 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
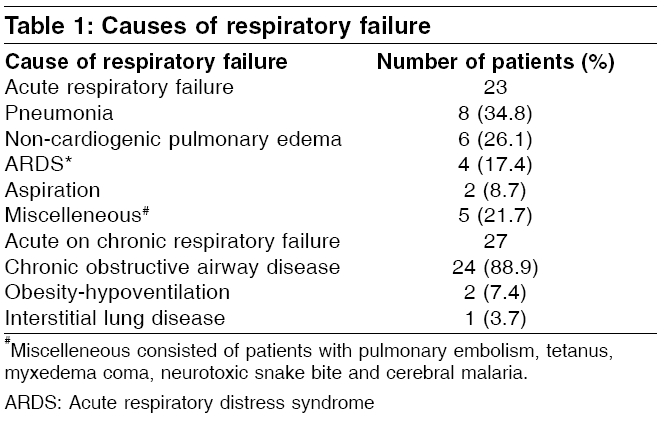
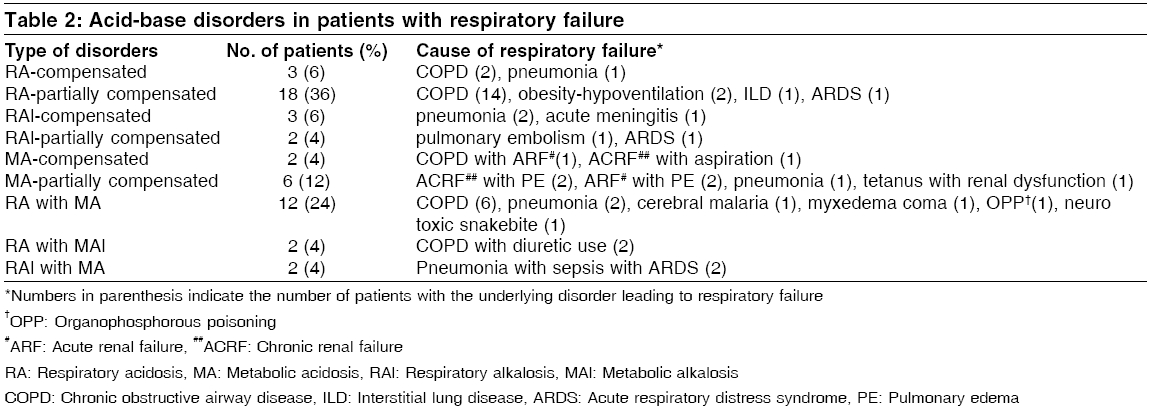
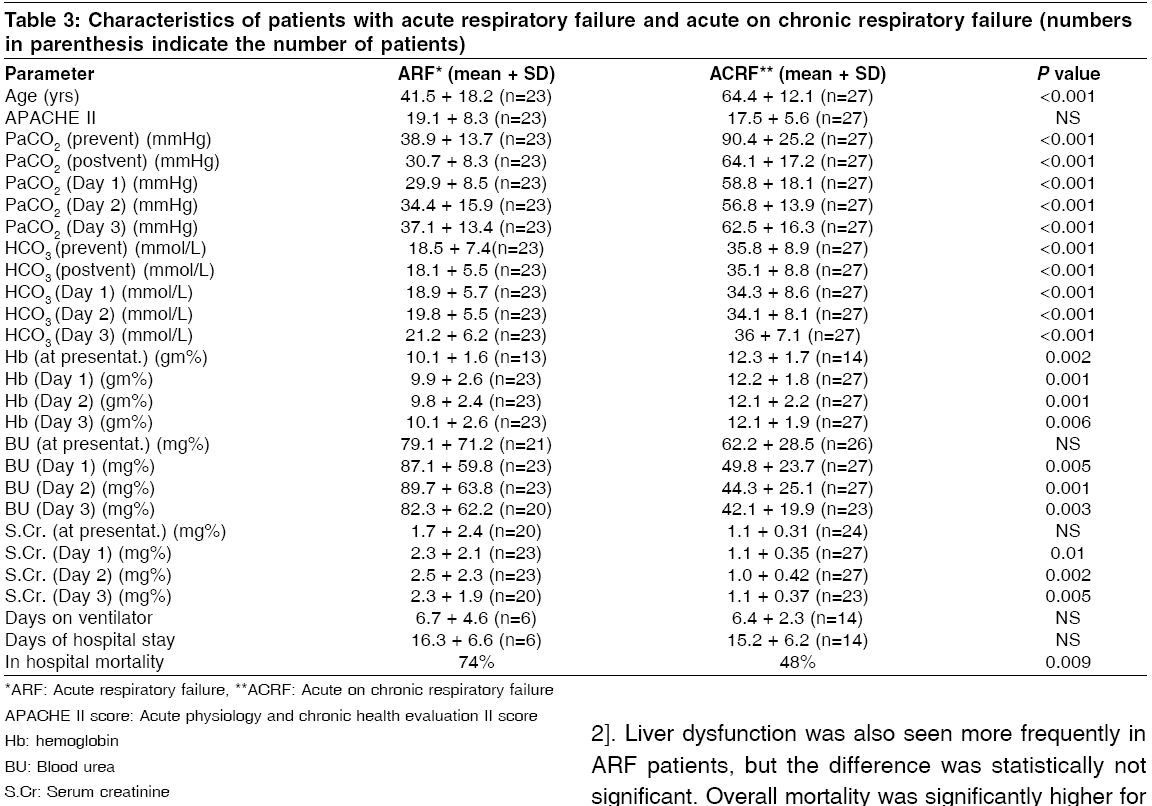
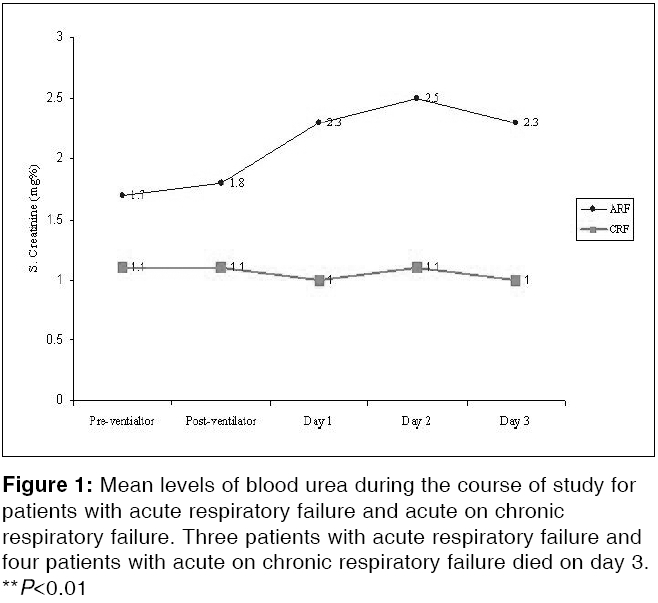
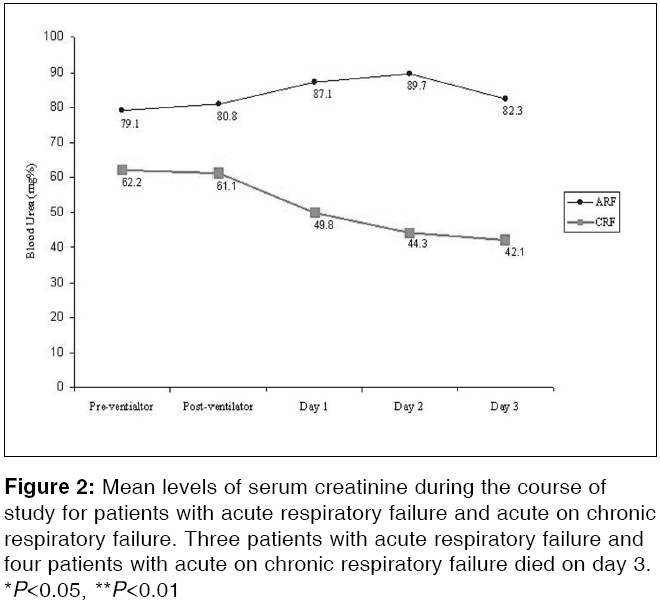
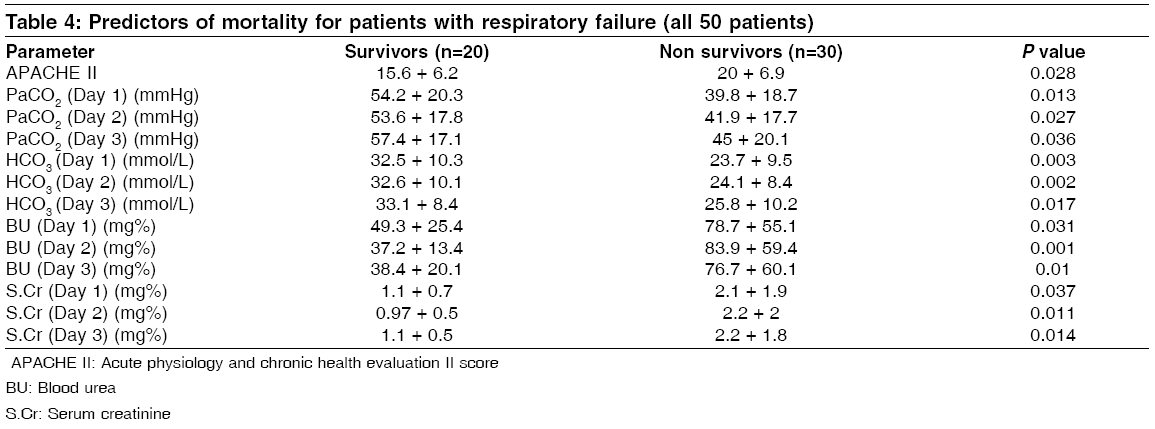
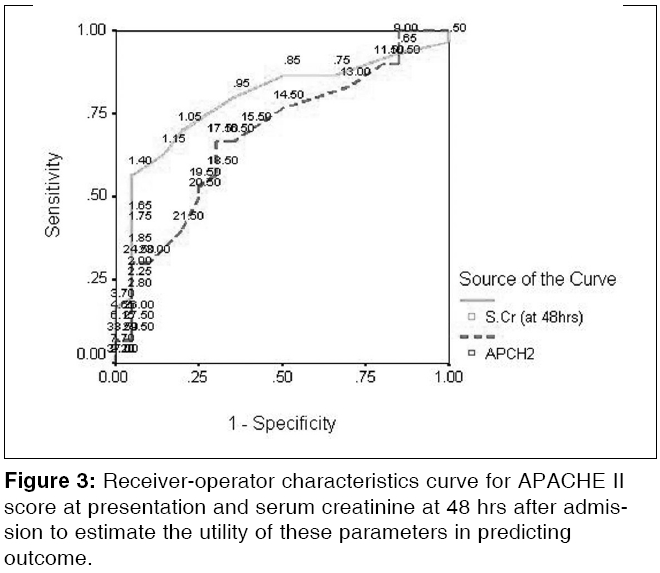
Indian Journal of Critical Care Medicine, Vol. 10, No. 2, April-June, 2006, pp. 80-87 Research Article A comparative study of characteristics and outcome of patients with acute respiratory failure and acute on chronic respiratory failure requiring mechanical ventilation Banga Amit, Khilnani GC Department of Medicine, All India Institute of Medical Sciences, New Delhi Code Number: cm06013 Abstract Background and Aims: Patients with respiratory failure requiring assisted ventilation form a large diagnostic group among critically ill patients. The outcome of patients with acute respiratory failure (ARF) as compared to those with acute on chronic respiratory failure (ACRF), may be different. The present study was designed to evaluate the clinical and acid base profile at presentation, hospital course and outcome in patients with ARF and ACRF requiring ventilatory support and to define factors that influence the outcome of these two groups of patients.Materials and Methods : Fifty patients with respiratory failure {ACRF (n=27) and ARF (n=23)} who required invasive mechanical ventilation, were included in a prospective fashion. Clinical data including APACHE II score, blood gas analysis and renal and liver functions were recorded at presentation and for the next three days. Survival to hospital discharge was the primary outcome measure. Various parameters were compared between ARF and ACRF, as well as between survivors and non-survivors to define predictors of mortality. Results: Patients with ARF were significantly younger (41.5 versus 64.4 years, P <0.001), but all other baseline parameters including APACHE II score were similar for the two groups. During the hospital course, mean blood urea and serum creatinine became significantly higher in patients with ARF ( P <0.001). Mortality was significantly higher for patients with ARF (74% versus 48%, P =0.009). For the whole study group, APACHE II score and serum creatinine, 48 hrs after admission, were independent predictors of mortality. Conclusions: Although patients with ARF and ACRF may appear equally ill at presentation, mortality is higher for patients with ARF. A higher incidence of complications such as development of non-pulmonary organ failure during the hospital course in patients with ARF, seems to be responsible for this increased mortality. Keywords: APACHE II score, ICU, mortality, non-pulmonary organ dysfunction, prognostic markers Respiratory failure is defined as the acute inability of the lungs to maintain adequate oxygenation of the blood and systemic organs, with or without impairment of carbon dioxide elimination. Respiratory failure forms a large diagnostic group among critically ill patients and many of these patients require mechanical ventilation (MV). In a recent multi-center study,[1] out of almost 5200 adult patients who required MV, indication for institution of MV was respiratory failure in almost 80% of the patients. Patients with respiratory failure constitute a heterogeneous group of patients who have variable clinical presentation, hospital course and outcome. Although the mortality of these patients may be high,[2],[3] many patients are suffering from potentially reversible ailments, such as severe community acquired pneumonia (CAP), recovery from which leads to minimal long-term disability. It is obvious that such patients should be identified early in their course of illness and offered the best of intensive care facilities available. Patients with respiratory failure can be broadly classified into two subgroups: acute respiratory failure (ARF) and acute on chronic respiratory failure (ACRF). While ARF can be defined as presence of features of respiratory failure in a patient without any underlying pulmonary pathology, ACRF signifies decompensation of an underlying chronic lung disease such as chronic obstructive pulmonary disease (COPD). Patients from both these groups of respiratory failure may appear to be suitable candidates for admission to an intensive care unit (ICU) because of similar clinical and laboratory characteristics, as well as similar critical illness score derived from various widely used prognostic scoring systems. But many of these patients appear equally ill at presentation, because of the presence of certain confounding factors. A typical example of such a factor would be the presence of similar level of hypercapnia in two patients; one with ACRF such as COPD and another with ARF such as CAP. Although the level of hypercapnia may be similar, the therapeutic implications for these two patients are totally different. Any prognostic scoring system that includes PaCO 2 levels in scoring the patients, would score similarly for both the patients. Hence, decision regarding provision of intensive care solely on the basis of the scoring system, may not be free from pitfalls. Many investigators, while studying a heterogeneous group of patients comprising of both patients with ARF and ACRF, have observed that patients with ARF have much worse outcome as compared to those with ACRF.[4] In spite of this, there is a lack of studies dedicated to direct comparison between these two types of respiratory failure. Also, factors that lead to comparatively poor outcome in patients with ARF have not been fully elucidated. This study was designed to compare the clinical profile and acid-base disorders at presentation, hospital course and outcome of patients with ARF and those with ACRF. We also tried to define factors that are associated with poor outcome in patients with respiratory failure. Materials and Methods Study Design: Prospective observational study Fifty consecutive patients with respiratory failure admitted to the ICU, were included over an eight month period (July 2003 - February 2004). A total of 154 patients were admitted to the ICU during this period. To avoid heterogeneity, only direct admits to the ICU and those who required MV for at least 48 hrs, were included in the present study. Informed consent was procured from the nearest relative of each study subject. These patients were classified into ARF (n=23, 46%) and ACRF (n=27, 54%) on the basis of arterial blood gas analysis (ABGA) and clinical profile. All patients were evaluated in detail and clinical diagnosis based on pertinent history, clinical examination and investigations was made. The clinical data including pulse rate (PR), respiratory rate (RR), mean blood pressure (MBP), Glasgow coma scale (GCS) (before intubation) and acute physiology and chronic health evaluation (APACHE) II score,[5] was recorded. For all patients, ABGA along with serum electrolytes were done before (pre-ventilator) and after (within ½ to 2 hrs) initiation of MV (post-ventilator). Various isolated and mixed acid-base disorders were classified on the basis of pre-ventilator ABG using the approach suggested by Harrington and coworkers.[6] Daily ABG, renal functions, liver functions and hemogram were done for the next three days. In addition, daily urine output and drugs prescribed were recorded. ABGA was done using approximately 0.5 ml of arterial blood collected in heparinized glass syringes from the radial or brachial artery. Analysis was done immediately after collection using the AVL-995S auto-analyzer and pH, PaO 2 , PaCO 2 , as well as HCO 3 values were recorded. None of the management decisions including drug therapy, decision regarding institution of invasive MV, or weaning protocols were modified for the purpose of the study and were solely taken by the ICU management team. Patients were followed up after the completion of three days and clinical outcome in the form of days on ventilator; days of hospital stay and survival to hospital discharge, were recorded. Various parameters were compared between patients with ARF and ACRF to study the differential profile at presentation, hospital course and outcome in these two groups of patients. Predictors of mortality were defined by comparing the parameters between survivors and non-survivors. Statistical analysis Data collected was entered into a computer and was analyzed using the statistical software ′ SPSS 10.0 .′ Data was described as mean with standard deviation (SD). The study group was split into two groups on the basis of the type of respiratory failure, namely ARF and ACRF. Various clinical and laboratory parameters and outcome measures were compared between the two groups using Mann Whitney U test for continuous variables and Fisher′s exact test for ordinal variables. Parameters were also compared between survivors and non- survivors using similar tests, to define predictors of mortality. Parameters significant on univariate analysis were evaluated by multivariate logistic regression analysis to define independent predictors of mortality. Receiver-operator characteristic (ROC) curve was plotted using 1-specificity on the x-axis and sensitivity on the y-axis for each value of APACHE II score and serum creatinine done at 48 hours after admission (independent predictors of mortality) and the area under the curve was estimated. Best cut-off for both the variables was taken as the value at the point where curve sharply angulated. Sensitivity and specificity was calculated for both the variables using the derived cut-off. Statistical significance was considered at P < 0.05 (only two-tailed). Results Mean age of the study group was 53.9 + 18.9 yrs (range 14-85 yrs), with 70% of the patients (n=35) being males. Seventeen patients (34%) had cyanosis at the time of presentation. Mean PR, RR and MBP were 99.7 + 19.2 per minute (range 52-150/min), 33.8 + 6.6 per minute (range 12-50/min) and 95.7 + 23.6 mmHg (range 20-133.3 mmHg), respectively. Mean GCS was 10.4 + 3.1 (range 3-15), whereas mean APACHE II score was 18.3 + 6.9 (range 6-36). Sepsis was the commonest cause of ARF (8 patients, 34.8%). A large majority of the patients with ACRF had COPD (24 patients, 88.9%). Various causes of respiratory failure in our study group are mentioned in [Table - 1]. Mean length of stay on ventilator was 6.5 + 3 days (range 3-15), whereas mean duration of hospital stay was 15.5 + 6 days (range 6-28). Overall mortality was 60% (n=30). Acid base disorders Most common acid base disorder was respiratory acidosis (RA), with variable degrees of compensation (21 patients, 42%), followed by combined RA and metabolic acidosis (MA) (12 patients, 24%) and pure MA (8 patients, 16%). Other acid base disorders seen with underlying disorder resulting in respiratory failure are listed in [Table - 2]. Among the patients who had acidosis, mortality was significantly higher for patients with pure MA than those with pure RA (75 versus 52%, P =0.019). Among the 27 patients with ACRF, 19 (70.4%) had pure RA, whereas 8 patients had mixed disorders (6 had associated MA and 2 had metabolic alkalosis). In this subgroup, mortality was higher for patients who developed MA with RA, as compared to those with pure RA (83.3 versus 42%, P =0.005). In patients with ARF, presence of RA with MA, or in other words, development of hypercapnic respiratory failure in presence of MA was associated with higher mortality than with pure MA, although the difference was statistically not significant (83 versus 50%). Comparative profile of the two groups Mean age of patients with ARF was 41.5 yrs (range 14-80 yrs), whereas that for patients with ACRF was 64.5 yrs (range 40-85 yrs, P < 0.001). There was no statistically significant difference in other clinical parameters such as PR, RR, MBP and GCS, between the two groups. Mean APACHE II score (estimated at presentation) also was similar for the two groups {ARF: 19.1 + 8.3 (range 7-36) and ACRF: 17.5 + 5.6 (range 6-25), P >0.4}. Although both mean PaCO2 and HCO 3 were significantly lower in patients with ARF in pre and post ventilator ABGA, as well as during all the three days of study, mean pH for both the groups remained similar throughout the study period [Table - 3]. Also none of the other baseline laboratory parameters including renal and liver functions at presentation were different for the two groups. But during hospital course, mean urea and creatinine levels tended to rise in patients with ARF and became significantly higher than mean urea and creatinine levels for patients with ACRF [Figure - 1][Figure - 2]. Liver dysfunction was also seen more frequently in ARF patients, but the difference was statistically not significant. Overall mortality was significantly higher for patients with ARF as compared to patients with ACRF (74 and 48%, P =0.009). There was no significant difference in days on ventilator,as well as days of hospital stay between the two groups. Predictors of mortality The whole study cohort was analyzed together to define predictors of mortality that could be applicable to patients with respiratory failure, secondary to various causes. Deranged renal functions were found to be the strongest predictor of mortality [Table - 4]. Non-survivors had higher APACHE II ( P =0.028) score at presentation. Also, low PaCO 2 and HCO 3 levels were associated with poor outcome. On subgroup analysis for ACRF group, mean APACHE II score was 21.1 + 4.1 for non-survivors, whereas it was 14.1 + 4.6 for survivors ( P < 0.001). For patients with ARF, mean APACHE II for both non-survivors and survivors was similar (19.1 + 8.5 and 19.2 + 8.4, P >0.9). This suggests that APACHE II score estimated at presentation is a poor predictor of mortality in patients with ARF, but is useful for predicting outcome in patients with ACRF. Renal dysfunction was associated with increased mortality for both ARF and ACRF. These parameters were evaluated using multivariate logistic regression analysis to define independent predictors of mortality. APACHE II score at presentation ( P =0.02, β =1.2) and serum creatinine at 48 hrs after admission ( P =0.024, β =23.1) were found to be independent predictors of mortality. ROC curve for APACHE II score and serum creatinine showed AUC value of 0.69 and 0.79, respectively [Figure - 3]. Best cut-off for APACHE II score was found to be 17.5 and sensitivity and specificity for predicting outcome at this level was 66 and 70%, respectively. Best cut-off for serum creatinine was 1.05 mg%, which resulted in a sensitivity of 70% and specificity of 80%, for predicting outcome. Discussion Cost of critical care remains high and with the limited availability of resources in developing countries, judicious usage of such resources is a must. It is common for critical care physicians to be in a dilemma while deciding whom to offer the limited intensive care facilities at their disposal. We studied patients with two different types of respiratory failure, commonly admitted to ICU. We tried to define which group is most likely to derive the maximum benefit from provision of ICU facilities. It was demonstrated that the outcome of these patients as judged by in hospital mortality, is far worse for patients with ARF as compared to those with ACRF. Although the mortality rates for both groups of patients were fairly high, this may be ascribed to the significant selection bias that occurred due to inclusion of only those patients who required ventilatory support. The findings from the present study substantiates those from the earlier studies,[4] where it has been consistently reported that patients with ARF are the sicker group of patients and are more likely to die as compared to those with ACRF. Both the groups had similar profile at presentation. No statistically significant difference was found in mean pH, renal functions, as well as liver functions at baseline. Also mean APACHE II score estimated at presentation was similar for the two groups. In spite of this, mortality in patients with ARF was significantly higher. This suggests that baseline characteristics of these patients are poor predictors of outcome. The single most important factor responsible for the failure of baseline parameters including APACHE II score to predict outcome, appears to be the fact that patients with ARF have a strong tendency to develop complications during the hospital stay. Mean levels of blood urea and serum creatinine for patients with ARF rose significantly during the hospital stay, as compared to patients with ACRF [Figure - 1][Figure - 2]. Even liver functions deteriorated during hospital stay for patients with ARF, although statistical significance was not achieved. It can be deduced that it is the hospital course that holds the key to outcome of these patients, rather than the baseline characteristics. Development of organ dysfunction during the hospital stay in patients with respiratory failure is a strong predictor of mortality and patients with ARF seem to be at a higher risk of developing these complications. This fact may be explained to an extent on the basis of pathogenesis of these two types of respiratory failure. In ARF, patients with otherwise healthy lungs are unable to maintain adequate oxygenation of the blood. Respiratory failure in these patients is result of an acute, but catastrophic insult. The seriousness of this insult can be estimated by the fact that it is significant enough to result in respiratory failure in healthy subjects, without any underlying illness. In contrast, patients with ACRF remain in a state of altered physiology due to chronic hypoxemia or hypercarbia and the most trivial of insults disturbs the precarious balance leading to decompensation in these patients. Although patients with ARF and ACRF may have similar characteristics at presentation, the severity of insult incurred by patients with ACRF is likely to be milder than that of patients with ARF. Another important issue has been the reluctance of clinicians to institute mechanical ventilation in patients of acute on chronic respiratory failure, for fear of prolonged ICU stay and increased cost of treatment. Many authors have raised the issue of cost effectiveness of providing assisted ventilation to a patient with advanced COPD, as weaning may be difficult and survival to hospital discharge low.[7],[8] In fact, Sluiter et al[9] recommended a conservative approach in the form of early therapy, preferably at home, with anti-microbial agents, bronchodilators and corticosteroids for patients with exacerbation of COPD. They went on to suggest that patients who fail adequate conservative treatment might not always be ventilated. In contrast, in our study, the days on ventilator as well as days of hospital stay for both groups of respiratory failure were similar [Table - 3] Similar findings have been reported by other recent studies as well.[1],[10] In addition, investigators studying exacerbation of COPD requiring mechanical ventilation have reported acceptable lengths of stay on ventilator for these patients.[11],[12] Moran[11] reported a mean duration of stay on ventilator of 6.2 days, whereas Kramer[12] found the mean duration to be 7 days for his study cohort. Significant advances made in the field of intensive care with wider availability of better monitoring equipment and superior modes of ventilation, seem to be responsible for this change. There have been few studies, which have looked at the various acid base disorders seen in patients of respiratory failure. Nor has the impact of these acid base disorders on outcome of these patients been studied. Our study classified the patients in to various acid base disorders on the basis of ABGA done before patients were put on ventilator. Mortality in patients with pure RA was significantly less than those with MA. Demonstration of the prognostic value of a simple acid base disorder is remarkable. In a large trial of adult patients with respiratory failure, requiring mechanical ventilation by Esteban and coworkers,[1] it was found that MA was a stronger predictor of mortality as compared to RA, with odds ratio being 2.05 and 1.24, respectively. In addition, only MA was an independent predictor of mortality. This substantiates the fact that presence of MA is an indicator of poor outcome, as compared to RA. MA actually is a reflection of non-pulmonary organ dysfunction such as circulatory failure or renal failure, whereas RA depicts hypercapnic pulmonary organ failure. It has also been shown that mortality increases remarkably with development of associated organ dysfunctions in presence of respiratory failure.[13] In this study, hospital survival rates in patients with respiratory failure fell from 44.5% in patients with pure pulmonary dysfunction, to 16.1 and 10% for patients with associated one and two non-pulmonary organ dysfunctions, respectively. Finding of higher mortality in patients with associated MA in ACRF group (all patients with ACRF had underlying respiratory acidosis), also proves the same point. The whole study group was analyzed together to find parameters, which could predict mortality in patients with respiratory failure. High APACHE II score was associated with significant increase in mortality. Although it appears to be a useful tool to prognosticate patients of respiratory failure as a whole, it was not found useful on subgroup analysis for patients with ARF separately. As discussed earlier, failure of APACHE II score at presentation to predict mortality in patients with ARF, was a consequence of the key role played by the hospital course in affecting the outcome of these patients. It can be inferred here that, it may be useful to repeat APACHE II score estimation after admission, since this score will reflect development of organ failure during hospital course. This score is likely to be a far stronger predictor of mortality, as compared to the score estimated at presentation. Although various other studies[1],[14],[15],[16],[17],[18] found age as risk factor for increased mortality in patients of respiratory failure, we did not find any such correlation. None of the other parameters at baseline were found to predict mortality. On the other hand, lower HCO 3 and PaCO 2 levels (all three days) were associated with increased mortality. This probably reflects underlying MA due to various causes, which was associated with higher mortality. Deranged renal functions (blood urea and serum creatinine) were consistently associated with increased mortality. Renal functions at presentation did not affect mortality. This is probably due to presence of azotemia in many patients at presentation, which is usually caused by various reversible pre-renal factors such as dehydration. These patients do well if managed in time and renal functions may return to normal levels. But development of frank renal failure in patients of respiratory failure carries a grave prognosis. Finding of the serum creatinine done 48 hrs after admission as the strongest independent predictor of mortality with best AUC value on ROC curve, substantiates this point. Similar worsening of outcome of patients with respiratory failure due to development of renal failure has been demonstrated in other studies as well.[13],[14],[19],[20] Avoiding development of non-pulmonary organ failure during hospital stay should be a priority in respiratory failure patients and all possible steps should be taken to prevent its occurrence. In conclusion, although patients with ARF and ACRF may appear equally ill at presentation, mortality is remarkably higher for patients with ARF. A higher incidence of complications such as development of renal failure in patients with ARF, seems to be responsible for this increased mortality. Because of this fact, when baseline characteristics for ARF and ACRF are similar, patients with ARF should be the priority group for provision of ICU facilities. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06013t4.jpg] [cm06013f3.jpg] [cm06013t2.jpg] [cm06013t1.jpg] [cm06013f2.jpg] [cm06013t3.jpg] [cm06013f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}