 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
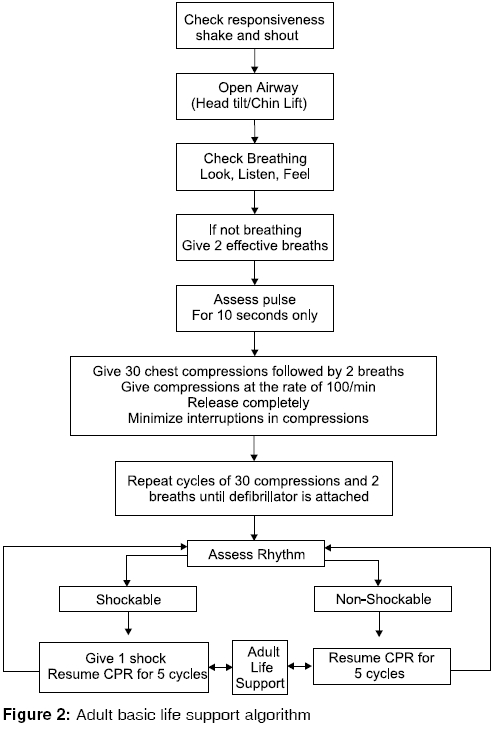
Indian Journal of Critical Care Medicine, Vol. 10, No. 2, April-June, 2006, pp. 95-104 Review Article Adult basic life support Sarin H, Kapoor D Department of Anaesthesia and Intensive Care, Fortis Hospital, Amritsar, India Code Number: cm06015 Abstract Prompt and skilful resuscitation during cardiac arrest can make a significant difference between life and death. There have been important advances in the science of resuscitation and various international resuscitation committees have formulated evidence-based recommendations for the performance of basic life support. The revised guidelines published in the year 2005 have been designed to simplify cardiopulmonary resuscitation. In this article, we have summarized basic life support guidelines for adult victims. Keywords: Basic life support, cardiopulmonary resuscitation, foreign body airway obstruction, recovery position The international guidelines for managing cardiopulmonary arrest were produced by the International Liaison Committee on Resuscitation (ILCOR) in the year 2000.[1] The 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations (CoSTR) contains new guidelines presented by ILCOR.[2] This review introduces basic life support and the guidelines adapted and produced by the European resuscitation council and the American heart association, from the consensus statement presented by ILCOR.[2],[3],[4] Basic life support (BLS) includes maintaining airway and supporting breathing and circulation without the help of any equipment. It comprises of recognition of signs of sudden cardiac arrest, heart attack, stroke, obstruction of airway by a foreign body; cardiopulmonary resuscitation (CPR); and defibrillation with an automated external defibrillator (AED).[4] The purpose of basic life support is to maintain adequate ventilation and circulation till a resource can be obtained to reverse the underlying cause of the arrest. The MONICA (multinational monitoring of trends and determinants in cardiovascular disease) Project set up by the World Health Organisation evaluated deaths from coronary artery disease in the age group of 35-64 years.[5] According to its findings, one third of people who developed myocardial infarction, died before reaching hospital. Ventricular fibrillation and pulseless ventricular tachycardia (VF/pulseless VT) accounts for 40 to 50% of all out-of-hospital cardiac arrests.[6] Majority of the cases of sudden cardiac death develop ventricular fibrillation (VF) at some point in their arrest.[7],[8] Failure of circulation for 3-4 minutes (less if the patient is already hypoxaemic) leads to irreversible cerebral damage. If defibrillation is performed within 5 minutes of collapse, the chances of survival are increased multifold. Immediate CPR is required in all cases of cardiac arrest. It is of importance, both before and after defibrillation. A small but critical amount of blood flows into the heart and brain during CPR. Various studies show that CPR started immediately after collapse from VF doubles, or even triples the chances of survival.[9],[10] CPR increases the likelihood of conversion of VF into a normal rhythm by DC shock. CPR also prevents degeneration of VF into asystole, which carries a poor prognosis.[11],[12] The chances of survival decrease by 7-10% for every minute CPR is delayed.[9] Various studies have demonstrated survival rates of 49 to 75%, when both CPR and defibrillation are carried out within 3-5 minutes of collapse.[6],[13] Death is 1.1 times more likely with each minute′s delay in CPR and defibrillation.[10] CPR should be continued until a defibrillator is available. The importance of CPR increases further, if defibrillation is not done within 4 minutes of collapse.[14] If defibrillation is attempted in a case of VF after 5 minutes of collapse, the chances of survival may be increased if it is preceded by CPR for some duration.[14],[15] CPR is also necessary for some time after defibrillation. In one study, organised rhythm was seen in only 25 to 40% of VF cases after shock delivery.[16] After defibrillation, asystole or pulseless electrical activity (PEA) is often noted for several minutes and perfusion is inadequate.[16],[17] Hence CPR is needed after defibrillation, till a perfusing rhythm is restored.[17] The American Heart Association has described a "Chain of Survival" to illustrate the sequence of events that contribute to a successful outcome after a cardiac arrest: [Figure - 1][18] (a) Immediate access to emergency medical services, in case the cardiac arrest occurs outside the hospital. (b) Early basic life support which slows the rate of deterioration of the brain and heart. In case of out-of-hospital cardiac arrest, CPR performed by bystanders increases the chance of survival. In case of an in-hospital cardiac arrest, the healthcare providers should perform CPR till the cardiac arrest team arrives. (c) Early defibrillation in indicated cases. This increases the chances of a successful outcome. In case of out-of-hospital cardiac arrest, the aim of the emergency hospital services should be to deliver a shock (if indicated) within five minutes. (d) Although defibrillation often restores a perfusing rhythm, yet it does not sustain the circulation and hence further advanced life support is required. Cardiorespiratory arrest in hospitalised patients is not a sudden unpredictable event. A few hours before cardiac arrest, clinical signs of deterioration occur in approximately 80% of the cases. The most common abnormalities are shortness of breath, an increase in respiratory rate, fall in oxygen saturation, fall in arterial oxygen tension, acidosis, increase in heart rate, fall in cardiac output and urine output < 30 ml/hr. Patients tend to be cold, clammy, confused, lethargic, or there may be a fall in the level of consciousness. Therefore it is important to recognise these signs as early identification and intervention decreases the likelihood of cardiac arrest. Basic Life Support Any potential risks associated with resuscitation of a victim should be eliminated initially. Before approaching the victim, the rescuer should be aware of any danger from electricity, gas, traffic, etc. A trauma victim should be moved by a lay rescuer, only if absolutely necessary. In cases of poisoning, care should be taken when handling the clothing of the victim or the body fluids, especially vomitus. There is no documented case of HIV, HBV, HCV, or CMV being transmitted during mouth to mouth ventilation. So far, only three cases of HIV infection acquired during resuscitation have been reported.[19] Two of the rescuers had deep needle stick injuries and the third involved heavy contamination of excoriated hands. According to Bierens and Berden, the risk for acquiring HIV infection during mouth-to-mouth ventilation is between 1 in one million and 1 in one billion depending on the population being resuscitated and the circumstances of the exposure.[20] Cases of CPR related transmission of Neisseria meningitides have however been reported. Studies indicate that herpes simplex virus (HSV) is readily transmitted from victim to rescuer and also from rescuer to victim.[21],[22] Healthcare workers should wear gloves and eye protection devices during resuscitation. All needles and sharps should be handled in a separate sharps container. Face masks with one way valves should be readily available. After ensuring his own and the victim′s safety, the rescuer should check the victim and see if he responds. This can be done by gently shaking the shoulders and asking loudly whether he is all right or not. If the victim responds, he should be left in the same position and the rescuer should get help if needed. The AHA guidelines state that if the victim is unresponsive, a lone rescuer should first call the national ambulance number and then open the airway and check for breathing. In case there are two rescuers, one of them should leave and call the national ambulance number. However, the ILCOR and ERC guidelines state that if there is no response, the rescuer should only shout for help and call for an ambulance after checking the victim′s breathing. Turning the victim onto his back on a hard surface, the rescuer should place his hand on the victim′s forehead and gently tilt his head back. The thumb and the index finger should be kept free to close the nose for rescue breathing. It has been recommended that a finger sweep should be used to remove any foreign material, only if it is visible in the oropharynx. The chin should then be lifted by placing the fingertips of the other hand under the point of the victim′s chin. A lay rescuer should always open the airway with the head tilt-chin lift manoeuvre. Various studies have shown that the head tilt-chin lift technique effectively opens the airway.[23],[24] However, when cervical spinal injury is suspected, a health care provider should open the airway using a jaw thrust without neck extension. Spinal injury has been reported in approximately 2.4% of blunt trauma cases and if there is an associated craniofacial injury or Glasgow coma scale score is less than 8, the risk increases three fold.[25],[26] In case the airway cannot be opened by the jaw thrust manoeuvre, head tilt-chin lift technique should be used, as, maintaining a patent airway is of more importance. Furthermore, manual in-line stabilisation (MILS) should be preferred to immobilization devices in suspected spinal injury cases,[27],[28] as cervical collars have been found to increase intracranial pressure and to make airway management difficult.[29],[30] Keeping the airway open, the rescuer should look for chest movements, listen at the victim′s mouth for breath sounds and feel for the exhaled air on the cheek. This should take a maximum of ten seconds. If the victim is breathing, he should be turned to the recovery position and the rescuer should immediately call for an ambulance and then reassess the patient. Various studies have shown that lay rescuers as well as health care workers have difficulty in accurately determining the presence or absence of adequate or normal breathing in unresponsive individuals.[31],[32] This could be because either the airway is not open[33] or the victim could be making occasional gasps. Agonal gasps are commonly seen in the early stages of cardiac arrest and rescuers often have difficulty in differentiating them from normal breathing.[34] If the victim is not breathing, or is making weak attempts at breathing or occasionally gasping, the rescuer should start CPR. A lone health care worker should also follow a similar sequence, except when the cause of the arrest is likely to be asphyxia (e.g., drowning), in which case the rescuer should provide 5 cycles of CPR and then leave the victim to call the national ambulance number. According to the ILCOR and AHA guidelines, when starting CPR, the rescuer should initially give two effective breaths to the victim. For this, the victim′s nose is pinched close with thumb and index finger and his mouth opened a little while maintaining chin lift. Taking a regular breath (not a deep breath), the rescuer should place his lips around the mouth of the victim ensuring a good seal and blow steadily into the mouth for about 1 second. The chest should rise and then fall, as in normal breathing. Only a small resistance should be felt during breathing. If an effective breath is not achieved, the rescuer should recheck the victim′s mouth for any obstruction and ensure proper head tilt and chin lift. Up to five attempts should be made to achieve two effective breaths. Mouth-to-nose ventilation has been recommended if a mouth-to-mouth seal is difficult to achieve, the victim′s mouth is injured, the mouth cannot be opened or the victim is in water. Mouth-to-nose ventilation has been found to be practical and effective. Mouth-to-stoma ventilation has been recommended for victims with tracheal stoma. However, there is no published evidence of its safety and effectiveness. A bag-mask device can be used to provide ventilation. If supplementary oxygen is available, it should be attached to the bag. A single rescuer using it, should be able to open the airway with jaw lift and hold the mask tightly against the patient′s face while squeezing the bag. The breath should be delivered over 1 second and the chest should rise. Bag-mask ventilation is more effective when provided by two trained rescuers. It is essential that sufficient tidal volume (by mouth-to-mouth or by mask) is given to produce a visible chest rise and rapid or forceful breaths are avoided. Aufderheide and colleagues found that hyperventilation increased intrathoracic pressure, which further decreased venous return to the heart and diminished the cardiac output.[35] Large tidal volumes also cause gastric inflation and its ensuing complications.[36] The risk of gastric inflation is increased by both high proximal airway pressure and reduced opening pressure of lower oesophageal sphincter.[37] Davis et al found that high proximal airway pressure is created by large tidal volumes, high peak inspiratory pressure, short inspiratory time, incomplete airway opening and decreased lung compliance.[38] Tidal volumes of 8-10 ml/kg have been found to maintain adequate oxygenation and carbon dioxide elimination in anaesthetised adults. During CPR, cardiac output is reduced to 25 to 33% of the normal[39] and hence oxygen uptake from and CO 2 delivery to the lungs is decreased. Various studies have shown that lower tidal volumes and respiratory rates can maintain effective oxygenation and ventilation during CPR.[40],[41] Tidal volumes of 500-600 ml (6-7 ml kg -1) have been considered adequate for adult CPR. Furthermore, oxygen level in the blood remains high for the initial few minutes after cardiac arrest and oxygen delivery to brain and myocardium is reduced by a decreased cardiac output rather than a deficiency of oxygen in blood. Hence, chest compressions are more important than rescue breaths for the first several minutes after VF cardiac arrest.[42] However, for victims of prolonged cardiac arrest, ventilations and compressions are of equal importance. A significant number of rescuers are unwilling to perform mouth-to-mouth breathing for the fear of acquiring infections,[43],[44] as mentioned previously. Research shows that outcome from chest compression without rescue breathing is significantly better than no CPR at all.[45] Even if adequate rescue breaths cannot be given, the rescuer should move on to the next step of chest compressions. The ERC guidelines state that if the victim is not breathing normally, the rescuer should immediately start chest compressions after calling the national ambulance number. The next step in CPR is assessment of circulation, which is usually done by palpating the carotid pulse. This has been reported to be an inaccurate method for confirming the presence or absence of circulation[46] and hence the various guidelines recommend that rescuers should start CPR if the victim is unconscious (unresponsive), not moving and not breathing. There is no evidence substantiating these signs of circulation to be diagnostically superior to checking the carotid pulse for assessment of circulation.[32] Lay rescuers are not required to check the pulse of the victim and can assume that cardiac arrest is present if the victim is unresponsive and not breathing. Studies have shown that health care workers have difficulty in detecting presence or absence of pulse and may take too long to check for pulse.[47],[48] A health care worker should take a maximum of 10 seconds to check for the presence or absence of pulse. If the carotid can be palpated but breathing is not present, rescue breathing should be continued at a rate of 10 to 12 breaths per minute, or about 1 breath every 5 to 6 seconds. The rescuer should reassess the pulse every 2 minutes. A maximum of 10 seconds should be taken to palpate the carotid. If the victim starts breathing, he should be turned to the recovery position. For giving chest compressions, the victim is placed supine on a hard surface and the rescuer kneels besides the victim′s thorax.[49] The heel of the dominant hand is placed on the sternum in the centre (middle) of the chest, between the nipples. The heel of the non-dominant hand is placed on top of the first hand, so that the hands overlap and are parallel to each other. The fingers of both hands are interlocked and the rescuer should ensure that pressure is not applied over the victim′s ribs, upper abdomen, or the bottom end of the bony sternum. The rescuer positions himself vertically above the patient′s chest and with his arms straight, presses down on the sternum to depress it between 4 and 5 cm (1½ to 2 inches). The contact should be maintained when the pressure is released. The chest should recoil completely before the next compression is initiated. Chest compression and relaxation times should be approximately equal. The compressions are continued at the rate of 100 times a minute. During CPR, effective chest compressions are crucial for providing blood flow. Paradis et al found in their study, that properly performed chest compressions produced a systolic arterial pressure peak of 60 to 80 mm Hg and the mean arterial pressure in the carotid artery seldom exceeded 40 mm Hg.[39] The ILCOR has emphasised that for "effective" chest compressions, the rescuer should "push hard and push fast". Insufficient depth was noted in 40% of chest compressions in both out-of-hospital and in-hospital settings.[50] Previously, sternal compression force was considered adequate if a carotid or a femoral pulse could be palpated. However, it has been shown that a venous pulse may be felt during CPR in the absence of effective arterial blood flow.[46] Various studies have also demonstrated that complete chest relaxation is necessary for effective CPR, as it allows venous return to the heart.[51],[52] Chest compression rate of more than 80 compressions per minute have been shown to achieve optimal forward blood flow during CPR.[53],[54] Hence all the guidelines recommend a compression rate of about 100 compressions per minute, compression depth of 4-5 cm and complete chest recoil after each compression. ILCOR has recommended that the ratio of chest compressions and rescue breaths should be 30:2. It has been found in various animal studies, that continuous chest compressions with minimal interruptions lead to better haemodynamics and chances of survival.[42],[55] Dorph et al have shown in an animal model of cardiac arrest, that a compression-ventilation ratio of 30:2 was associated with a significantly shorter time to return of spontaneous circulation, than continuous chest compressions.[56] Furthermore, a theoretical analysis carried out by Babbs et al has shown that the best blood flow and oxygen delivery would be provided by a compression-ventilation ratio of 30:2.[57] Rescuer fatigue has been found to be one of the factors for inadequate CPR.[58] Significant fatigue and inadequate compression rate and depth have been seen after 1 minute of CPR.[58] Therefore, it has been recommended that when 2 or more rescuers are present, the "working compressor" should be relieved every 2 minutes (or after every 5 cycles of compressions and ventilations at a ratio of 30:2). A compression-ventilation ratio of 30:2 has been recommended for both single and 2 rescuer CPR in adults. Once an advanced airway has been placed, ventilation should be provided at the rate of 8 to 10 breaths per minute. Chest compressions should be carried out continuously at a rate of 100 per minute without pauses for ventilation. CPR should be continued until defibrillator/monitor is attached, or the victim starts breathing normally. Once a defibrillator is attached, if a "shockable" rhythm (VF) is confirmed, a single shock is given. The guidelines recommend that irrespective of the resultant rhythm, 5 cycles of CPR should be given immediately after the shock, to minimise the "no flow" time Alternative Compression Techniques Cough CPR "Cough" CPR cannot be used in an unresponsive victim.[59] Several case series report that during episodes of rapid VF in supine, monitored and trained patients in the cardiac catheterisation laboratory, repeated coughing every 1 to 3 seconds maintained mean arterial pressure > 100 mm Hg and consciousness for up to 90 seconds.[60],[61] Coughing increases intrathoracic pressure and this generates blood flow to the brain and helps maintain consciousness. Prone CPR When an intubated hospitalised patient cannot be placed in a supine position, the guidelines recommend that CPR should be commenced with the patient in the prone position. Various studies and case reports have reported higher blood pressure during CPR in intubated prone patients in the hospital.[62],[63] Six case series have documented survival to discharge of 10 out of 22 intubated hospitalised patients who received CPR in prone position.[62],[63] Interposed abdominal compression In the interposed abdominal compression (IAC)-CPR technique, a rescuer provides manual compression of the abdomen (midway between the xiphoid and the umbilicus) during the relaxation phase of chest compression. IAC-CPR may be considered during in-hospital resuscitation, when sufficient personnel trained in its use are available. The purpose is to enhance venous return during CPR.[64] Various studies have reported survival rates when IAC-CPR, performed by trained providers, was compared with standard CPR in the in-hospital setting.[65],[66] Public Access Defibrillation Programmes Public access defibrillation (PAD) and first responder AED programmes have increased the number of bystanders providing CPR and early defibrillation to victims of sudden cardiac arrest, thereby increasing their chances of survival.[67] These programmes require rescuers trained to recognise emergencies, provide CPR and use the AED.[68] PAD programmes are most likely to improve survival from cardiac arrest, if they are established in areas where witnessed cardiac arrests are more common.[69] Uncontrolled studies using police officers as first responders have reported survival rates as high as 49-74%.[13],[70] Recovery position The recovery position is used in adult victims who are unresponsive but have normal breathing and effective circulation. In this position, the airway remains patent and the risk of airway obstruction and aspiration is reduced. An ideal position should be stable, near a true lateral position with the head dependent and there should be no pressure on the chest to impair breathing.[71] So far, no position has been found to be perfect for all victims. To place a victim in the recovery position, the following sequence is recommended by the ERC. In case the victim is wearing spectacles, the rescuer removes them. Then the rescuer kneels besides the victim and makes sure that both legs are straight. The victim′s arm nearest to the rescuer is placed at right angles to the body, elbow bent, with the palm upwards. Then the rescuer brings the far arm across the chest and holds the back of the hand against the victim′s cheek nearest to him. With the other hand, the rescuer grasps the far leg just above the knee and pulls it up, keeping the foot on the ground. Keeping the victim′s hand pressed against his cheek, the rescuer pulls on the far leg towards himself to roll the victim onto his side. The upper leg is adjusted, so that both hip and knee are bent at right angles. The victim′s head is tilted back to ensure that the airway remains open. The hand is adjusted under the cheek if necessary, to keep the head tilted. The breathing is checked regularly. If the victim is to be kept in the recovery position for longer periods of time, he should be turned to the opposite side after every 30 minutes to relieve pressure on the lower arm. Foreign Body Airway Obstruction ILCOR recommends that like CPR, relief of foreign body airway obstruction (FBAO) is an urgent procedure and should be taught to lay persons. If obstruction is mild and the victim can breathe, speak and cough forcefully, a rescuer should not interfere with his coughing. When severe obstruction is present, cough becomes silent, breathing difficulty increases, stridor may develop and the victim may lose consciousness. In such a situation, the rescuer should act quickly to relieve the obstruction. Various studies have reported back blows, abdominal thrusts and chest thrusts to be successful in relieving FBAO in conscious victims and chest thrusts and abdominal thrusts in unconscious victims.[72],[73] However, it has been shown that approximately 50% of the episodes of airway obstruction are not relieved by a single technique and more than one technique is required to relieve obstruction.[72],[74] For applying back blows, the rescuer stands to the side and slightly behind the victim. The rescuer supports the chest with one hand and leans the victim well forwards, so that when the obstructing object is dislodged, it comes out of the mouth. With the heel of the hand, a sharp blow is given between the shoulder blades. For giving abdominal thrusts, the rescuer stands behind the victim and puts both arms around the upper part of the abdomen. With the victim leaned forward, the rescuer clenches his fist and places it between the umbilicus and xiphisternum. With his other hand, the rescuer grasps the first one and pulls sharply upwards and inwards. The AHA recommends that if the victim is having difficulty in breathing, the rescuer should immediately call the national ambulance number. If there are two rescuers, one should call for help while the other attends the choking victim. If obstruction becomes severe, the rescuer should apply abdominal thrusts in rapid sequence till the obstruction is relieved. If the abdominal thrusts are not effective, the rescuer should start chest thrusts. If the victim is in the late stages of pregnancy or is obese and the rescuer cannot encircle the abdomen, then chest thrusts should be used instead of abdominal thrusts. If the victim becomes unconscious, the rescuer should support the patient to the ground, call the national ambulance number and begin CPR. During CPR, each time the airway is opened, the rescuer should look for an object in the victim′s mouth and if present remove it. The ERC guidelines recommend that if severe airway obstruction is present and the victim is conscious, five back blows should be applied initially. The rescuer should aim to relieve the obstruction with each slap. If five back blows fail to relieve obstruction, the rescuer should give up to five abdominal thrusts. If the obstruction is still not relieved, the rescuer should keep alternating five back blows with five abdominal thrusts. If the victim becomes unconscious, the rescuer should support the patient to the ground, call the national ambulance number and begin CPR. The guidelines state that if a health care worker can feel the pulse he should still initiate chest compressions. Conclusion All resuscitation organisations strive to prevent premature cardiovascular death. Prompt and skilful response from a trained rescuer is of prime importance in determining survival from sudden cardiac arrest. The new guidelines based on current knowledge, research and experience are considered to be the most effective and easily learned interventions. The recommendations provide simplified information and lay stress on high quality CPR. The guidelines recommend that CPR should be commenced if the victim is unconscious and not moving and breathing. A single compression - ventilation ratio of 30:2 has been designed to simplify CPR instructions, promote skill retention, increase the number of chest compressions delivered per minute and minimize interruptions in chest compression during CPR [Figure - 2].References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06015f2.jpg] [cm06015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}