 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
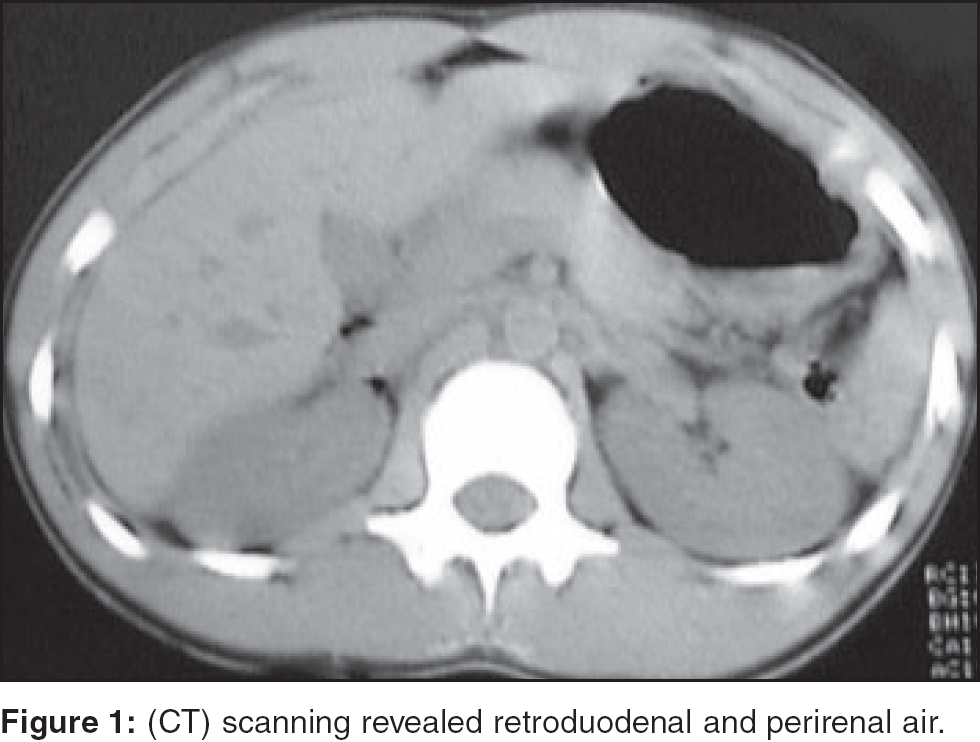
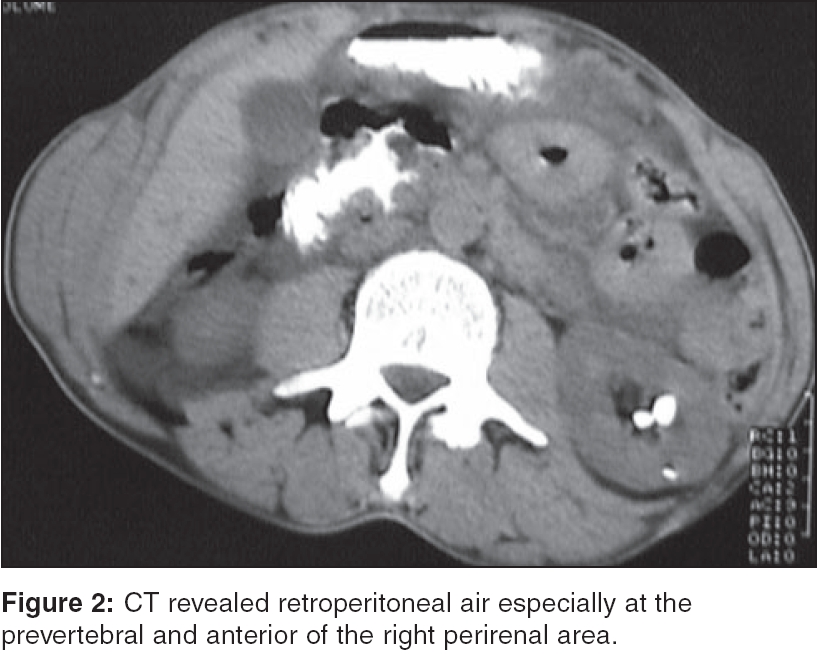
Indian Journal of Critical Care Medicine, Vol. 10, No. 1, January-March, 2006, pp. 44-46 Case Report Isolated duodenal rupture due to blunt abdominal trauma Celik Atilla, Altinli Ediz, Onur Ender, Sumer Aziz, Koksal Neset From:Haydarpasa Numune Training and Research Hospital, Department of General Surgery, 2nd General Surgery Clinic, Istanbul, Turkey Correspondence Address:Dr. Ediz Altinli, Naci Kasim Cad. Baran Sitesi C 1 Blok D: 10, 34590 Bahcelievler, Istanbul, Turkey. E-mail: dredizaltinli@yahoo.co.uk Code Number: cm06008 Abstract Duodenal rupture following blunt abdominal trauma is rare and it usually seen with other abdominal organ injuries. It represents approximately 2% to 20% of patients with blunt abdominal injury and often occurs after blows to the upper abdomen, or abdominal compression from high-riding seat belts. Two cases of blunt duodenal rupture successfully treated surgically, are presented with their preoperative diagnosis and final out comes.Keywords: Blunt duodenal injury, duodenal trauma, blunt abdominal trauma. Duodenal rupture following blunt abdominal trauma is rare and it is usually seen with other abdominal organ injuries. It represents approximately 2% to 20% of patients with blunt abdominal injury and often occurs after blows to the upper abdomen, or abdominal compression from high-riding seat belts.[1] Forty percent of patients with duodenal injuries have other concomitant surgically important intra-abdominal injuries, such as hepatic (38%), or pancreatic (28%) injuries.[2] Case 1 Physical examination on admission showed slightly tender abdomen and two epigastric dermabrasion, with 2x2 cm in dimensions. Blood pressure, pulse and temperature, were all normal. Blood analysis showed a hemoglobin 12.6 g/100 ml, a white blood cell count of 23 x 10 9/L and amylase level of 126 mg/100 ml. Plain abdominal and chest radiographs were normal and did not show any evidence of pneumoperitoneum and abdominal ultrasonography were unremarkable. The patient was admitted for observation. After observation for 2 hours, the patient had prominent peritoneal signs and a hollow viscus injury was suspected. IV contrast enhanced computed tomography (CT) scanning without oral contrast material was performed, which revealed retroduodenal and perirenal air [Figure - 1]. The patient underwent urgent laparotomy for duodenal rupture, with initial diagnosis. The injury severity degree evaluated to grade III, according to duodenal injury scale as described by Moore et al .[3] Primary repair plus drainage was the choice of treatment. Recovery after the operation was uneventful and the patient were discharged from hospital on the 6th postoperative day. Case 2 First observations including blood pressure, pulse and temperature, were all normal. Abdominal examination was not special, except for epigastric echimosis with 2 cm in diameter, due to hitting of the handlebar. Blood analysis showed a hemoglobin level at 13 g/100 ml and a white blood cell count of 13x10 9/L. Serum amylase was 147 mg/100 ml. Abdominal plain roentgenograms and abdominal ultrasonography were normal. Because of persistent pain and suspicion of abdominal injury, IV contrast enhanced abdominal CT scanning without oral contrast material, was performed. The CT demonstrated retroperitoneal air, especially in the prevertebral area and anterior of the iliopsoas muscle [Figure - 2]. The patient underwent urgent laparotomy with diagnosis of duodenal rupture, like the first patient. The injury severity degree evaluated to grade III, according to the duodenal injury scale as described by Moore et al .[3] The rupture site was the anterior and posterior site of the 3rd part of the duodenum. Primary repair in a shape of Henike-Mickulich type plus drainage was the choice of treatment.Recovery after the operation was uneventful and the patient was discharged from hospital on the 12th postoperative day. Discussion Isolated blunt injury of the duodenum is both less common and more difficult to diagnose than penetrating injuries and it may also occur with pancreatic injury.[4] Despite progression of the imaging techniques, the diagnosis still remains critical and may be delayed in particular, when there is perforation of the retroperitoneal part of the duodenum.[5] It usually occurs from crushing of the duodenum between the spine and steering wheel, handlebar, or some other force applied to the anterior aspect of the abdomen.[6] While the history and clinical findings of steering wheel, handlebar and seat belt marks on the anterior abdominal wall may make the clinician suspect a duodenal injury, the physical examination may not be helpful in trying to identify early duodenal injuries.[7] In the vast majority of retroperitoneal perforations, there is at first only mild upper abdominal tenderness with a progressive rise in temperature, tachycardia and occasional vomitting. After several hours, the duodenal contents extravasate into the peritoneal cavity, with the development of peritonitis. Initial clinical changes in isolated duodenal injury may be extremely subtle before the severe, life-threatening, peritonitis develops.[4] Laboratory findings that contain WBC, hemoglobin, or amylase level, are not specific. Although serial determination of serum amylase is better than a single, isolated assay on admission, sensitivity is still low and serial determination involves unnecessary delay in the treatment. Plain radiographs of the abdomen are useful when gas bubbles are present in the retroperitoneum. They may also show free intra-peritoneal gas and, although rarely seen, gas in the biliary tree has also been described.[8] Abdominal ultarsonograpy is faster and less invasive than diagnostic peritoneal lavage and can occasionally reveal injuries in the retroperitoneum. Abdominal sonography that reveals free fluid, suggests hemoperitoneum, or bowel injury requires abdominal CT or emergency laparotomy.[9] Diagnostic peritoneal lavage (DPL) has been found to have a low diagnostic sensitivity for duodenal rupture, because of the retroperitoneal location of the duodenum. Furthermore, because the incidence of associated intra abdominal injuries is high in cases of duodenal trauma and liver or splenic injury is often the source of a positive DPL, so the specificity of DPL for duodenal rupture remains still low.[10] CT has been added to the diagnostic algorithm for subtle duodenal injury. It is very sensitive to the presence of small amounts of retroperitoneal air, blood, or contrast agent extravasated from the injured duodenum, especially in children.[4] Early diagnosis of duodenal rupture is essential, the delay of which is associated with increased morbidity and mortality. The diagnosis of this injury remains problematic, because the signs and the symptoms of retroperitoneal viscus are notoriously subtle. Diagnostic delaying of the patients with duodenal rupture may cause catastrophic events. A delay in diagnosis for longer than 24 hours results in a thickened, friable and inflamed bowel wall. Primary repair alone is unlikely to be successful, as it may lead to duodenal dehiscence, a lateral duodenal fistula and other lethal complications.[7] The degree of duodenal injury, diagnosis time and surgeon preference,often determines the type of technique using repair. Although most duodenal injuries can be managed successfully by simple repair, the available techniques contain simple reparation, tube duodenostomy and pyloric exclusion, with or without gastrojejunostomy.[11] In conclusion, the diagnosis of duodenal injuries remains difficult, with high incidence of suspicions, especially if it is isolated. A preoperative diagnosis of isolated duodenal rupture can be very difficult to make and there is no single method of duodenal repair that completely eliminates the possibility of dehiscence of the duodenal suture line.[4] Contrast enhanced abdominal CT may be helpful for early diagnosis and to prevent complications due to delayed diagnosis of duodenal rupture. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06008f2.jpg] [cm06008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}