 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
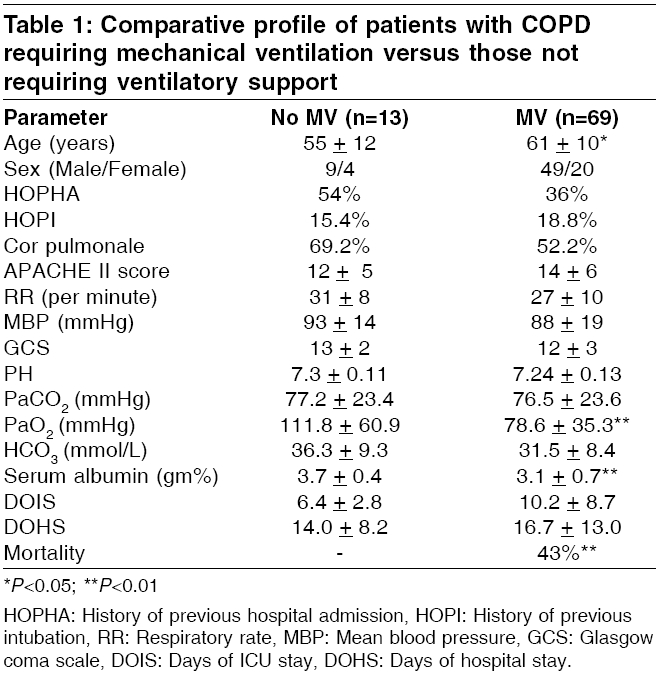
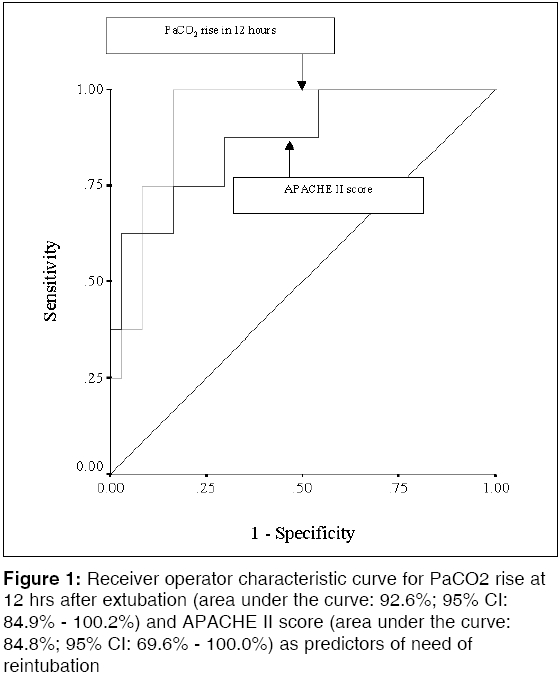
Indian Journal of Critical Care Medicine, Vol. 10, No. 2, April-June, 2006, pp. 88-94 Research Article Predictors of need of mechanical ventilation and reintubation in patients with acute respiratory failure secondary to chronic obstructive pulmonary disease Khilnani GC, Banga Amit, Sharma SK Department of Medicine, All India institute of Medical Sciences, New Delhi Code Number: cm06014 Abstract Background and Aims: To identify predictors of need of mechanical ventilation (MV) and that of reintubation, after a planned extubation, among the patients with exacerbation of chronic obstructive pulmonary disease.Materials and Methods: Prospectively collected data of 82 patients with exacerbation of COPD over a one-year period were reviewed. Clinical and demographic profile, APACHE II score, blood gas parameters and serum biochemistry, recorded at the time of admission, were compared between patients who required MV and those who did not. Parameters were also compared between the groups formed on the basis of requirement of reintubation. Results: Sixty-nine patients (84.1%) required invasive MV. Independent predictors of need of MV were pH<7.26 (adjusted OR, 95% CI) (4.9, 1.1-21.3; P =0.03) and SA < 3.5 g/dL (6.3, 1.4-27.7; P =0.01). Reintubation was required in 8 patients out of 45, who were extubated (17.8%). PaCO2 rise 12 hours after extubation (1.25, 1.0-1.5; P =0.01) and APACHE II score (1.33, 1.0-1.7; P =0.03) were independent predictors for need of reintubation. A cut off level of 7.2 mmHg for PaCO2 rise had sensitivity of 100% and specificity of 84%,for need of reintubation. Conclusions : Presence of acidemia and hypoalbuminemia at admission are predictors of need of MV, whereas APACHE II score at baseline and PaCO2 rise in the initial 12 hours after extubation, predict need of reintubation. Keywords: Acute exacerbation, APACHE II score, CO 2 narcosis, PaCO 2 Chronic obstructive pulmonary disease (COPD) is characterized by irreversible airway obstruction, leading to marked disability.[1] Gradual progressive decline of lung function is the hallmark of the disease.[1] This chronic course is punctuated by repeated episodes of exacerbations requiring hospitalization. COPD is a common disease and data from United States indicates that incidence of the disease is on the rise.[2] During the year 2000, approximately 24 million United States adults had evidence of obstructive airway disease. COPD was responsible for 1.5 million emergency department visits, 726,000 hospitalizations and 119,000 deaths.[2] The disease puts an enormous economic burden on the society and this is especially true for exacerbations of COPD. Andersson and coworkers estimated that almost 35-45% of the total per capita health-care costs for COPD are accounted for by exacerbations alone.[3] Patients with severe exacerbations requiring hospitalization and/or intensive care unit (ICU) admission along with assisted ventilation, are responsible for major share of these costs. This is largely due to higher rates of ventilator dependence, weaning failures, as well as reintubation in patients with exacerbation of COPD, as compared to other causes of acute respiratory failure.[4] Furthermore, reintubation alone has been found to be associated with increased duration of mechanical ventilation (MV), ICU and hospital stay, need for tracheostomy and hospital mortality.[5] In view of these findings, availability of parameters that could predict the need of MV as well as reintubation, would be useful. Management strategies can be modified according to these predictors which may help to improve the outcome of these patients and reduce the cost of therapy. This study was carried out to identify predictors of need of MV, requiring ICU admission for acute respiratory failure due to COPD. In addition, we made an attempt to determine predictors of reintubation, after a planned extubation, among the patients that require MV. Materials and Methods Prospectively collected data of patients with acute respiratory failure secondary to COPD, admitted to medical ICU of All India Institute of Medical sciences, New Delhi, India (a tertiary care center in north India), over a one-year period (January to December 2002), were reviewed. Diagnosis of COPD was based upon the characteristic findings on history and examination with typical radiographic abnormalities.[6] Patients with underlying COPD admitted to the ICU for another illness as primary indication, such as acute coronary event, were excluded. Similarly, patients in whom the primary cause of respiratory failure was bronchiectasis, bronchial asthma, pulmonary edema or pulmonary embolism, were not included. Finally, 82 patients with a primary admitting diagnosis of acute respiratory failure secondary to COPD, were included. All patients were documented cases with prior pulmonary function test confirmation of irreversible airway obstruction and had been receiving a combination of various bronchodilators. Management of the patients was the primary responsibility of the ICU team. Treatment strategy was individualized for each patient and was the sole prerogative of the treating physician. All patients received regular nebulized bronchodilators including salbutamol (as frequently as 2.5-5 mg every 15 minutes to every 6 hours), ipratropium bromide (as frequently as 0.25-0.5 mg every 15 minutes to 0.25 mg every 6 hours) and intravenous corticosteroids. Most patients also received antibiotics (n=75, 91.5%). Oxygen therapy (2-3 L/min) was administered to spontaneously breathing patients. The decision to institute ventilatory support was taken by the treating physician. All patients with pH< 7.35 despite optimal medical therapy but intact sensorium, maintaining organ functions and homodynamic stability, were candidates for non-invasive ventilation (NIV) as the initial strategy. Endotracheal intubation was done if the patient developed respiratory arrest, deteriorating level of consciousness, rising PaCO 2 despite maximal pharmacological treatment and deteriorating acidemia. Initiation of weaning from mechanical ventilation was considered as soon as the patients were considered capable of breathing spontaneously. Method of weaning trials included t-piece trials, gradual reduction of synchronized intermittent mandatory ventilation (SIMV) breaths and pressure support ventilation (PSV). Clinical and demographic profile at the time of admission to ICU including age, sex, smoking status, history of previous hospital admissions, history of previous intubation and/or ventilatory support, prior evidence of cor pulmonale with or without congestive heart failure, were recorded. Findings on clinical examination including heart rate, respiratory rate and mean blood pressure, were recorded. Acute physiology and chronic health evaluation II (APACHE II) score[7] and Glasgow coma scale (GCS) were recorded at the time of admission to the ICU. Acid-base abnormalities at the time of presentation were analyzed by recording the arterial blood gas analysis and serum electrolytes (estimations done on AVL 995S). Renal functions, liver functions and serum albumin (SA) done at the time of admission were also recorded. Development of complications during mechanical ventilation such as pneumothorax and ventilator associated pneumonia (VAP), were recorded. VAP was defined as per the criteria of American college of chest physicians.[8] Development of acute respiratory distress syndrome (ARDS), sepsis, and multi-organ failure was also documented. ARDS was defined as presence of bilateral pulmonary infiltrates on chest radiograph, in presence of hypoxemia with PaO 2 / FiO 2 ratio less than 200, without any evidence of left atrial hypertension (American-European Consensus conference).[9] Sepsis was defined as the presence of a clinically identified site of infection (e.g., pneumonia) and two or more of the following: temperature > 38°C or < 36°C; heart rate > 90 beats/min; respiratory rate > 20 breaths/min or PaCO 2 < 32 mm Hg; and WBC count > 12 x 10 9/L, < 4.0 x 10 9/L, or > 0.10 immature forms (i.e., bands) (American College of Chest Physicians/society of Critical Care Medicine Consensus Conference).[10] The number of weaning trials with the mode of weaning, was recorded. We speculated that need of reintubation in patients with COPD with type 2 respiratory failure, could be related to the PaCO 2 levels. The PaCO 2 levels at the time of initiating weaning, at the time of extubation and rise in 12 hrs after extubation, was also recorded. Statistical analysis Data were double entered to minimize errors and managed on an ′Excel′master sheet. Analysis was done using the statistical software ′SPSS version 10.0′ (SPPS Corp, Chicago, IL, USA). The study group was split on the basis of need of MV. Various parameters were compared between the two groups to identify the predictors of need of MV. Analysis of continuous variables was done using independent t-test, whereas non- continuous variables were analyzed using the Fisher′s exact test. Parameters significant on bivariate analysis were identified as potential predictor variables and were evaluated further using multivariate logistic regression analysis (backward stepwise method) to identify independent predictors of need of MV. Among patients who required MV and subsequently received weaning trial, reintubation after a planned extubation was determined as the dependent variable. Various baseline parameters as well as PaCO 2 levels at the time of initiating weaning, at the time of extubation and rise in 12 hrs after extubation, were compared with reintubation as the dependent variable. Independent t-test was employed for continuous variables, whereas ordinal variables were compared using Fisher′s exact test. Independent predictors were determined by multivariate logistic regression analysis. To test the predictive utility of the independent predictors of need of reintubation, receiver operator characteristic (ROC) curves were constructed for APACHE II score and rise of PaCO 2 levels following extubation, to study their utility in predicting reintubation. Statistical significance was considered at P < 0.05 (only two tailed). Results The majority of patients in the study group were males (mean age 60 + 10, range 35-85 years; M:F 58:24). In all, 79 patients required some form of assisted ventilation (94.0%). Non Invasive Ventilation (NIV) was used as an initial strategy in 17 patients (20.2%). This strategy had a success rate of 59% (n=10). The rest of the patients (n=7) required invasive ventilation. None of the patients who were given NIV developed any complications related to ventilatory support. All had to be intubated because of rising PaCO 2 levels and accompanying encephalopathy. Sixty-nine patients (84.1%) received invasive MV. The commonest mode of ventilatory support used was synchronized intermittent mandatory ventilation (SIMV) with pressure support (PS) (n=40, 58%). Other modes used were intermittent positive pressure ventilation (n=24,29%) and SIMV without PS (n=3, 3.7%). Predictors of need of mechanical ventilation Parameters were compared between patients who required MV and those who did not [Table - 1]. Older patients, those with hypoxemia, academia and hypoalbuminemia, were more likely to need MV. Independent predictors of need of MV were pH< 7.26 {adjusted odds ratio (AOR), 95% confidence intervals (95% CI): 4.9, 1.1-21.3, P =0.03} and serum albumin (SA) < 3.5 g/dL (AOR, 95% CI: 6.3, 1.4-27.7, P =0.01). Hospital course Sepsis developed in 11 patients (13.4%) and all these patients eventually died. Parameters associated with development of sepsis were high APACHE II score (18.1 and 12.6, P =0.005) and low albumin (2.6 gm and 3.3 gm%, P < 0.001). VAP developed in 8.6% (n=6) of patients who required ventilatory support and was associated with an increased stay in the ICU (18 vs 10 days, P =0.021), as well as increased stay in the hospital (30 vs 15 days, P =0.005). Outcome was not affected by development of VAP (50 vs 42.8%, NS). Weaning Weaning trials were given in 45 patients. The majority of weaning trials were given using T-piece (n=31, 68.9%), whereas reducing SIMV breaths were used in 14 patients (17.2%). There was no difference in rates of extubation, duration of stay on ventilator, or reintubation for the two strategies. Reintubation had to be done in 8 patients out of 45, who were extubated (17.8%). Mean values of various parameters were compared for the two groups. Parameters associated with need of reintubation were high APACHE II score at baseline (17.8 and 11.7, P =0.006), high PaCO 2 at 12 hours after extubation (68.5 mmHg and 56.7 mmHg, P =0.032) and PaCO 2 rise 12 hours after extubation (20.5 mmHg and 2.5 mmHg, P < 0.001). On multivariate logistic regression analysis, PaCO 2 rise 12 hours after extubation (AOR, 95% CI 1.25, 1.0-1.5, P =0.01) and APACHE II score (AOR, 95% CI 1.33, 1.0-1.7; P =0.03), were independent predictors for need of reintubation. ROC curve for PaCO 2 rise and APACHE II score showed good predictive value of both these variables for reintubation [Figure - 1], with AUC values of 0.926 (95% CI: 0.849-1.002) and 0.848 (95% CI: 0.696-1.000), respectively. A cut off level of 7.2 mmHg for PaCO 2 rise had sensitivity of 100% and specificity of 84%. Negative predictive value was 100%, but positive predictive value was only 57%. A cut-off of 11.5 for APACHE II score was associated with a sensitivity and specificity of 87.5 and 62.2%, respectively. Reintubation was associated with increased incidence of VAP (37.5 and 2%, P < 0.001), increased stay in the ICU (16 and 9 days, P =0.017), as well as significantly increased mortality (75 vs 23%, P =0.002). Discussion Patients with COPD, presenting with acute exacerbation, frequently require ventilatory support (both invasive and non- invasive mechanical ventilation). Wherever indicated, NIV was used as the initial strategy. The failure rate of NIV in the present series is comparable to what has been reported earlier.[11],[12] The only predictor of failure of NIV was presence of associated non-pulmonary organ failure (multi-organ failure, renal dysfunction or hepatic dysfunction) at admission (71.4% versus 10%, P =0.042). Therefore, whenever such patients are initiated on NIV, they should be monitored and electively intubated at the earliest indication of deterioration in status of the patient. Earlier, reported data on the incidence of need of invasive MV in patients with exacerbation of COPD has been from 9.8 to 67.6%.[13] In our series, more that 84% (n=68) of the patients required invasive ventilatory support. The higher incidence of requirement of ventilatory support in the present study is because of a significant selection bias,whereby the sickest group of COPD patients was included. Because of the perennial shortfall in the number of ICU beds, most of the patients with exacerbation of COPD who do not require ventilatory support, are managed in wards only. Therefore, the denominator in calculating the incidence of need of MV in the present study, was only a fraction of the actual number of patients with exacerbation of COPD. Presence of acidosis (pH < 7.26) and SA< 3.5 gm/L at admission were the independent predictors of requirement of MV. Finding of pH as an independent predictor of need of MV is in consonance with earlier studies.[14],[15] Patients with pH< 7.26 were almost 5 times more likely to need MV and this cutoff may be used to identify patients that require close monitoring and aggressive management. Significantly, mean pH levels were statistically comparable in the two groups (MV and non-MV group), in the present study. This suggests that the risk of need of MV does not rise in a continuous fashion with fall in pH. Nonetheless other studies have failed to document any predictive utility of pH.[16] Although few studies in the past have examined the role of SA as a marker of need of MV, its utility as a marker of nutritional status is well known.[17] Albumin is the largest fraction of the serum protein and is solely responsible for the majority of oncotic pressure exerted by the plasma. Levels of SA are known to fall in individuals with protein calorie malnutrition. It is possible that patients with poor nutritional status are likely to need ventilatory support, which may explain the predictive capability of SA. Vitacca and coworkers[18] derived similar conclusions in a study of 39 COPD patients. They found that malnourished patients, estimated by anthropometry, had higher risk of having poor outcome and increased need of MV. Also, albumin is responsible for almost two thirds of the total antioxidant capacity of the plasma[19],[20] and hypoalbuminemia may increase the oxidative stress, which already is significantly high in critically ill patients. Nonetheless, failure of albumin supplementation in improving the outcome of critically ill patients, suggests otherwise.[21],[22] In other words, it appears that SA acts only as a marker of the disease severity, rather than cause of the severe disease. The most significant result to come out of the present report, is the documentation of certain routinely performed parameters, which could predict the need of reintubation in patients who have undergone planned extubation. Reintubation was associated with increased morbidity as well as mortality and this has been observed in some other studies also.[23],[24],[25] Although it is well established that reintubation worsens outcome, what causes this worsening is not clear. It is essential to answer this question for obvious reasons. It has been suggested that reintubation only serves to act as a marker of severity of the disease rather than the cause or effect of the disease.[26] In such a scenario, predicting the need of reintubation may not affect the outcome of the patient. Nonetheless, it has also been reported clinical deterioration occurring between the time of extubation and eventual reintubation, may be responsible for poor outcome in these patients.[27] Therefore, availability of predictors for identification of patients after extubation and timely institution of ventilatory support, may reduce the increased mortality associated with extubation failure in patents with COPD. Earlier studies have found age > 70 years, severity of illness at the onset of weaning, use of continuous IV sedation and a longer duration of mechanical ventilation prior to extubation, as predictors for need of reintubation.[28] In addition, role of various physiological measurements such as ratio of frequency to tidal volume (f/VT),[29] endotracheal secretion volume and cough strength,[30] in prediction of need of reintubation has been studied. Rise in PaCO 2 after extubation, as well as APACHE II score at baseline, were independent predictors of failed extubation and had good AUC values on ROC curve. These findings have important implications. An independent association of reintubation with high APACHE II score at admission, suggests that reintubation is, to an extent, a function of severity of the diseases at baseline. That is, the poor outcome associated with need of reintubation may not be entirely due to the events that happen after extubation. Patients who eventually need reintubation, are a sicker group of patients at baseline and the need of reintubation acts as a marker of the severity of illness. Similar findings have been reported earlier as well.[26] Secondly, it is possible to predict which patients are likely to have a failed extubation, by looking at certain simple physiological variables. This seems true at least for patients with COPD. We could demonstrate that early rise of PaCO 2 after extubation, is strong predictor of need of reintubation and a cutoff level of 7.2 mmHg is associated with excellent sensitivity, specificity and negative predictive value. Positive predictive value is not enough to warrant elective reintubation for all patients with rise> 7.2 mm Hg, but such patients need close monitoring. On the other hand, a negative predictive value of 100% for this cutoff, suggests that patients with PaCO 2 rise < 7.2 mmHg, are highly unlikely to have a failed extubation. Whether this variable is the ′cause′ or ′effect′of the underlying altered patho-physiology in patients requiring reintubation, is not entirely clear. We would like to suggest that it probably works both ways. A patient who has an imbalance between respiratory capacity and load develops CO 2 retention and a rising PaCO 2 causes CO2 narcosis, leading on to further reduction in respiratory capacity. This ensues a vicious cycle, which culminates in failed extubation. Such patients should be initiated on ventilatory support in an elective manner and without losing much time. Also, patients with a high APACHE II score at baseline should be considered potential reintubation candidates and closely monitored after being extubated. We acknowledge a small sample size and retrospective design as important shortcomings of this study. Nonetheless, the present study does indicate that certain simple parameters could be used reliably to predict reintubation and help to reduce mortality in patients with exacerbation of COPD. The possibility of widespread use of such parameters for a complication of a common disease like COPD should be stimulus enough for further evaluation of these parameters, using a larger number of patients in a prospective study. It is concluded that presence of acidemia and hypoalbuminemia at admission predicts the need of MV in patients with COPD. A significant number of patients require reintubation and these patients have increased morbidity and mortality. APACHE II score at baseline and PaCO 2 rise in the initial 12 hours after extubation are independent predictors of need of reintubation. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06014t1.jpg] [cm06014f1.jpg] |
| |||||||||

{kind=link}
{kind=link}