 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
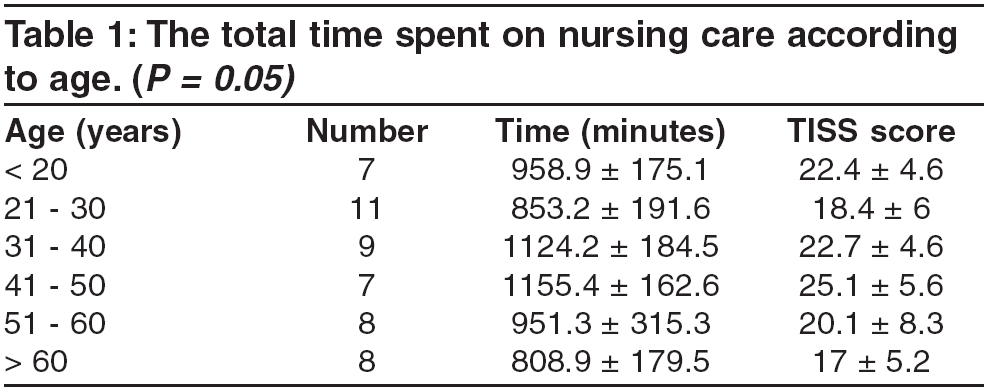
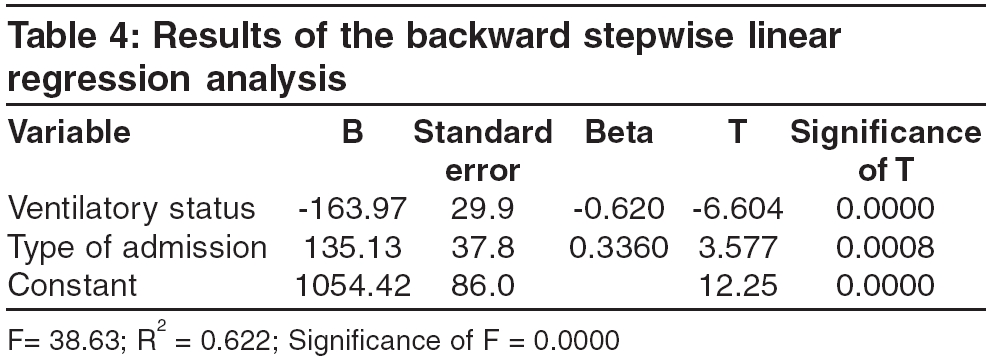
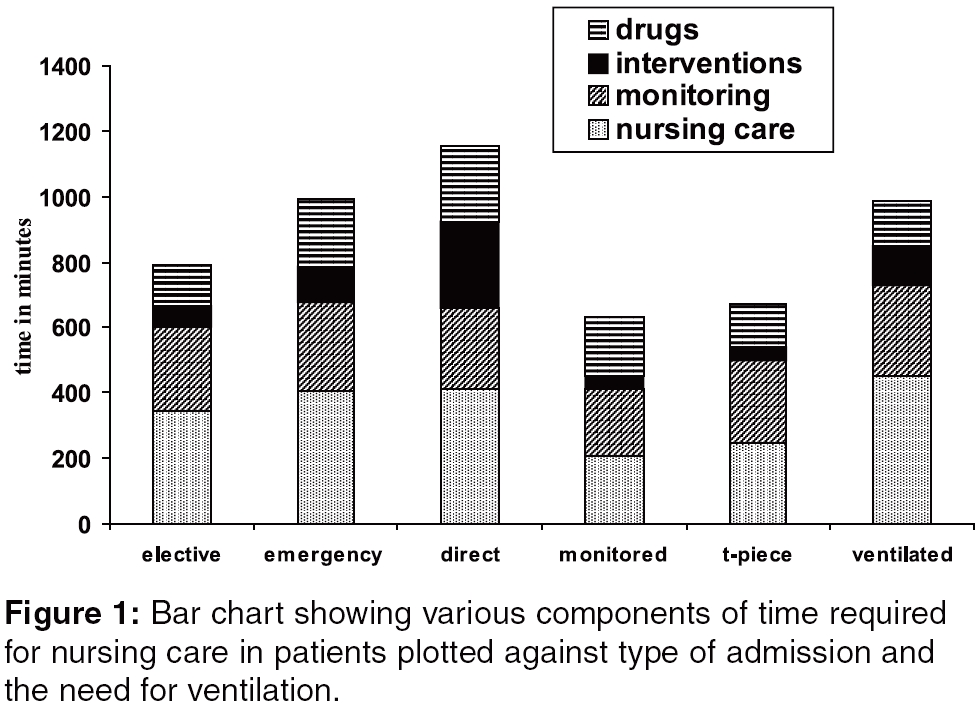
Indian Journal of Critical Care Medicine, Vol. 10, No. 1, January-March, 2006, pp. 15-20 Original Article Factors influencing nursing care in a surgical intensive care unit J. P. Raj, Nagamani Sen, K. R. John* From: Departments of Surgical Intensive Care Unit and *Community Health, Christian Medical College, Vellore, India Correspondence Address:John Prakash Raj, Surgical Intensive Care Unit, Christian Medical College, Ida Scudder Road, Vellore - 632 004, India. E-mail: johnprakash.raj@cmcvellore.ac.in Code Number: cm06002 Abstract Context: The total time spent in nursing care depends on the type of patient and the patient's condition. We analysed factors that influenced the time spent in nursing a patient. Keywords: Time, nursing nare, ICU, nursing time, allocating time. In an intensive care unit, the health care professional who spends maximum time with the patient, is the ICU nurse. To ensure that the patient's needs are adequately taken care of, a nurse to patient ratio of one is to one, is needed. There are occasions when this ratio may not be adequate.[1],[2],[3] We are in an age where critical care medicine is costly[4],[5],[6],[7] and where specialised nursing personnel are scarce.[1] In such a situation, providing adequate care to a patient is difficult. Often the nurse to patient ratio becomes less than ideal, compromising on the quality of care.[2],[3] With such a background, it is important to optimise the time a nurse spends with a patient. This would lead to utilisation of a minimum number of nurses, without compromising on the quality of care delivered. Studies on the time spent by nurses on patients have been done in the past. [8],[9],[10],[11],[12],[13] Several scoring systems like the Therapeutic Intervention Scoring System (TISS),[14] the Time Oriented Scoring System (TOSS)[15] and the Nursing Care Recording System (NCS)[11] have been devised, both to measure and to predict the amount of time, a nurse needs to give in the care of each patient. These scoring systems help to estimate the amount of time required for nursing care. While studies have been done on the time a nurse spends in the ICU,[8],[9],[15] few studies have been done to determine factors that may influence this time. Such factors may include the need for mechanical ventilation, number of medications to be administered and procedures performed. In addition, the time spent by the nurse may also be influenced by the age of the patient, the disease and interventions that may be required. Severity scores like the APACHE II score,[16] the SAPS score,[17] indicate the severity of illness. However, they give very little indication of the factors that may influence the time involved in nursing a patient with a particular score. Knowledge of this type would be useful, to help in planning nursing care of patients in an ICU. This study was done in a ten-bedded Surgical ICU of a tertiary care centre. The surgical ICU receives about 900 admissions every year. The average length of stay of patients is about 2.3 days. A total of 21 nurses including the head nurse, staff the unit. This works to a nurse- patient ratio of 1:2, at the best of times. Improving this ratio would mean an increased cost, both to the patient (who funds his treatment) and to the hospital. It was therefore important to use the time available for nursing care efficiently, to ensure adequate patient care. The study was done with the objective of measuring the total amount of time that a nurse spends on each patient and the various components of that time. We also analysed the various factors that played a role in the utilisation of this available time. Knowledge of these factors would help in more optimal utilization of nursing resources. Materials and Methods Fifty consecutive patients who were admitted into the Surgical Intensive Care Unit during a one month period, were included in the study. This study was done with the permission of the institution's Research Committee. As the study did not involve patients, informed consent was not required. Consent of the nurses studied, was not taken to avoid bias. Before starting this study, every nursing procedure was timed and an average of ten such timings was taken. Since all nurses follow standard protocols for each procedure in the ICU, there was very little change in the time for each procedure, between nurses. At admission, the patient's name, age and sex were recorded. Patients were categorised into three types of admission: following elective surgery; following emergency surgery and direct admissions from the ward or the Emergency Room (ER). The need for mechanical ventilation was noted. Admissions with an endotracheal or tracheostomy tube in situ, were also recorded. Interventions carried out were also recorded. The total time a nurse spent on a patient for the first twenty-four hours of stay in the ICU, starting from the moment the patient was transferred to the ICU, was recorded. The first twenty-four hours was taken, because we felt that the most interventions are carried soon after admission and the nursing input is maximum during that period. The time that a nurse spent for the first 24 hours after admission, was calculated by listing the procedures done during that period and using the average time that had been calculated earlier. This time was recorded under four categories: the time taken for routine nursing care; the time taken for monitoring; the time taken for administering medications and the time taken for interventions. Where an intervention like a central venous line, tracheostomy or endotracheal intubation was done, the actual time spent by the nurses was recorded. In addition, the time taken in admitting or discharging (if a patient was discharged within 24 hours), was recorded. If a patient died within twenty-four hours of admission, the time taken for death care was recorded. During this period, the actual time taken for various procedures was timed at random intervals, to ensure that there was no variation from the average calculated earlier. The time spent by nurses on breaks or administrative work not connected with patient care, was not included in the time taken for patient care. The TISS score for each patient during the first twenty-four hours was calculated for each patient. Statistical analysis The results were analysed by using age, sex, the diagnosis, the type of admission and the need for ventilation as variables. These were compared with the total time taken, the time taken for routine nursing care, the time taken for monitoring, the time taken for administering medication, the time taken for interventions and the TISS score. Analysis of variance (ANOVA) tests were done to determine significance. A probability of < 0.05 was considered significant. A backward step wise linear regression analysis using these variables was done, to determine the influence each of these variables had on the total time. All values are expressed in minutes, ± standard deviation. Results 1. Total time Age Sex Primary diagnosis The type of admission Time spent on ventilated patients 2. Time for routine nursing care 3. Time taken for monitoring Time taken for interventions Time taken for administering medications Multiple regression Discussion The above results show that the type of admission and the need for ventilation, appears to be the main factors influencing the time a nurse requires for the care of a patient. While the sex of the patient did not appear to influence the total time, younger patients required more time for nursing care, regardless of their underlying condition. This agrees with another study done in an ICU, where patients who were more than 75 years of age had a lower TISS score, than younger patients. This was seen even when factors like severity, need for mechanical ventilation, mortality rate and the disease process were taken into account.[18] Patients who were admitted after emergency surgery, or directly from the wards, required significantly more time than patients admitted after routine, elective surgery. Looking at the break up of time consumed in various nursing activities [Figure - 1], there was no difference between the two groups in the time taken for routine nursing care (409.1 ± 107.3 versus 349.7 ± 127.7 minutes; P =0.21) and monitoring (270.4 ± 21.2 versus 257.3 ± 47.9 minutes; P = 0.5). However, these patients required significantly more time for interventions and medications. The TISS score in these patients were also significantly higher. Interventions such as inserting intravascular lines and intubations (for direct admissions), accounted for most of the time taken in these patients. These patients were more likely to be on ionotropic supports, multiple antibiotics and were more likely to require transfusion of blood and blood products. These contributed to the increased time required for medications. Patients who were ventilated, required significantly more time than patients who were either brought extubated, or brought with an endotracheal tube or tracheostomy in situ. These patients required more time for routine nursing care (450.5 ± 58.8 versus 227.2 ± 71.7 minutes; P = 0.0000). These patients also required more time for interventions and medications. Ventilated patients were more likely to be sedated than non ventilated patients. This necessitates more frequent back care and attention, consuming more time. Moreover, there were more patients who were ventilated following an emergency surgery, than after an elective surgery. Seventy-nine percent of the patients who were admitted after an emergency surgery required ventilation, whereas 53% of the patients after an elective surgery, required ventilation. A patient who has undergone elective surgery and is brought for extubated to the ICU for monitoring only will require about 558 minutes (9 hours, 18 minutes). While such patients ideally require a high dependency unit and not intensive care, they may be admitted to the ICU in the absence of a dedicated high dependency unit. For these patients, a nurse to patient ratio of 1:2 or even 1:3, may be adequate. On the other hand, a patient who comes directly from the ward and requires ventilation, will need about 1258 minutes (20 hours, 58 minutes) of nursing care per day. Here, a 1:1 ratio is mandatory and occasionally extra help may be required to ensure adequate care of this patient. We believe that this study will be useful in the planning of nursing care in the ward. The time required for various types of patients can be easily calculated just by knowing the type of admission and the ventilatory status of the patient. The allocation of patients to a particular nurse can be done, depending on the time required. This would help in optimising both, the care offered as well as the number of nurses needed to staff the ICU. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06002f1.jpg] [cm06002t3.jpg] [cm06002t4.jpg] [cm06002t2.jpg] [cm06002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}