 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
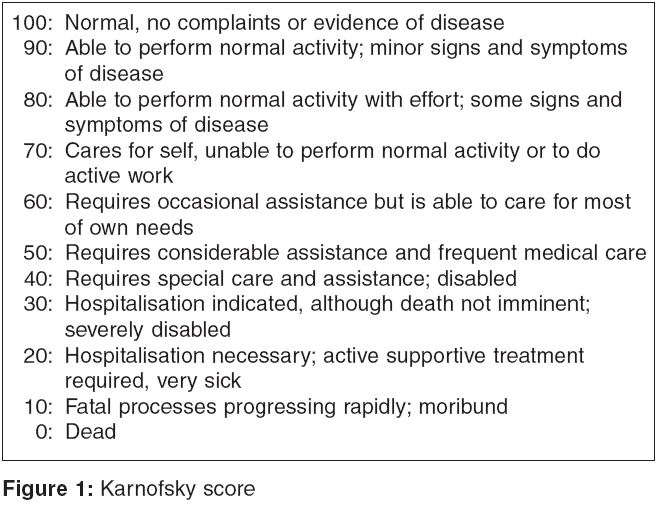
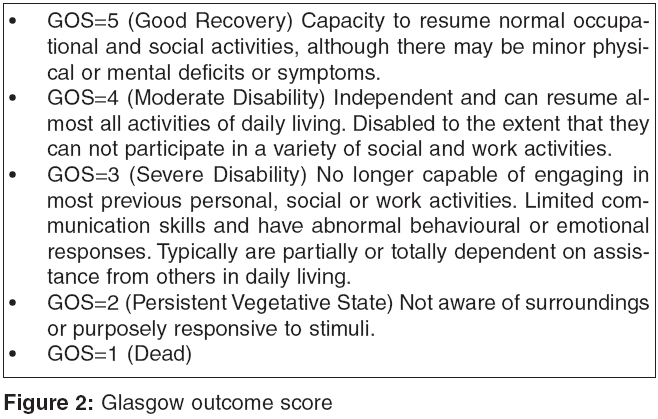
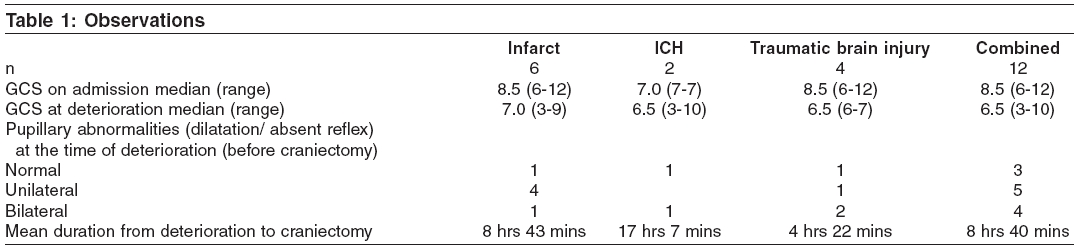
Indian Journal of Critical Care Medicine, Vol. 10, No. 1, January-March, 2006, pp. 21-24 Original Article An audit of decompressive craniectomies F. N. Kapadia*, V. A. Masurkar, M. S. Sankhe**, R. D. Gursahani*** From: Department of Intensivist *Critical Care Medicine, **Neurosurgery and ***Neurology, P. D. Hinduja National Hospital and Medical Research Centre,Mumbai, India Correspondence Address:Dr. Vikram Masurkar, 4-6/19, Talmakiwadi, Javji Dadaji Road, Tardeo, Mumbai - 400 016, India. E-mail: drmasurkar@hotmail.com Code Number: cm06003 Abstract Background: The management of acute intracranial hypertension refractory, to the medical management, remains a challenging endeavour. Mortality and morbidity rates remain high despite optimal medical management. Decompressive craniectomy has been proposed as an effective treatment for patients who have raised intracranial pressure (ICP) refractory, to the medical management. This study examined the outcome of patients who underwent this procedure.Aim: To assess the outcome of patients who underwent decompressive craniectomy. Materials and Methods: We conducted a prospective audit of consecutive patients of one neurosurgical unit, who underwent decompressive craniectomy at a tertiary care centre between 01/01/2004 to 31/03/2005. A complete neurological assessment, including Glasgow coma scale (GCS) and pupils was done and recorded at the time of admission, deterioration, post-op one wk and post-op three wks. End points were Glasgow outcome score (GOS) and Karnofsky score at 30 days, at discharge and at 6 months. Results: We studied 12 patients who were aged 30 to 69 yrs (Mean = 47 yrs). Unlike most interventions in critical care, survival is not an acceptable single end point. Good recovery ( Karnofsky score ≥80 / GOS≥4) was seen in five patients. Three patients were alive with severe disability ( Karnofsky score 1-70 / GOS 2-3), at follow up. Four patients died (Karnofsky score 0 / GOS 1). Conclusion: Eight patients who underwent decompressive craniectomy survived. Five of these patients had a good recovery. The other three survived with severe disability. Keywords: Decompressive craniectomy, raised intracranial pressure, intracranial hypertension. A subset of patients with ischaemic stroke, intracerebral haemorrhage (ICH) and traumatic brain injury suffer a progressive deterioration, secondary to massive cerebral ischaemia, oedema and increased intracranial pressure (ICP), despite well conducted medical treatment. The Brain Trauma Foundation guidelines recommend decompressive craniectomy as a second-tier therapy in refractory intracranial hypertension.[1] Aim To assess the outcome of patients who underwent decompressive craniectomy.Materials and Methods We conducted a prospective audit of consecutive patients of one neurosurgical unit, who underwent decompressive craniectomy at a tertiary care centre, between 01/01/2004 to 31/03/2005. A complete neurological assessment, including Glasgow coma score (GCS) and pupils was done and recorded at the time of admission, deterioration, post-op one wk and post-op three wks. The end points were Glasgow Outcome Score (GOS) and Karnofsky Score [Figure - 1][Figure - 2]. These were calculated at 30 days, at the time of discharge, and at 6 months. Operative technique The frontotemporoparietal hemicraniectomy adopted at our centre involved aggressive bone with removal, to provide good decompression. The bone removal was always more than 12 cms x 10 cms, with removal of the squamous temporal bone till the middle cranial fossa base. The temporal bone removal helped relieve pressure over the temporal lobes, thereby avoiding pressure over the midbrain. The dura was opened in a cruciate manner to reach the middle cranial fossa base and left open. The scalp was then closed. Results We studied 12 patients. They were aged 30 to 69 yrs (Mean = 47 yrs). Nine patients were males and three were females. The results are shown in [Table - 1][Table - 2].Discussion Progressive brain oedema can cause the area of damaged brain to extend. Within the confined cranial vault, the oedematous tissue places pressure against the surrounding normal parenchyma. Decompressive craniectomy converts the closed, rigid cranial vault, into an "open box." The result is a dramatic decrease in ICP and a reversal of the clinical and radiological signs of herniation. Early decompressive craniectomy can limit the extension of the infarcted area. However, this surgical procedure is still controversial, because of the lack of clearly defined indications in literature. In a classic article in 1905, Cushing reported the use of this procedure, to relieve the pressure caused by an intracranial tumour.[2] Since then, surgical decompression has been reported as a treatment option for supratentorial cerebral ischaemia, cerebellar infarction, traumatic brain injury, intracerebral haematoma, subdural haematoma, oedema resulting from vasospasm secondary to subarachnoid haemorrhage, encephalitis, cerebral venous and dural sinus thrombosis.[3],[4],[5],[6] The management of patients with severely raised ICP is a challenge. Small and heterogeneously composed study groups, inadequately defined selection criteria, the absence of long term follow up evaluation and ongoing uncertainties over the influence of treatment-independent prognostic factors hamper subgroup evaluation and the comparative analysis of various treatment strategies. Patients undergoing decompressive craniectomy represent a rather heterogeneous population with a varying prognosis. Hence, analysing outcome and prognostic markers is difficult. Uhl et al studied 188 patients who underwent decompressive craniectomy for space occupying cerebral infarctions.[7] They found that pre-treatment variables have a profound impact on outcome. Unfavourable predictors were older age (>50 years) and the involvement of more than one vascular territory. The improvements that occur following decompressive craniectomy, result due to the fall in ICP and the rise in brain tissue oxygen (PtiO 2 ). Jaeger et al monitored intraoperative PtiO 2 during decompressive craniectomy in three patients.[8] In all these patients suffering from severely raised ICP, it was found that the PtiO 2 rapidly increased to non-hypoxic levels. Yoo et al showed that the reduction in ICP occurs in two steps, during bone flap removal and dural opening.[9] At our centre, we used clinical deterioration as a trigger for decompressive craniectomy. ICP was not monitored preoperatively in any patient due to the urgency of the situation and financial constraints in different circumstances. The mean GCS at the time of deterioration was worse in the group with intracerebral bleed. Nine patients had pupillary abnormalities at the time of deterioration. The duration between the time of deterioration and time of craniectomy, was shortest in the group with traumatic brain injury (Four hours and 22 mins). This was probably because these patients needed a craniotomy for the primary brain injury. Unlike most interventions in critical care, survival is not an acceptable single end point. Recovery with minimal disability is as important. We used outcome scoring systems to analyse the outcome in our patients. Good recovery (Karnofsky score ≥80 / GOS≥4) was seen in five patients. These patients had a median GCS of 9 (range 6-10) before surgery. Three patients were alive with severe disability (Karnofsky score 1-70 / GOS 2-3), at follow up. These patients had a median GCS of 6 (range 4-7) before surgery. Four patients died (Karnofsky score 0 / GOS 1). These patients had a median GCS of 3 (range 3-8) before surgery. In a study conducted by Albanese et al , the authors found that decompressive craniectomy allowed 25% of patients to obtain social rehabilitation, at one year.[10] Polin et al reported a good recovery in selected patients, in their case series. Good recovery and moderate disability for the patients who underwent craniectomies was 37% (13 of 35 patients), whereas the mortality rate was 23% (8 of 35 patients).[11] The only prospective randomised controlled trial (PRCT) in children published till date reported good outcomes. The authors, Taylor A et al concluded that when children with traumatic brain injury and sustained intracranial hypertension are treated with a combination of very early decompressive craniectomy and conventional medical management, it is more likely that ICP will be reduced, fewer episodes of intracranial hypertension will occur and functional outcome and quality of life may be better than in children treated with medical management alone ( P =0.046).[12] However, the value of this procedure in adults has not been proven in a PRCT. A European study titled RESCUEicp (Randomised Evaluation of Surgery with Craniectomy for Uncontrollable Elevation of Intracranial Pressure) is an ongoing multi-centre PRCT comparing decompressive craniectomy versus optimal medical management, for refractory intracranial hypertension. The Australian and New Zealand Intensive Care Society Clinical Trials Group is currently conducting a large prospective randomised multicentre study of early decompressive craniectomy for refractory intracranial hypertension. The results of these studies will throw light on the value of this procedure in adults. Conclusion Eight patients who underwent decompressive craniectomy survived. Five of these patients had a good recovery. The other three survived with severe disability.References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06003f2.jpg] [cm06003f1.jpg] [cm06003t1.jpg] [cm06003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}