 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
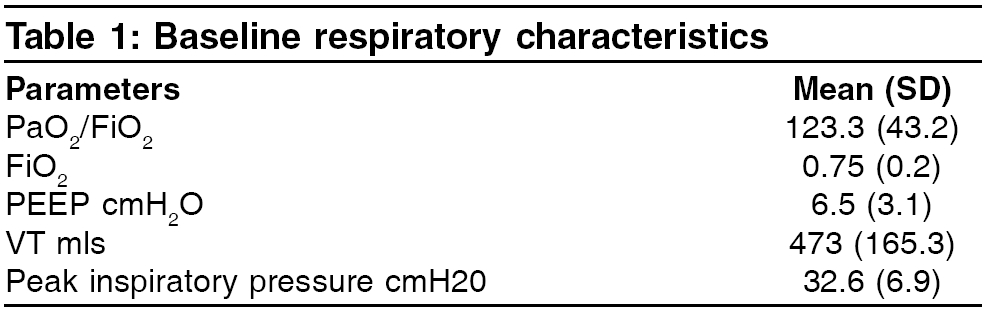
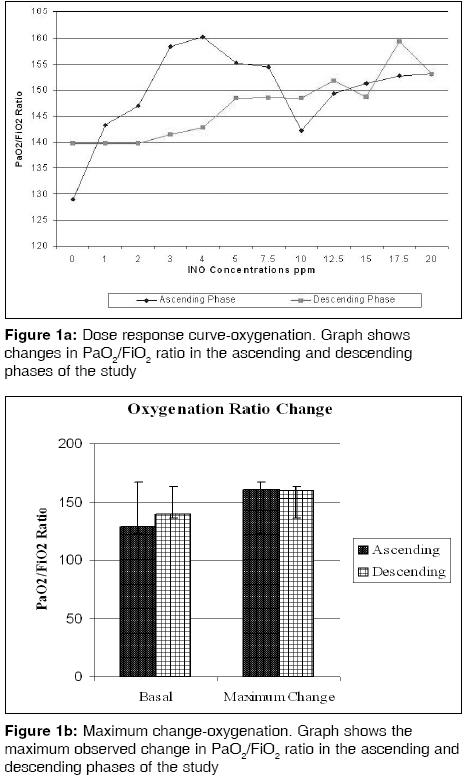
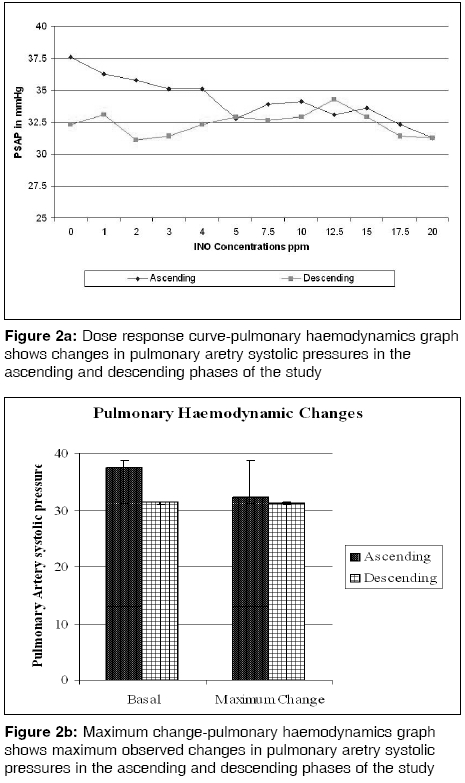
Indian Journal of Critical Care Medicine, Vol. 10, No. 2, April-June, 2006, pp. 75-79 Research Article Acute effects of nitric oxide inhalation in ARDS: A dose finding study at steady state kinetics Hari MShankar, Trikha A, Madan R, Kaul HL Intensive Care Unit, Guy's and St Thomas Hospitals, London Code Number: cm06012 Abstract Background: Inhaled Nitric oxide (INO) decreases pulmonary artery pressures and improves oxygenation in patients with ARDS.Aim: To evaluate the dose response to 1-20 parts per million (ppm) INO in ARDS, by noting changes in oxygenation, pulmonary artery systolic pressures (PASP) and to determine optimum dose. Methodology and Design: Prospective study. Setting: 10 bed general intensive care unit. Patients: 13 consecutive patients with ARDS. Interventions: INO was given between 1-20 ppm with 15 minutes at each concentration via an insufflator from a high pressure source, to the inspiratory limb of the ventilator. Study had ascending and descending phase. Results and Conclusions: The optimum dose of INO to improve oxygenation was between 3 and 10 ppm. PaO2 improvement was independent of pulmonary haemodynamic changes. The pulmonary haemodynamic changes needed higher INO initially. Once stabilized, INO could be brought down to concentrations at which maximum improvement in PaO2 occurred. The 'responders' had lesser duration of pre INO ventilation and lower PaO2/FiO2. Keywords: ARDS, nitric oxide, acute effects Adult respiratory distress syndrome (ARDS) is characterized by acute respiratory distress, refractory hypoxaemia and pulmonary hypertension and remains a challenging organ failure for the intensivist. Accumulating data from basic science and clinical studies have dramatically changed the understanding of the ways in which mechanical ventilation itself may interact with the acutely injured lung to further impair pulmonary function. This understanding has prompted a lung protective ventilation strategy, which in a recent clinical outcome study, was shown to improved pulmonary function and survival.[1] As an intervention- inhaled nitric oxide [INO] therapy has not been shown to improve the outcome and the optimum dose of INO in ARDS is not defined. Our hypothesis was INO is a selective pulmonary vasodilator which redistributes the pulmonary blood flow to the ventilated parts of the lung. This reduces pulmonary vascular resistance (PVR) and improves PaO 2 by better ventilation perfusion matching. 0 The aim of our study were to evaluate dose - response effect of INO in ARDS by noting changes in oxygenation (PaO 2 /FiO 2 ratio) and pulmonary artery systolic pressure (PASP), in response to 1-20 parts per million [ppm] concentrations, to determine the optimum dose and the predictors of response to INO. Methodology Lung protective ventilatory strategy [tidal volume of 4-8 ml / kg and the mean airway pressures less than 30 cmH2O] was used and the ventilatory parameters remained constant during the course of the study. The FiO 2 was adjusted between 0.5 and 1.0 to maintain a PaO 2 > 60 mmHg. Administration of inhaled Nitric Oxide (INO) All the study patients had a radial artery catheter and a PA-catheter in situ, during the course of the study. Monitoring of hemodynamic variables was using Mennen Medical Inc . Monitor Horizon 2000. Hemodynamic and oxygenation variables were measured at end expiration, every 15 minutes before changing the INO concentration. For the pulmonary mechanics ventilator, display was noted. For blood gas analysis, AVL 998 monitor was used. One point calibration was done every 30 minutes and two point calibrations were done every 8 hours. The ′responders/response to treatment′ were defined by the following criteria: PaO 2 /FiO 2 ratio increase was more than 15% of base line and/or PSAP fall was more than 15% of base line value in three consecutive concentrations. Analysis Results The mean (SD) age of our patients was 50 (15.3) yrs, with a mean (SD) Apache III score of 53.7 (13.3). The mean (SD) MODS and Murray score were 7.2 (1.4) and 2.8 (0.5), respectively. On analysis of risk factors for ARDS present at admission, 12 patients had pneumonia which was statistically significant ( P =0.002), 3 patients had laparotomy evidence of peritonitis which was statistically significant ( P =0.04) and one patient each had eclampsia, pancreatitis and polytrauma with fat embolism. The baseline respiratory characteristics of the patient are presented in [Table - 1]. The baseline mean PaO 2 /FiO 2 ratio was 129.1 (44.2). The maximum improvement of 160.3 (80) was observed at 4 ppm, which was 24% above baseline. The mean values at 3 ppm to 7.5 ppm and 15 ppm to 20 ppm, showed an increase of greater than 15% above baseline values, by our definition ′Response to treatment/Responder status′. However, there was no statistically significant improvement in PaO 2 /FiO 2 ratio at any INO concentrations [Figure - 1]a and b. Baseline mean (SD) PASP was 37.5 (12.1) mmHg. Statistically significant reduction in PASP was observed at INO concentrations of 20 ppm in the ′ascending phase′ of the study and at 2 ppm and 3 ppm in the ′descending phase′of the study. ( P =0.013) [Figure - 2]a and b. The hemodynamic parameters i.e., the heart rate, blood pressure, central venous pressure, pulmonary artery wedge pressure and peak inspiratory pressure showed no statistically significant improvement. The baseline mean (SD) cardiac output (CO) was 7.3 (0.7) L/min, which increased to 7.7 (0.06) L/min at 20 ppmI NO. There were 8 responders in the study- 4 by increase in PaO 2 /FiO 2 ratio and 4 by decrease in PSAP without corresponding increase in PaO 2 /FiO 2 ratio. Seven of the eight responders had pneumonia. Responders had significantly lower PaO 2 /FiO 2 ratio (96.7 ± 26.6 vs 135.2 ± 45 mmHg) ( P =0.032), were ventilated for significantly shorter period before INO treatment than non responders (103.5 ± 82.43 vs 394.89 ± 479.87 hrs) ( P =0.037) and had a higher hematocrit (28.2 ± 5.94 vs 22.3 ± 2.06). 8 out of 13 patients enrolled into the study, did not survive. Discussion The ventilatory strategy used in our study is similar to the treatment group data provided by the acute respiratory distress syndrome network.[1],[2] The following studies formed the basis for the INO concentrations in our study. Bigatellow et al[4] and Rossaint et al[5] have showed that INO of 5-20 ppm are sufficient to elicit a significant increase in PaO 2 and that toxicity is immeasurable at these concentrations. Gerlach et al[6],[7] showed that INO of 10 ppb to 100 ppb is required to improve oxygenation and INO of 1-10 ppm, to improve pulmonary hypertension in ARDS. The variability in response to INO prompted us to study the same concentrations in the reverse order to note consistency in response. The repeat dose testing to see the consistency in response, was also done by Lundin et al[8] and Treggiary Venzi et al .[9] The consistency in response (± 10% of corresponding values) to INO was not seen in our study, which corresponded with the results of these authors. Equilibration time of inhaled and alveolar concentrations has been reported as 10 to 20 minutes. This prompted us to use INO for 15 minutes at each concentration. The observed change in the PaO- 2 /FiO 2 ratio in our study was a non dose dependent, non linear increase. The non dose-dependent change in oxygenation parameters in our study was similar to Johannigam et al ,[10] but the data from Bigatellow et al[4] showed a dose dependent increase in PaO- 2 /FiO 2. Treggiari-Venzi[9] et al and Lowson et al[11] found a maximum increase in PaO- 2 /FiO 2 ratio at 10 ppm INO, with a range of 1-20 ppm INO. However, in our study, the INO concentration at which maximum response observed was 3-10 ppm, which we attribute to optimal lung recruitment. The observed change in PASP was non dose dependent, non linear and unrelated to the change in oxygenation. From our data, it was observed that the reduction in PAP is related to the duration of INO treatment, as the PASP was lower in the descending phase of study, than the ascending phase for the same INO concentration. Reviewing the literature, we have found contradictory reports. Rossetti et al[12] described a significant fall in pulmonary artery pressures (PAP) at 15 and 25 ppm INO ( P =0.001). Lowson et al[11] showed non dose dependent fall in mean PAP ( P < 0.022) at 10 ppm INO. Iotti et al[13] described a dose dependent fall in mean PAP from 0.5-5 ppm, while Puybasset et al[14] described a dose dependent fall in mean PAP with INO of 0.1-2 ppm. However, Luyt et al[15] and Lundin et al[16] showed that INO had no effect on PAP. In our study, we had 21 concentrations of INO. Due to extreme variability in response to INO, we defined responders as those who had either persistent increase in PaO 2 /FiO 2 of 15% or more, or decrease in PASP of 15%. Of the 13 patients studied, 8 patients were responders by the above criteria i.e., 62% which corresponds with the data by Manketelow et al .[17] A marked variation was observed during our study in the hemodynamic and oxygenation effects of INO. The reasons for the variability include preexisting pulmonary disease, infusions of vasoactive drugs, ventilation associated lung injury and pulmonary vascular remodeling in ARDS. The "Responders" had maximum increase in PaO 2 /FiO 2 at concentrations between 3 and 10 ppm. Once maximum increase was reached, further increase in INO did not increase PaO 2 or reduce PASP significantly. Patients who were "Responders" by PASP criteria, were non-responders by PaO 2 /FiO 2 criteria, thereby showing that changes in PAP were independent of PaO 2 changes, which was similar to the data from Lundin et al .[8] From our study, it was clear that the "Responders" had significantly lower PaO 2 /FiO 2 ratio similar to data from Treggiari-venzi[9] and Dupont et al .[18] the duration of ventilation before INO treatment as a marker of response to INO was lesser, which has not been shown before and that we feel probably reserves the place for INO treatment in early severe ARDS. From the concentrations, we studied that the optimum dose to improve oxygenation was between 3 ppm and 10 ppm. Neither oxygenation nor the pulmonary hypertension in ARDS showed dose dependent change. Concentrations of inhaled NO above 10 ppm do not produce any further benefit. We could not identify a uniform predictor of response to INO treatment, however low baseline PaO 2 /FiO 2 ratio and shorter duration of ventilation prior to INO treatment appears to be best predictive markers of beneficial response to INO. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06012t1.jpg] [cm06012f1.jpg] [cm06012f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}