],[34],[35] It may also preserve physiological breathing pattern better than PSV, allowing a greater variability of tidal volume with different degrees of assistance.[36],[37] Additionally, PAV may significantly improve patient-ventilator matching compared with traditional modes of mechanical ventilation[38] and may increase comfort.[39],[40] Some investigators have evaluated the utility of PAV over prolonged periods during non invasive mechanical ventilation: no major side effect was noted and data suggested that it might be better tolerated. [40],[41],[42],[43] Less refusals to continue mask assistance were observed with PAV in a randomized study.[40] Several drawbacks have been signaled for PAV. As it was previously described, elastance and resistance must be known by the ventilator to work correctly. This may be difficult during assisted ventilation. If incorrect high values are introduced and high percentage of assistance is used, the ventilator can overassist the patient and fail to recognize the end of patient breath. This situation is known as "runaway." Under these circumstances, the ventilator inspiration finishes when peak pressure alarm is attained or when patient expiratory effort is strong enough to correct the mistake.[32] Although runaways may not jeopardize patients if alarms are correctly set, it may create major phase asynchronies and discomfort. To overcome this problem, elastance and resistance can be calculated during flow controlled ventilation obtained with hyperventilation or brief sedation.[44] Another possibility is progressively increasing volume and flow assistance (gain) until obtaining a runaway. This allows recognizing the maximum tolerable values. This is frequently reported as the runaway method.[32],[45] However, these methods are not dynamic and if used, repeated measurement should be performed. Recently, new methods of non invasive intermittent measurements of elastance and inspiratory resistance during PAV have been proposed [Figure - 4].[46],[47] These methods are very promising and have been partially integrated in PAV offered by Puritan Bennett 840 (Tyco Healthcare, Mansfield, MA). However, larger long-term experience is needed to test its safety and efficiency. PAV is also affected by intrinsic PEEP, even if inspiratory trigger is set at the minimum value. The latter may induce ineffective efforts or reduce the total amount of patient's effort that is actually assisted, failing to correctly coupling patient inspiration to ventilator assistance. Ventilatory Assist Driven by the Patient Recently, some authors have proposed modes that assist in proportion to indicators of diaphragmatic activity. One approach using transdiaphragmatic pressure as driven signal was tested in healthy subjects exposed to different levels of inspiratory pCO2. The ventilator was well synchronized to subjects'efforts.[49] Although this mode may appear promising, transdiaphragmatic pressure signal sometimes is altered by cardiac artifacts or expiratory muscle interference possibly limiting its utility.[50] Another interesting approach is neurally adjusted ventilatory assist (NAVA).[51] It is a promising but still experimental mode of ventilation. It provides assistance in proportion to diaphragm effort. It depends on continuous recording of diaphragmatic electrical activity, which is obtained via a nasogastric catheter incorporating a multiple array esophageal electrode (nine electrodes spaced 10 mm apart). The onset and end of assistance and the level of assistance are directly driven by this signal.[52] In theory, NAVA should provide better patient-ventilator synchrony than other pressure-targeted modes. First results support this expectation. Unlike all other modes (including PAV), NAVA should not be influenced by intrinsic PEEP or by the presence of leaks as in the case of standard triggering systems. The initial report on NAVA revealed advantages compared with PSV in terms of triggering and cycling-off synchrony.[52] These first physiological results are encouraging. Adaptive Support Ventilation When starting ventilation in ASV, the ventilator provides three pressure control time cycle inspirations, and calculates respiratory mechanics. Expiratory time constant is estimated from the tidal volume curve during each expiration.[55] Then, using Otis's formula, a target respiratory rate is calculated. Target tidal volume is computed from minimum minute ventilation and target respiratory rate. Thereafter, target values are calculated cycle by cycle. Depending on patient's spontaneous respiratory rate, ASV can works as PCV, if there is no spontaneous breathing; as pressure SIMV, when patient's respiratory rate is smaller than target; or as PSV, if patient's respiratory rate is greater. Pressure level is then adapted to attain the target tidal volume (within limits imposed by pressure alarms). Cycling off criteria is flow based in the case of assisted ventilation or time based for mandatory inspiration.[53] There is not much published experience with ASV. Most studies are short term and during the postoperative period.[56],[57],[58],[59],[60] All these studies showed promising results, including decrease of patient's respiratory efforts, stability of alveolar ventilation without operator's intervention and safety during weaning in selected situations. However, many important unsolved questions remain to be answered for ASV: how minimum ventilation must be set, how ASV must be adapted faced with changes in breathing demand and how weaning must be handled. Knowledge-based Systems The Smart Care ® system, which is now included in Evita XL (Dräger, Lübeck, Germany), is an embedded version of the initial NeoGanesh system.[64] The NeoGanesh system drives the ventilator with PSV, keeping a patient within a zone of "respiratory comfort" defined by respiratory parameters. Additionally it is capable of superimposing an automated strategy for weaning.[64],[65] The NeoGanesh system is based on modeling of the medical expertise required to perform mechanical ventilation in PSV mode. It does not include mathematical equations of a physiological model. Several types of evaluation have been performed to determine how well the system adapts the level of assistance to patient needs (evaluation of the control level),[65] to assess the extubation recommendation made by the system (evaluation of the strategic level)[64] and to estimate the impact on clinical outcomes.[66] This system has been shown to reduce periods of excessive respiratory efforts and to predict extubation time with good accuracy. It has been used safely during prolonged periods of mechanical ventilation and has been shown recently to reduce the time spent on the ventilator.[67] Conclusion Traditional modes of mechanical ventilation provide adequate control of ventilation in most cases. However, as it was previously described, they may present many problems to the clinician facing a spontaneously breathing patient. New modes such as PAV, ASV or knowledge based system are now available and seem very promising to help to improve adaptation during assisted ventilation. However, before recommending their use, further studies are needed to better characterize clinical interest and to target the population that might take advantage of its implementation.References
Copyright 2005 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm05036f4.jpg] [cm05036f1.jpg] [cm05036f2.jpg] [cm05036f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}