 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
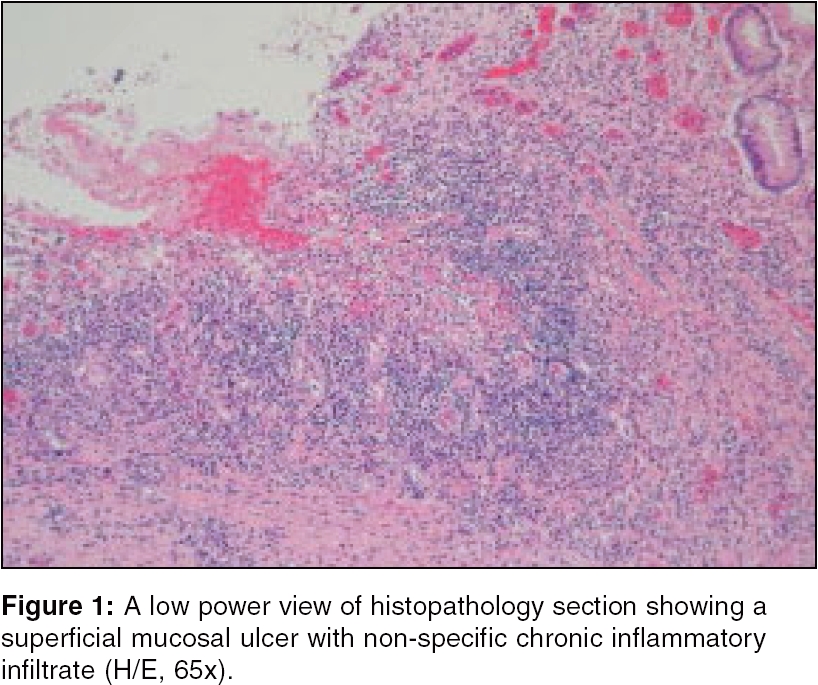
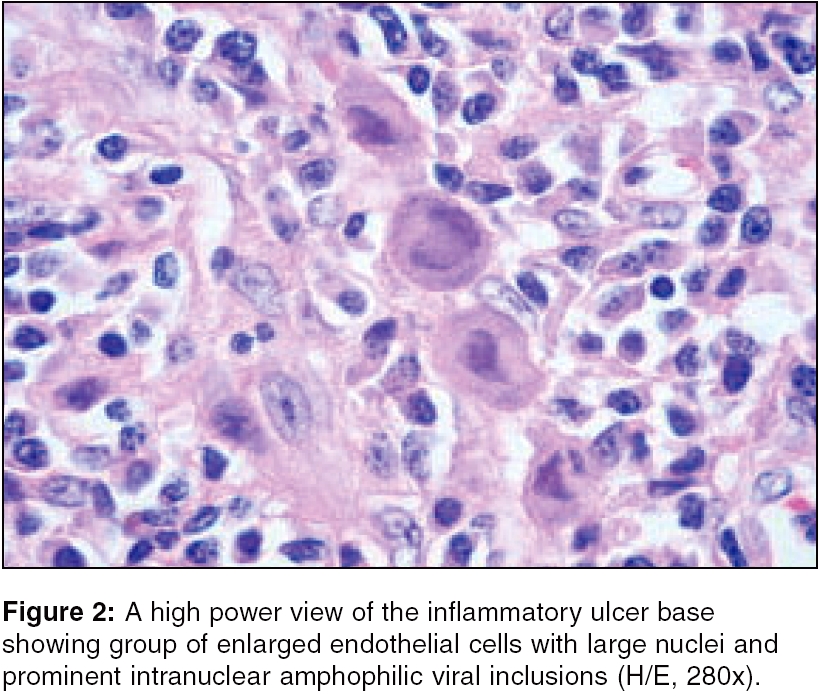
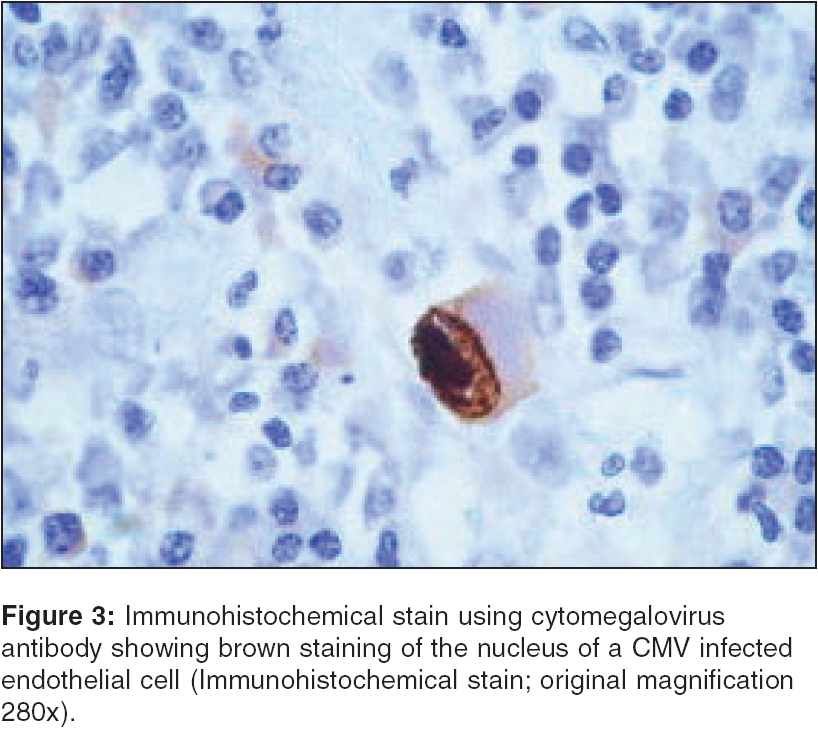
Indian Journal of Critical Care Medicine, Vol. 10, No. 1, January-March, 2006, pp. 40-43 Case Report Cytomegalovirus enteritis in a mechanically ventilated patient with chronic obstructive pulmonary disease F. Y. Khan, N. A. Morad* From: Departments of Medicine and *Pathology, Hamad General Hospital, Doha-Qatar Correspondence Address:Fahmi Yousef Khan, Department of Medicine, Hamad General Hospital, Doha-Qatar. E-mail: fakhanqal@yahoo.co.uk Code Number: cm06007 Abstract Massive lower gastrointestinal (GI) hemorrhage is a rare manifestation of GI cytomegalovirus (CMV) infection, in a critically ill patient. We report a 69-year-old man, known to have chronic obstructive pulmonary disease on ventilator, who developed sudden onset abdominal pain and massive lower GI bleeding. Due to uncontrolled bleeding, the patient was explored surgically. Bleeding from ileum was evident. The affected segment of the ileum was resected. Histology confirmed the diagnosis of CMV enteritis and Gancyclovir was initiated. On the following days, his physical state had improved and bleeding was resolved.Keywords: Cytomegalovirus , lower GI bleeding, enteritis. Cytomegalovirus (CMV) diseases occur almost exclusively in the immunocompromised hosts. Persons most commonly affected are patients with acquired immunodeficiency syndrome (AIDS). On rare occasions, however, CMV diseases can be seen in apparently immunocompetent persons. Case Report A 69-year-old man with a history of severe chronic obstructive pulmonary disease on home oxygen, was admitted with a 3-day history of worsening dyspnea and productive cough, with purulent sputum. He underwent multiple admissions to the medical intensive care unit (ICU), due to respiratory failure. Initial evaluation revealed an elderly man in moderate to severe respiratory distress, not able to speak in full sentences, with a BP 130/90 mmHg, Pulse of 110 beats/min; Lungs had decreased breath sounds, with occasional expiratory wheezing. Initial arterial blood gas analysis was as follows: PH, 7.25; PaCO2, 70; and PaO2 48. Chest radiograph showed hyperinflation, without infiltrates or pneumothorax. Neublized Bronchodilators, intravenous antibiotics and steroids were initiated. After one hour, on follow up, he became more dyspnic and the arterial blood gas showed a pH of 7.00, PaCO2 of 100 and PaO2 of 55. The patient was intubated and ventilated with assist control and volume control, for hypercapnic respiratory failure. Neublized Bronchodilators, intravenous antibiotics and steroids were continued. On the following days, the patient become stable and steroids were tapered, until stopped. Weaning failed on several attempts, due to many factors: first, advanced lung disease, second, generalized muscular weakness. Third, recurrent chest infection. On the 15th hospital day, the patient developed severe abdominal pain and massive lower gastrointestinal bleeding. Initial examination was notable for a temperature of 37.7°C, pulse of 113 beats/min, respiratory rate of 21/min and blood pressure of 100/60 mm Hg. He appeared ill and the examination of the abdomen revealed tenderness on the periumblical area without organomegaly. Rectal examination was positive for bright red blood. Initial investigations revealed a hemoglobin concentration of 8 gm/dL, WBC 4500/uL and platelet count of 200,000/uL. Blood chemistry, liver profile and coagulations studies, were within normal limits, as well as serum lipase and amylase. Hepatitis C antibody, hepatitis B markers and antibody to the human deficiency virus, were negative. Bacterial cultures of the stool were negative. Tagged red blood cell studies, endoscopy and angiogram failed to demonstrate any active eding site. Bleeding continued and despite the transfusion of several units of blood, the hemoglobin did not go up. During exploratory laporotomy, ilieal ulceration and bleeding were evident; the affected segment of the ileum was resected. Microscopically, resected terminal ileum revealed superficial mucosal ulcer with non specific chronic inflammatory infiltrate [Figure - 1], beneath the ulcer group of enlarged endothelial cells with large nuclei and prominent intranuclear amphophilic viral inclusions were found [Figure - 2]. Immunohistochemical stain using cytomegalovirus antibody revealed brown staining of the nucleus of a CMV infected endothelial cell [Figure - 3]. IgG antibody titer to CMV was low, but IgM titer was high and Gancyclovir was initiated. On the following days, his physical state had improved and bleeding was resolved. Discussion CMV is a member of the Herpesviridae family, which includes the Epstein-Barr virus (EBV), herpes simplex virus, varicella-zoster virus and herpesvirus 6, 7 and 8. CMV infection is worldwide and usually asymptomatic. Like other members of the Herpesvirus family, CMV establishes latent infection in the tissues of the human host after the resolution of acute infection, reactivating and shedding, when the host′s immune system is compromised. The proportion of humans with evidence of prior CMV infection varies throughout the world, with seroprevalence rates ranging between 40 to 100 percent of the adult population.[1] Seroprevalence generally correlates inversely with a country′s socioeconomic development, with highest rates observed in developing countries throughout Africa and Asia.[2] Secondary, symptomatic disease may present later in the life of the host, reflecting one of two possibilities: reactivation of latent CMV, or reinfection with a novel exogenous strain. CMV is not highly contagious. It is contracted from close personal contact with people who excrete the virus in their body fluids (e.g, saliva, urine, blood, breast milk, semen and even transplanted organ tissue). It also can be shed from the throat and uterine cervix.[3] Transmission can occur via multiple routes: during perinatal period or sexual intercourse,[4] close contacts,[5],[6] blood or tissue exposure[7] and occupational.[6] In our patient, there was no obvious source of infection and most probably the patient developed secondary disease due to reactivation of latent CMV. Cytomegalovirus (CMV) is an important human pathogen, causing a variety of syndromes ranging from asymptomatic infections to life-threatening end-organ disease.[8] The most common site of involvement by CMV infection in the GI tract, is the colon followed by the upper GI tract and the least common site is the small intestine.[9] Cytomegalovirus infections of the alimentary tract have been reported mainly in severely immunocompromised patients, or those with predisposing disorders such as ulcerative colitis.[10] Another risk factor includes, the critically ill patient.[11] Although GI bleeding is one of the major presenting symptoms of patients with CMV infections of the GI tract,[9] massive lower gastrointestinal bleeding related to CMV ulceration in small bowel, is rare.[12] Our patient was not receiving steroids or any immunosuppressive drugs, but he was debilitated and critically ill. The use of serology and parallel PCR analysis to confirm the diagnosis of cytomegalovirus infection, should enable early antiviral therapy to be instituted, resulting in marked clinical improvement. Histology, demonstrating the classical appearance of ′′owl′s eye′′inclusion bodies, is the gold standard test for cytomegalovirus diagnosis. However, recent studies using PCR have indicated that it may be a sensitive and specific assay for diagnosis.[13],[14] If CMV infection is confirmed, Ganciclovir therapy should be initiated without delay. Immediate surgical resection and prompt antiviral therapy, lead to successful treatment. Our patient had improved and bleeding was stopped, when Gancyclovir was initiated after resection of the ileum. Mortality rates for patients with cytomegalovirus enterocolitis have been quoted as high as 71%.[15] In conclusion, physicians must be aware of CMV enterocolitis and Immediate surgical resection and prompt antiviral therapy as the main treatment. Therefore, CMV enterocolitis should be considered in the differential diagnosis of lower gastrointestinal bleeding, in any debilitated and/or mechanically ventilated patient. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06007f3.jpg] [cm06007f1.jpg] [cm06007f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}