 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Critical Care Medicine, Vol. 10, No. 2, April-June, 2006, pp. 117-147 Guidelines Guidelines for noninvasive ventilation in acute respiratory failure Chawla Rajesh, Khilnani GC, Suri JC, Ramakrishnan N, Mani RK, Prayag Shirish, Nagarkar Shruti, Kansal Sudha, Sidhu US, Kumar Vijay International Reviewer: Brochard Laurent, India Code Number: cm06019 Background The term non-invasive ventilation (NIV) refers to the application of artificial ventilation without any conduit access to the airways i.e., without an endotracheal or tracheostomy tube. Recently, NIV has assumed a prominent role in the management of acute respiratory failure.[1],[2],[3],[4] By avoiding endotracheal intubation, NIV prevents complications associated with invasive ventilation like airway problems, nosocomial pneumonia (21%) and sinusitis (5-25%).[5],[6],[7],[8] The use of noninvasive positive pressure ventilation has increased dramatically in the last decade due to the availability of more accessible interface and the desire to avoid complications of intubation. Its success in various conditions finds support in literature. Randomized controlled trials have proved its role in acute exacerbation of COPD, weaning failure and cardiogenic pulmonary edema. However, the definitive role of NIV in hypoxemic respiratory failure is still being evaluated. Patient selection, appropriate application of interface and proper monitoring determine the success or failure of NIV. The purpose of this document is 1. To disseminate information regarding the appropriate use of NIV by the
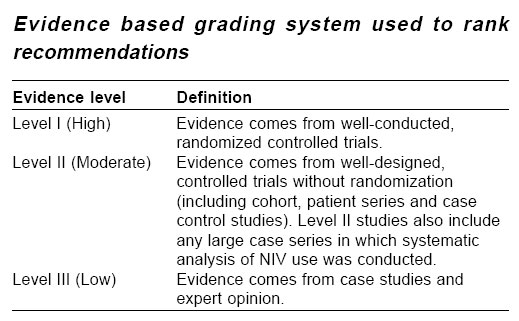
physicians involved in the care of critically ill patients in India. Methods The executive committee of Indian Society of Critical Care Medicine selected the chairperson. The chairperson then identified the members of the committee from amongst prominent workers in the field from all over India. Each member was allotted one aspect of the guidelines. All the members prepared the allotted aspect after an intensive literature search, which included Medline, Cochrane analysis and references in major articles from1980 to 2005. All these sections were presented and discussed in a meeting and modifications were suggested. The chairperson then compiled all the sections into one draft document, which was sent to all the members. This was followed by a series of meetings where each recommendation was discussed and graded. The document was also discussed electronically among members and after a consensus was reached and was sent to an international reviewer for his comments and suggestions. The guidelines were than circulated among members for final comment. This final statement represents the result of this process. Grading of recommendations Wherever applicable, recommendations were graded on the basis of modified version of the evidence-based recommendations, which have been used earlier for grading for community-acquired pneumonia.[10] All available and relevant articles till January 2006 were considered. Evidence based recommendations were chosen as they are dynamic and they can change as new evidence becomes available.
Indications There are three ways in which noninvasive mechanical ventilation
can be used[3] Hypercapnic Respiratory Failure A) Chronic obstructive pulmonary disease Patients with COPD are prone to exacerbations with progression of their disease. A significant number of COPD exacerbations are complicated by hypercapnic respiratory failure with significantly increased mortality and morbidity . Tracheal intubation and mechanical ventilation has so far been the standard modality for managing these patients; this method is associated with significant complications. In the last decade many studies have been published on the role of NIV in treating severe episodes of acute respiratory failure in COPD patients. This has dramatically modified outcome in these patients. [11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29] These well-conducted, randomized controlled trials have shown that when NIV is used in addition to standard medical therapy, it decreases rate of endotracheal intubation rate and mortality as compared to medical therapy alone. [11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21] There are only two studies, which have not shown any benefit of NIV. These studies tended to include patients with mild respiratory failure.[22],[23] NIV also shortens the length of ICU and hospital stay compared with medical therapy alone.[12],[13] Recently, meta-analyses have been published on these controlled trials. Lightowler et al in a Cochrane review have shown that the application of NIV in patients with hypercapnic respiratory failure is advantageous in terms of decreasing intubation rates, treatment failure and mortality and it should be applied early, before severe hypercapnia and acidosis ensue.[26] Keenan et al systematically analyzed the results of 15 studies and came to the same conclusions.[27] In addition, they also found that the benefits of NIV were not demonstrated in patients with mild exacerbation. Most of the above mentioned studies excluded patients who required immediate intubation. However, Conti et al[19] reported a prospective randomized controlled trial of NIV versus conventional mechanical ventilation in patients who had a mean pH of 7.2 and who failed medical treatment . In these patients, noninvasive ventilation was no worse than endotracheal intubation.[19] The intubation rate in NIV group was 52%, which is higher than in other randomized controlled trials, which is not surprising because sicker patients who had failed medical treatment were included in the study. This trial illustrated that even at this stage, intubation was avoided by NIV in almost 50% patients. The patients who could be managed by noninvasive ventilation successfully required less hospital admission in the year after hospital discharge. Squadrone et al[20] evaluated the effects of NIV in patients with COPD who were deemed to require intubation and compared the outcome with a matched set of patients who had earlier been ventilated invasively for COPD. Though 40 out of the 64 patients on NIV needed intubation, the mortality rate, duration of invasive ventilation, length of ICU and post ICU stay were not different between the two groups. Compared to those who needed intubation, patients who were successfully managed with NIV had decreased mortality rate and length of ICU and post ICU stay. Recently it has been shown that hypercapnic coma with GCS< 8 can be treated as successfully as awake patients with NIV.[21] In this open non-controlled study, between groups of acute respiratory failure patients with GCS scores less than 8 vs. more than 8, the mortality rates were similar. Thus, the beneficial effects of NIV are also seen in the sicker sub group of COPD patients. One must remember, however, that these studies were conducted in the controlled environment of an ICU where facilities for close monitoring were available. Celikel et al[18] have also shown that early NIV had a success rate of 93% whereas the same was reduced to 67% if initiated late. All these studies conclude that when applied in addition to standard medical therapy in COPD patient with acute hypercapnic respiratory failure, NIV results in the following: 1. Reduction in the rate of endotracheal intubation Recommendations 1. NIV should be considered in patients of
COPD in addition to standard medical therapy, when they present in acute exacerbation
(pH < 7.35, PaCO2 > 45
mm Hg). (Level 1) Practice Points
B) Neuromuscular disease/chest wall deformity NIV is effective in chronic ventilatory failure due to chest wall deformity and neuromuscular diseases. However, there are very few studies, which have examined the use of NIV when these patients become acutely ill. These patients constitute a very small proportion of patients with respiratory failure.[30],[31],[32] There are no randomized controlled trials but only a few retrospective case series, which have suggested that NIV alleviates gas exchange abnormalities and avoids intubation in patients with neuromuscular diseases and kyphoscoliosis who present with respiratory failure.[32] Recommendations NIV is recommended in patients with neuromuscular disease and chest wall deformity when they present in acute -on-chronic respiratory failure. (Level III) C) Acute asthma One may assume that NIV should be as effective in asthma as in COPD, both being disorders of airway resistance. However, this has not been confirmed by any randomized controlled trials. This may be due to the fact that the natural history and pathophysiology of asthma is entirely different.[33],[34],[35],[36],[37] In a retrospective analysis of 33 asthmatics, the outcome of 22 patients managed with NIV was compared with 11 patients who were managed by endotracheal intubation and ventilation. NIV patients were less hypercapnic and gases improved rapidly in this group.[33] In a randomized controlled trial, Soroksky et al[35] has shown that in selected patients with severe asthma, the addition of NIV to conventional treatment can improve lung functions, alleviate exacerbation faster and reduce the need for hospitalization. However, in another randomized trial no benefit of NIV was demonstrated.[37] Although the evidence for the use of NIV in asthma is inconclusive[36] a trial on NIV in carefully selected patients is justified, particularly in patients who fail to respond promptly to medical treatment and have no contraindication. It has also been suggested that aerosolized medicines may be delivered more effectively by NIV. Recommendations 1. NIV is not recommended
for routine use of asthma exacerbation. (Level III) D) Acute respiratory failure in obstructive sleep apnea Patients with acute on chronic respiratory failure caused by severe obstructive sleep apnea syndrome have been treated successfully with NIV.[38] CPAP has also been used in these patients of severe decompensated obstructive sleep apnea.[39] If respiratory acidosis is present, NIV should be used and they should be transitioned to CPAP once they are stable. So far, there are no randomized controlled trials to prove this application. NIV therapy has also been found to be effective in the treatment of patients with obesity hypoventilation syndrome providing a significant improvement in the clinical status and gas exchange.[40] Recommendation 1. CPAP/NIV is recommended
for obstructive sleep apnea presenting as acute respiratory failure. (Level
III) E) Cystic fibrosis There are few case series on the role of NIV in patients with cystic fibrosis. Hodson et al[41] used NIV in six patients with Cystic Fibrosis who developed acute retention of CO 2 superimposed on chronic retention. Out of the six patients, four survived until heart-lung transplant. In another large study the same team[42] used NIV in 113 patients with cystic fibrosis who were being evaluated for lung transplant and experienced acute respiratory failure. Eight had successful transplant and ten were on waiting list. NIV resulted in improvement in hypoxemia in these patients but not in hypercapnia. NIV can be used for home mechanical ventilation in children. Recommendations 1. NIV may be helpful as rescue therapy to support acute respiratory failure in cystic fibrosis, providing a bridge to lung transplantation (Level III) Interstitial lung diseases The evidence for use in interstitial lung disease (ILD) in terminal stage is limited although it has been mentioned in case series. In end stage of ILD, these patients have severe hypoxemia and low lung compliance. NIV would not be expected to offer much benefit.[43] Recommendation NIV is not recommended for interstitial lung disease with acute on chronic respiratory failure. (Level III) Acute Hypoxemic Respiratory Failure Data on successful application of NIV in patients with acute hypoxemic respiratory failure is less and conflicting. This is mainly due to varied etiologies in the sub groups of patients causing hypoxemic respiratory failure (HRF) included in most of the published studies.[44]-[59] The first RCT of NIV among non-COPD patients with HRF, conducted by Wysocki et al ,[44] found no benefit in terms of reduction of intubation rate or hospital mortality. Since then, a number of randomized controlled trials[44]-[48] that included patients of HRF have produced conflicting results. The meta analysis by Wysocki et al and Keenan et al[47],[59] of the randomized trials [44],[45],[46],[47],[48],[49],[50],[51],[52],[53],[54],[55],[56] suggests that patients with hypoxemic respiratory failure are less likely to require endotracheal intubation when NIV is added to standard therapy. However, the effect on mortality is less clear and the heterogeneity among studies suggests that its effectiveness varies among different patient populations. As such, suggesting that NIV is beneficial for all patients presenting with acute hypoxemia would be misleading.[59] In addition, the diagnostic category of hypoxemic respiratory failure is too broad to apply to individual patients in these studies. Recently, a few studies have focused on some of the individual diagnoses within the large category.[75],[76],[77],[78],[79],[80] It has been found to be very effective in cardiogenic pulmonary edema.[52],[58],[60],[69] NIV may also be efficient when some components or degree of cardiac decompensation participates in the clinical feature, even if it is not the main or only cause of episode of respiratory failure. Recommendations 1. NIV may be useful
in appropriately selected patients of hypoxemic respiratory failure. (Level
I) A) Role of NIV in cardiogenic pulmonary edema A number of randomized controlled trials[52],[53],[54],[55],[56],[60],[61] have compared CPAP or pressure support plus PEEP to standard medical therapy and found similar results with the two techniques in terms of improvement in arterial blood gases, respiratory frequency and reduction in endotracheal intubation rate. Recently, NIV has increasingly been used in combination with medical treatment for acute cardiogenic pulmonary edema.[52],[58],[60],[69] Nava et al ,[64] in the emergency department, found that NIV improved PaO 2 /FiO 2 ratio, respiratory rate and dyspnea significantly faster than the group receiving medical therapy plus oxygen. However, intubation rate, hospital mortality and duration of hospital stay were similar in the two groups. In the sub group of hypercapnic patients, NIV improved PaCO 2 significantly faster and reduced the rate of intubation compared with medical therapy. Adverse events, including myocardial infarction, were evenly distributed in the two groups. Chadda et al[65] found NIV superior to CPAP in unloading the respiratory muscles when patient were studied after at least 24h stabilization period. In another study, Mehta et al ,[57] comparing pressure support plus PEEP with CPAP in patients with acute cardiogenic pulmonary edema showed that NIV reduced the sensation of dyspnea and improved the gas exchange more than CPAP alone but they found a higher rate of myocardial infarction in the Pressure Support group. Following this, several studies have compared NIV and CPAP directly over the past year and found both to be equally effective in the treatment of acute cardiogenic pulmonary edema.[66],[67],[68] In addition, these studies also indicated that NIV does not increase myocardial infarction rates.[66],[68] Recommendations 1. CPAP/NIV are recommended in addition to standard
medical treatment in cases of cardiogenic pulmonary edema. (Level I) B) Role of NIV in transplant and Immunosuppressed patients Immunosuppressed patients are at greater risk of developing serious nosocomial infections when ventilated through an invasive route. In a randomized trial of 40 solid organ transplants patient with HRF, Antonelli et al[49] compared NIV with facemask to standard treatment and found a significant reduction in rate of endotracheal intubation, fatal complications, length of stay in the ICU of survivors and ICU mortality. However, there was no difference in-hospital mortality . In another prospective RCT, by Hilbert and colleagues,[50] 52 immuno-suppressed patients (30 patients with hematological malignancies and neutropenia, 18 who received immunosuppression to prevent rejection of solid organ transplantation and four with HIV syndrome), were randomized to receive conventional medical treatment or NIV plus conventional treatment. Patients were recruited at an early stage of HRF. NIV significantly reduced the rate of intubation and serious complications. Both ICU and hospital mortality were significantly reduced. In this prospective RCT on immunocomprmised patients treated with NIV, authors obtained impressive results in the sub group of patients with hematological malignancies and neutropenia. With use of NIV Azoulay et al have shown improved survival in cancer patients.[164] Recommendation NIV is recommended early in the course of hypoxic respiratory failure in immunocomprmised patients, particularly in those with hematological malignancies. (Level I) C) Role of NIV in lung resection surgery and abdominal surgery Thoracic and upper abdominal surgery are associated with marked and prolonged post operative reduction in functional residual capacity, leading to hypoxemic respiratory failure due to widespread atelectasis at basal lung zones. Pennock et al[70] showed significant improvement in gas-exchange and a reduction in respiratory rate 1 hour after the use of NIV. Aurient et al[71] conducted a randomized controlled trial in patients who experienced respiratory distress after lung resection. With the use of NIV, a reduction in endotracheal intubation and a clear benefit in terms of hospital survival was observed. NIV has been shown to avoid intubation in 67% of patients who developed respiratory failure after abdominal surgery. It also resulted in lower length of ICU stay and lower mortality rate.[165] Recommendation NIV may be used in patients who develop respiratory distress or respiratory failure after lung resection or abdominal surgery. (level II) D) Role of NIV in severe community acquired pneumonia Few studies have reported the use of NIV in patients with HRF in community acquired pneumonia (CAP) and published results are conflicting.[46],[72],[73] Among 30 patients with hypoxemic respiratory failure receiving NIV, Benhamou et al[92] found no difference in response rate in patients with and without pneumonia. Pennock et al[70] also reported similar results. Confalonieri et al[46] in a recent RCT demonstrated major benefit of NIV in patients with severe CAP and HRF, by reducing the rate of endotracheal intubation and complications and duration of stay. This benefit, however, was almost entirely explained by the subgroup of patients with COPD. Other studies of severely hypoxemic patients with pneumonia, have shown a high rate of failure in this sub group.[74],[75],[76] NIV cannot therefore be recommended for all patients with severe CAP. Ferrer et al[45] showed that, provided a very careful selection of the patient performed (exclusion of hemodynamic instability, several organ failures, lack of cooperation, abundant secretions etc.), NIV can be very successful in community acquired pneumonia. Recommendation NIV may be used in the ICU with caution in selected patients with community-acquired pneumonia particularly in those with associated COPD (Level II) E) Role of non invasive ventilation in ARDS There is limited literature on the use of NIV in ARDS. In an uncontrolled study by Rocker and coworkers,[77] NIV was applied with the help of facemask to ten patients with ARDS. Intubation was avoided in 67% of patients. Two controlled studies[49],[51] comparing NIV with a conventional approach included some patients of ARDS. The rate of intubation was 40% for patients of ARDS randomized to NIV and the mortality rate in these patients was 35%. Severe acute respiratory syndrome (SARS) Recently, several reports have described the role of NIV in patients with severe acute respiratory syndrome (SARS). In a study by Chen et al[78] NIV resulted in improvement of vital signs, gas-exchange and sense of dyspnea and they recommended that NIV could be used as a substitute tool for ETI in selected patients of SARS. Han et al[79] reported the successful use of NIV in hypercapnic patients of SARS. Endotracheal intubation was however required in 1/3rd of the patients who initially had a favorable response to NIV. The above results should be interpreted cautiously and one should be very careful while applying NIV in ARDS patients. It should ideally be restricted to hemodynamically stable patients who can be closely monitored and where facility for endotracheal intubation is available. Recommendations NIV may be used with great caution in cases of Acute Lung Injury and that too only in ICU (Level III). The application should be reserved for hemodynamically stable patient who can be closely monitored in an ICU where facilities for invasive ventilation are present. F) Trauma Patients who sustain trauma can develop respiratory failure. Some of these patients with a flail chest or mild acute lung injury might respond to NIV therapy. In a retrospective analysis of 46 trauma patients who were treated with NIV, Beltrame et al found rapid improvement in gas exchange and success in 72% of the patients.[80] CPAP with regional anesthesia when compared to invasive ventilation in patients with chest trauma resulted in fewer ICU and hospital days for NIV group.[81] In another study published recently, when NIV along with regional anesthesia was used in patients with blunt thoracic trauma with acute respiratory failure it proved to be a safe and effective method to improve gas exchange in these patients.[82] These patients should however be treated in ICU. Recommendation CPAP/NIV can be recommended for hemodynamically stable patients of chest trauma with flail chest. (Level II) G) Role of NIV in "do not intubate" patients There is a group of patients with acute respiratory failure who are poor candidates for endotracheal intubation due to advanced age or co-morbidity. There are also patients who do not want intubation (DNI) but accept NIV. Levy and colleagues[83] instituted NIV to a group of 114 patients with DNI status for ARF and found that 49 (43%) patients could be treated successfully and survived to discharge. Only those patients with higher baseline PCO 2 had a favorable odds ratio for survival to discharge. Patients with congestive heart failure had significantly better survival than those suffering from COPD, cancer, pneumonia or other diseases. Meduri et al had shown that NIV offers an effective, comfortable and dignified method of supporting patients with end stage disease and acute respiratory failure.[9] Practice Points for hypoxemic respiratory failure
NIV in Weaning from Mechanical Ventilation NIV can be used to reduce muscle fatigue and can thus serve as a bridge between invasive support and spontaneous breathing to reduce the time on invasive mechanical ventilation. It is attractive to speculate that the many complications of endotracheal mechanical ventilation (ETMV) can be prevented by successful early weaning to NIV. This principle can also be extended to include the postextubation period in an attempt to reduce the incidence of reintubation and the attendant risks of late nosocomial pneumonia. NIV has been applied in the following 3 ways for either reducing time on endotracheal mechanical ventilation or for preventing reintubation: 1. As a part of an early weaning strategy, when patient fails a trial of
spontaneous breathing. Case series[84] and studies by Nava et al[85] and Ferrer et al[86] support the use of NIV in scenario 1 for selected patients of COPD. However, for non-COPD respiratory and primarily non-respiratory conditions, evidence for its benefit is lacking. Nava et al[85] studied the efficacy of NIV for early extubation in patients of COPD on mechanical ventilation. In this 3-centre prospective study, patients were initially mechanically ventilated for 48 hours and then extubated after a successful spontaneous breathing trial (SBT). Those who failed the SBT were randomized to two groups. The intervention group was extubated to NIV support and the conventional group continued to be on MV for gradual weaning through daily reductions of pressure support. There were predetermined criteria for reintubation. When NIV was thus combined with a 48-hr period of invasive ventilation, the total period of ventilation, ICU stay, incidence of pneumonia and 60-day mortality were reduced. In a prospective, randomized, single center study by Girault et al ,[87] continued invasive pressure support was compared with systematic extubation to NIV support in patients who failed a 2-hour weaning trial. With matched baseline characteristics, the NIV group had a shorter duration of invasive ventilation but there was no reduction in the total duration of respiratory support or of 3-month mortality. Ferrer et al[86] similarly studied the efficacy of NIV in reducing the time of weaning from invasive ventilation. This multicentre Spanish study involved 43 mechanically ventilated patients who had failed weaning trials for 3 consecutive days. NIV was applied virtually continuously in the first 24 hours postextubation. This study also showed decreased mortality, ICU days and incidence of VAP, septic shock and total mechanical ventilator days in the NIV as compared to the control group. Additionally, this study also showed a reduced incidence of tracheostomy in the NIV group. NIV application to all immediately postextubated patients had no impact on duration of ICU stay or reintubation rates.[88] However, recently, Ferrer et al[89] demonstrated in a RCT that when NIV was applied immediately after extubation to those patients, who had high risk of respiratory failure (age>65 yrs, APACHE II>12 at the time of extubation, cardiac failure at the time of intubation), it resulted in decreased reintubation and ICU mortality in this group as compared to the controls. Hilbert applied NIV intermittently in 30 patients of COPD in whom postextubation failure occurred within 72 hrs. He found significant reduction in reintubation rates, duration of MV, ICU stay and mortality in patients, who also received NIV support as compared to those who received only medical therapy.[90] Keenan et al ,[91] in a single center, prospective randomized study applied NIV to half the patients of a heterogeneous group who had postextubation failure within 48hours. Although the duration of mechanical ventilation decreased in the NIV group, there was no significant reduction in mortality, reintubation rates or duration of ICU stay. However a recent, prospective, randomized, multicentre study involving 37 centers from 8 countries, showed different results. 221 patients who developed post extubation failure within 48 hours were randomized for NIV vs. standard treatment. There was no difference in reintubation rates, which was 25% in each. Significantly, there was a trend towards a higher mortality in the NIV group (26 vs. 14%, P = 0.48). The median time from extubation to reintubation was also significantly more in the NIV group (12 hours vs. 2.5 hours P =0.02). The higher mortality in the NIV group was attributable to the delay in reintubation, as 38% of those who were reintubated died in this group as compared to 22% in the standard treatment group ( P = 0.06). There was a trend towards benefit of NIV in the subset of COPD patients but the patient number was too small for analysis.[92] Recommendations 1. NIV may be used to expedite weaning from invasive
ventilation in uncomplicated cases of COPD who fail a trial of spontaneous
breathing. (Level II) Practice Points If NIV is applied for weaning from invasive mechanical ventilation or for postextubation failure in COPD, the following procedure could be adopted:
Contraindications There are no absolute contraindications for the use of NIV. Some contraindications have, however, been suggested. Most contraindications have been determined by the fact that they were the exclusion criteria in many studies.[93],[94]
1. Inability to protect the airways - comatose patients, patients with CVA or bulbar involvement, confused and agitated patients. Predictors of Success with Noninvasive Ventilation It is evident that not all patients with respiratory failure may be suitable for the successful application of NIV.[12],[95],[96] NIV has not been universally successful, with reported failure rates of 7-50% mainly due to the heterogeneity of the study populations.[27] It would appear, that those with a very mild form or very severe form of the disease do not benefit from NIV.[26] Justifiably, there are concerns about incorrect selection of patients leading to delay in instituting invasive ventilatory support. NIV is not a substitute for endotracheal mechanical ventilation, but only a way to prevent it by providing support early enough, before severe derangements take place.[28] Understanding the determinants of success will help in accurate patient selection for NIV and a timely switchover to invasive mechanical ventilation. The following factors have been considered to influence immediate failure with NIV application: 1. The baseline respiratory abnormalities at admission like respiratory rate,
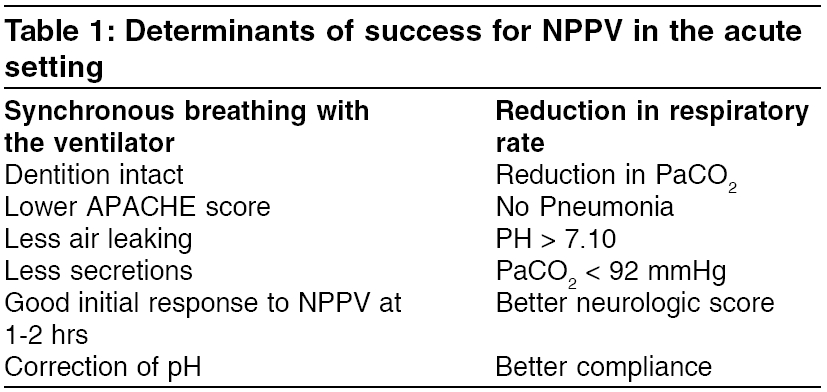
heart rate, pH and paCO 2 Soo Hoo et al[98] retrospectively studied a small number of patients who received nasal NIV. No differences in age, baseline pulmonary function or respiratory rate were found between those who succeeded and those who failed NIV. They also found that patients with hypercapnia at baseline did better as compared to those with hypoxemia alone. In 17 consecutive patients with respiratory failure due to a variety of causes, Wysocki et al . found that those who were successfully ventilated with NIV had a higher pCO2 and lower pH (7.33 vs 7.45) and a lower A-a o2 difference at baseline.[99] However, Ambrosino et al , on the other hand, in a retrospective review of a larger study of 59 episodes in 47 patients of COPD found that lower baseline PCO2 values (79 vs. 98) and higher pH values (7.28 vs 7.22) correlated with success of NIV support . Keenan et al in a recent systematic review of 15 randomized controlled trials observed that the benefit of NIV in COPD is demonstrable only in those with severe exacerbations and not in those with milder ones.[27] The level of consciousness at admission has been used to predict success or failure. Most studies have excluded patients with altered sensorium due to theoretical concerns about the risk of aspiration. Guidelines have also cautioned against its use in the presence of altered consciousness.[3] Anton et al[101] studied 44 episodes of exacerbations in 36 patients of COPD and confirmed the findings of Ambrosino et al[100] that baseline level of consciousness and pH values correlate with success. Several studies have however demonstrated success with NIV in the presence of altered sensorium and even coma.[102],[103] Benhomou achieved a success rate of 65% even in those with severe respiratory acidosis and encephalopathy.[104] More recently, Diaz et al showed that patients in hypercapnic coma with GCS< 8 can be treated as successfully with NIV.[21] Plant et al in a recent, large, multicentric, prospective study concluded that lower pCO2 and higher pH levels after 2 hrs NIV support correlated with success and that it is possible to calculate the risk for intubation based on these and other values.[96] In a prospective, randomized controlled trial Confalonieri found that in the subgroup with COPD, the 2 month survival rate was better in these who received NIV than in those who received conventional treatment alone.[46] Baseline APACHE scores were found to have no significant impact on the outcome with NIV, although its efficacy differs in various disease conditions.[105] Plant et al , however, in a prospective multicentre study found correlation of APACHE> 29 with failure of NIV. Response to NIV may also indicate the chances of success. Studies appear to indicate that this can be gauged early within the first 2 hours. Ambrosino et al went on to suggest that those who did not improve within 1-2 hrs in terms of PCO2 and pH values should be intubated. Carratu et al[106] have shown that patients who improve have increased pH and decreased PaCO 2 at 2 hours post NIV whereas those who fail have no change in these two parameters. Other predictors of early failure were a low pH, low GCS and higher APACHE II scores. In a failure risk model for NIV in COPD, Confalonieri et al[107] have recently shown that a GCS < 11, APACHE > 29, respiratory rate more than 30 and pH < 7.25 predicted a 50% failure risk and a pH of less than 7.25 at two hours post NIV predicted a 90% failure risk. Several other studies have adopted short-term (1-4 hours) trials to predict failure and indeed most guidelines advice this.[3],[43],[102],[105],[107],[108] Benhomou noted that the only factor that determined outcome was the tolerance to the mask.[104] Similarly, Ambrosino found compliance to be an important factor. Air leak is another factor recognized to be important.[100] A late failure, i.e., respiratory failure occurring after 48 hrs of support with NIV has been recognized. Moretti et al[109] found that 23% of patients deteriorated late. When those who refused intubation were then given more aggressive NIV, they did worse in the in-hospital period than those who had accepted invasive ventilation (mortality of 93% compared to 52%). Patients with late failures had significantly lower activities of daily living (ADL) scores, lower pH and associated complications at admission. The determinant of success of NIV are summarized in [Table - 1]. Recommendations 1. NIV is likely to succeed in patients with
exacerbations of COPD of more than mild severity and in selected cases of hypoxemic
failure. Practice Points
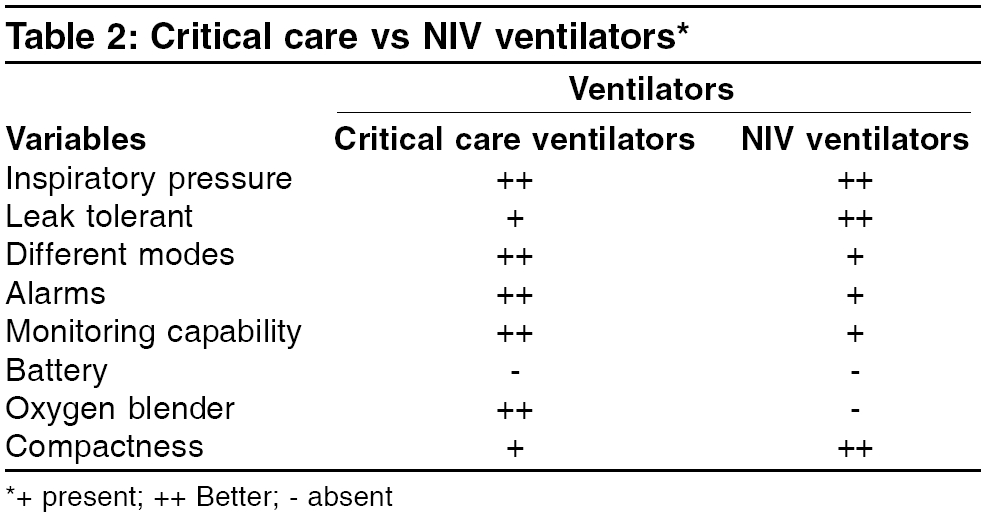
Application of Noninvasive Ventilation Modes of noninvasive ventilation All modes of ventilation that are used invasively can theoretically also be used for applying noninvasive ventilation. However, NIV is usually delivered in the form of assisted ventilation where every breath is supported. Rarely however, controlled mechanical ventilation is used.[110] There are four principal modes in which noninvasive ventilation can be used: Controlled mechanical ventilation There is no patient effort required and the ventilator provides full ventilatory support. On NIV machines this is referred to as ′timed′mode (T). Assist control ventilation The machine provides ventilatory support in response to the patient′s breathing effort but provides back-up safety rate, should the patient not trigger the machine. This mode is referred to ′spontaneous / timed′mode on NIV machines (S/T).′ Assist mode The machine provides ventilatory support in response to the patient′s breathing effort but provides no back-up safety rate, should the patient not trigger the machine. This mode is referred to ′Spontaneous′mode on NIV machines (S). CPAP A constant pressure is applied to the airway throughout the respiratory cycle. In acute respiratory failure, it is used primarily to correct hypoxemia. It is not a ventilatory mode and is used to correct hypoxemia in acute respiratory failure. Cardiogenic pulmonary edema is the main indication for CPAP. Proportional assist ventilation (PAV) The ventilator assists the patient by generating volume and pressure in proportion to patient′s effort creating a ventilatory pattern that matches metabolic demands on a breath-by-breath basis. Till date, there is no data to show any advantage of PAV. Equipment to be used for Niv and its Maintenance Ventilators Conventional ICU ventilators with full monitoring and alarm systems, portable volume preset ventilators and portable pressure preset ventilators have all been used for providing NIV. The advantages of typical ICU ventilators are the presence of full alarm systems, ability to deliver a precise/high FiO2 and the ability to separate inspiratory and expiratory gas mixtures thereby preventing the complications of rebreathing. Newer NIV ventilators incorporate many of these features for use in the acute setting, albeit at significantly increased cost. Portable non-invasive ventilators and critical care ventilators are equally effective when used for NIV.[110] Ventilators with oxygen blenders are preferred for patients with hypoxemic failure. A comparison of critical care ventilators and NIV ventilators is shown in [Table - 2].[112] NIV ventilators can be basically classified into pressure or volume preset, though some models incorporate both modalities in a single machine. In volume-preset ventilation, the set parameter is the tidal volume delivered and airway pressure is the variable depending on lung characteristics. In pressure-preset ventilation, the set parameter is the applied airway pressure and tidal volume delivered is the variable. Pressure preset ventilation could be either pressure controlled or pressure support. In pressure controlled ventilation the delivered pressure and the time for which it is applied is preset. In pressure support ventilation, the applied pressure is preset but the duration for which it is applied is patient effort dependent. Pressure support breath is terminated when the flow rate decreases to a predetermined percentage of the initial flow rate. Most portable NIV pressure ventilators use the pressure support option. Although the concept of NIV was started with the use of volume-preset ventilators, pressure preset ventilation is now the predominant mode used in NIV. NIV ventilators providing bilevel ventilation are the most popular. These machines deliver two treatment pressures. A higher pressure is applied when the patient inhales and is called IPAP (inspiratory positive airway pressure) and a lower pressure is applied when the patient exhales called the EPAP (expiratory positive airway pressure). The difference between these two pressures is the effective pressure support. EPAP is equivalent to applying PEEP in a spontaneously breathing subject. The advantage of volume-preset ventilators is that they provide a relatively constant tidal volume in the face of changing lung characteristics (increasing airways resistance/worsening lung compliance) whereas with pressure-preset machines the tidal volume will vary with changing lung characteristics. The advantage of pressure-preset machines is that they compensate for leaks, which are common in patients on NIV, either from the mask or the mouth. Most pressure-preset machines also offer facility for EPAP, which has advantages in certain patients. The peak airway pressure can also be limited unlike volume-preset machines, which do not limit peak pressure. This can create problems of gastric distension and barotrauma in certain susceptible patients (bullous lung disease). Another great disadvantage of volume-preset machines is that the flow in them is fixed and if the flow demand of the subject is greater ′flow starvation′ and consequently patient ventilator asynchrony will result. In pressure-preset machines, flow will vary according to patient′s demands making it easier for a subject to synchronize with the ventilator. Volume preset machines also tend to be more bulky and costlier when compared to their pressure counterparts, which are lighter and more portable. There have been a number of studies comparing volume and pressure preset machines in various groups of patients. Pressure preset ventilation has been shown to be as effective as volume preset ventilation in terms of improving breathing pattern and gas exchange parameters.[113],[114],[115],[116] Pressure preset machines are also simpler to use, lighter and cheaper.[117] Lab studies using lung models have also shown the better leak compensation ability of pressure-preset ventilation.[118] The choice of a machine providing assist or assist control mode depends on the patient′s disease severity. In sick patients, who are being ventilated for acute respiratory failure, a machine with assist/control facility is desirable whereas a machine with only assist mode could ventilate a stable patient with chronic respiratory failure on domiciliary ventilation. There is a substantial cost difference between these two types of machines. Staff familiarity and training with the ventilator is an important determinant of success and it is desirable to use a single model of ventilator in a particular area. Use of EPAP / bi level machines The ability to provide an EPAP on pressure-preset ventilators is advantageous. Unlike ICU ventilators, which separate inspiratory and expiratory gas mixtures, portable ventilators used for NIV have a single tubing with a potential for rebreathing expired gas.[121] The application of EPAP flushes dead space CO2 and prevents rebreathing. EPAP also helps in alveolar recruitment, prevents atelectasis and stabilizes the upper airway during sleep. EPAP has been found to be more useful in improving gas exchange parameters in patients with chest wall/neuromuscular disease as compared to patients COPD.[122] In patients with COPD who have significant intrinsic PEEP, EPAP can offset this PEEP, decrease the work of breathing and improve trigger sensitivity.[123] Triggering Triggering or changeover from expiration to inspiration, is crucial for the success of NIV. A ventilator that triggers to the inspiratory phase in a very sensitive manner, thereby responding to patient′s efforts, prevents ventilator-patient dysynchrony. At the same time, it should not be so sensitive that it auto-triggers.[124] Both pressure and flow triggering have been used and no clear superiority of one mode over the other has been established. In patients with COPD, flow triggering, by ensuring a constant flow through the circuit, does reduce the amount of auto-PEEP thereby ensuring some advantage for flow triggering.[125] In general, flow triggered devices appear to be more sensitive than pressure triggered devices and are associated with a lesser work of breathing.[126] Cycling Cycling or changeover from inspiration to expiration, in harmony with the patient′s breath, is another important function that a good ventilator must be able to perform. Cycling is also called expiratory triggering. The criteria used for expiratory triggering can have an impact on the efficiency of NIV and patient-ventilator synchrony. The usual criterion used in pressure support ventilators is a decrease in inspiratory flow from a peak to a threshold value (for example 25% of peak flow). This varies amongst various NIV machines. Since most patients with COPD or air leaks have high end inspiratory flows, a high flow threshold (25 to 40%) should be chosen for these patients as a lower threshold may lead to prolonged inspiratory times. Ventilators with a facility for adjustable maximal inspiratory times also permit better patient-ventilator synchrony. Settings the maximal inspiratory time (Ti) at one second is a reasonable approach. When patients with COPD have air leaks, the ventilator does not decrease the inspiratory flow, thereby not allowing the decrease in inspiratory flow, which cycles the machine to expiration. This leads to prolonged inspiration and patient-ventilator dysynchrony. By setting the inspiratory duration to no more than half the respiratory cycle duration, this effect can be minimized.[123],[127] Therefore, machines with adjustable expiratory triggers offer advantages. Alarms Alarms on non-invasive ventilators are basic and detect disconnection (low pressure alarm), high pressure, worsening leaks (flow alarm) and power failure. More sophisticated alarms add to the complexity and cost of machines. As NIV is used on more stable patients than conventional ventilation, a whole lot of alarms are not needed. Oxygen administration Supplemental oxygen can be administered by connecting oxygen directly to a port on the mask or to a T-connector in the ventilator circuit. Unlike classical ICU ventilators, non-invasive ventilators lack the ability to deliver precisely controlled oxygen-air mixtures to patients. The FiO2 will vary according to the patient′s respiratory pattern. High levels of FiO2 cannot be achieved because of dilution by base flow (EPAP). One can only achieve a high Fio2 with ICU ventilators. The best way to monitor oxygen administration is by pulse oxymetry. Humidification As physiological humidification mechanisms are unaltered in NIV and much of the air being breathed is ambient and consequently better humidified, humidification is not routinely needed. It may be useful in patients with thick or tenacious secretions and patients who develop nasal stuffiness, dryness and congestion. It can be provided with a simple or heated pass-over humidifiers, a pass-through humidifier or a heat and moisture exchanger. Whereas the first two require an extrinsic water source, heat and moisture exchangers reuse the moisture in the expired air for humidification. It is important to remember that these devices can alter the triggering characteristics of the ventilator and caution needs to be exercised. This problem occurs least with pass over humidifiers. It is important to remember that air leaks will produce increase in the base flow with consequent more nasal symptoms and rectification of the air leak by appropriate methods alone can circumvent the need for additional humidification.[129] A ventilator-designed specifically for NIV should therefore comprise the following features:
Additional desirable attributes include adjustable pressure rise time (ramp), adjustable inspiratory and expiratory triggers, battery backup, simple control knobs and ability to prevent inadvertent change of parameters (cover or lock out facility). Recommendations 1. Both ICU ventilators
and portable NIV ventilators can provide NIV. Portable
pressure preset bilevel ventilators
are advantageous
in terms
of patient comfort. They are also less expensive, lightweight and
easier to
maintain.
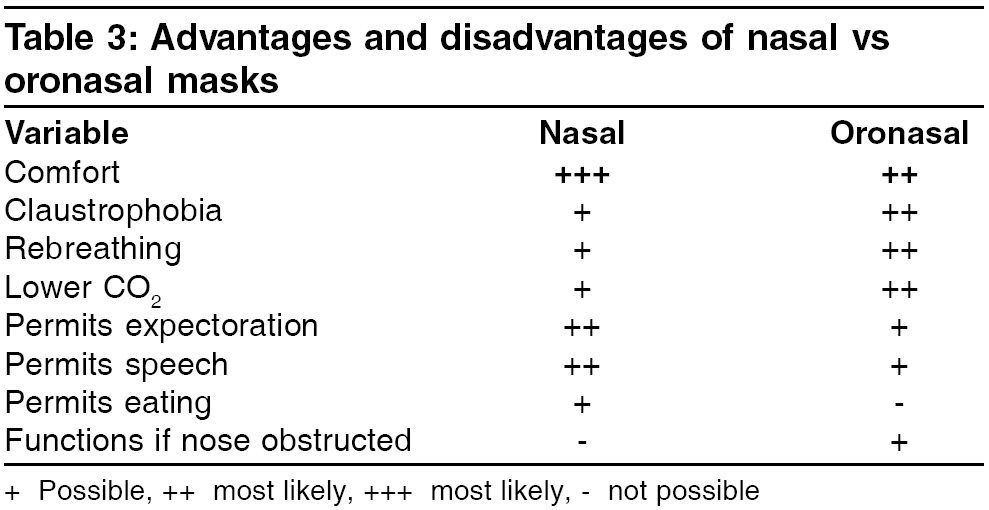
(Level III) Patient Ventilator Interface Interfaces are devices that connect the ventilator tubing to the patient and facilitate the entry of pressurized gas into the upper airways during NIV. These are crucial for the successful implementation of NIV. Currently available interfaces for non-invasive ventilation include nasal masks oronasal (full face) masks, nasal pillows, mouthpieces and the newer ′total face′helmets. Masks, however, remain the most common interfaces for NIV. They are available in multiple sizes to suit pediatric and adult patients. It is important to choose the appropriate (small, medium, large, wide or narrow) mask for best results and compliance with NIV.[130] The advantages of nasal mask include less dead space, less claustrophobia and minimum complications especially if vomiting occurs. However, full-face masks are used in acute respiratory failure since very dyspneic patients are mouth breathers. It is especially important to remember that full-face masks can add substantial dead space with consequent risk of rebreathing expired gas mixtures.[131] They also tend to be more claustrophobic. There are not enough published studies to make firm recommendations and there are not many patients′tolerance direct comparison studies of efficacy. Anton et al compared the efficacy and patient tolerance of nasal and full facemasks during acute exacerbations of COPD. They concluded that NIV improves ABG and respiratory indices regardless of type of mask used.[132] Navalesi et al compared the efficacy of NIV using nasal and full facemasks in patients with chronic respiratory failure. They found that the nasal mask was better tolerated, though the minute ventilation was significantly higher and PaCO 2 was significantly lower with a full facemask.[133] Studies in patients with acute hypercapnic respiratory failure have shown an overall bias in favor of a facemask in producing quicker improvement in blood gases. A recent randomized controlled trial comparing nasal and oronasal masks found both to be equally efficacious in the reduction of PaCO 2 or respiratory rate in patients with acute respiratory distress, though the full facemask was better tolerated.[134] Recently, a novel interface, a helmet, has been described, which is a clear plastic cylinder that fits over the head and seals with straps under the shoulders. It does not seal the nose and mouth, thereby improves comfort. Two studies have compared CPAP via helmet in patients of hypoxemic respiratory failure with historically matched controls who used standard full-face masks. Both studies found that the helmet permitted more prolonged delivery of CPAP and was better tolerated.[135],[136] However, in patients with hypercapnic respiratory failure due to COPD, the helmet appeared to be less efficient.[137] A variety of mask accessories are available that optimize mask fit, comfort and prevent troublesome side effects like nasal bridge pressure sores and leaks. Mask templates are available for sizing masks for individual patients. Choice of headgear or the strap that hold the mask is especially important and an element of elasticity must be present in the headgear material to prevent undue tension on the subject′s skin, especially the nose. Mask cushions help in increasing comfort and preventing leaks and excessive pressure on the skin. Foam spacers aid in prevention of nasal bridge pressure sores by transferring pressure onto them. Elastic chinstraps are particularly useful in preventing air leaks through the mouth. Masks with anti-asphyxia valves permit breathing, if the ventilator stops functioning. The range of accessories is large and their optimal use is best learnt by continuous practice of NIV. Mask selection Important consideration when choosing between masks is listed in [Table - 3].[112] Exhalation devices A variety of exhalation devices are available which vent the expired air to the exterior and also introduce an intentional leak in the system to flush the mask and circuit, thereby preventing rebreathing. These could either be simple exhalation ports built into the mask or could take the form of a separate attachment in the circuit (simple swivel valves, disposable exhalation ports or non-rebreathing valves). It is important to remember that CO 2 rebreathing can occur with NIV using standard exhalation valves. Moreover, masks add significant dead space. If a patient while on NIV has unexplained rise of CO 2 or non-improvement of CO 2 , this possibility should be considered. This problem can be tackled by either using a non-rebreathing valve or by increasing the level of EPAP, which flushes the mask and circuit. However, it is important to remember that at commonly used levels of EPAP, especially when the respiratory rate is high, a substantial rebreathing volume may still be present.[138] Because the ventilators trigger algorithm takes leak flow into account, only breathing circuits, exhalation valves and masks that are recommended by manufacturer should be used. Recommendations 1. Both nasal and full-face
masks can be used for providing NIV successfully. However, in the acute setting
full-face masks appear to be advantageous. (Level
I) Maintenance All ventilators should be maintained strictly according to the manufacturer′s recommendations. This includes both preventive maintenance and rectification of faults by qualified personnel. Care of the ventilators should be delegated to a specified person and all ventilators when not being used should be parked in a single designated area of the hospital. An inventory of equipment should be maintained. Since most ventilators have a base flow (EPAP) even during expiration, there is no airflow from the patient back into the ventilator. Therefore the risk of contamination of the ventilator is extremely low, especially when an outlet bacterial filter is being used. Superficial cleaning of the ventilators exterior with a slightly dampened cloth and a mild detergent between patient uses is satisfactory. Unplug the unit before cleaning. Ensure that the unit is dry before plugging it in. Do not use bleach, chlorine or alcohol based solutions to clean the exterior of the ventilator. The air inlet filter on the ventilator should be regularly inspected to see if it is blocked by dirt or contains holes and replaced when it appears dirty. There is no firm limit of time in which the filter has to be changed since the life of the filter will depend on the dust in the ambient atmosphere. Follow the manufacturer′s recommendations regarding the time frame for change. The filter must be changed when the unit is unplugged. Under no condition, should the unit be running without a filter in place. Only the filter recommended by the manufacturer should be used. Failure to replace a dirty filter may cause drop in ventilator flow and pressures and may elevate the operating temperature of the machine with consequent damage to the sensitive ventilator internal circuitry. All filters are disposable and must not be reused after washing. A ventilator performance verification check should be performed periodically and preferably before use in each new patient to see if the ventilator is adequately pressurizing. The aim is to see whether the ventilator is indeed pressurizing the circuit at the same level as set on its control. This can be done in ventilators with a built in pressure monitor or a simple hand held commercially available manometer. This can be done by occluding the circuit outlet and measuring the pressures at the outlet and ensuring that the pressure matches with that set on the machine. This should be done at different settings of pressure, for example, at 5 cm, 10 cm, 15 cm of IPAP and EPAP. This should be done in all the modes available on the ventilator. The triggering and cycling function of the machine should be checked in all the modes (S, S/T and T). By creating a small leak in a circuit to simulate a trigger, the cycling from IPAP to EPAP can be verified. It is also important to see whether the unit cycles at the set rate on the BPM control in the S/T and Timed modes. If the ventilator is equipped with alarms, verify the functioning and responsiveness of the alarms and their settings. If an outlet filter is being used, it is important to know its resistance characteristics. The pressure at the mask port should be verified when the ventilator is in use to see if the filter is causing any pressure drop in the circuit. Ventilator accessories like fuses and batteries should be replaced strictly following the specifications and procedures as described by the manufacturer. No unqualified personnel should be allowed to service or repair the unit. Electrical safety checks should be undertaken at least once a year. It is helpful to have a maintenance schedule so that planned preventive checks can be undertaken. An annual maintenance contract with the manufacture is recommended. Accessories All accessories stamped, as single use should not be recycled amongst patients. Masks and exhalation valves require high-level disinfection between patients. The manufacturer′s recommendations should be strictly followed as regards to the nature of the disinfecting agent. Both heat (dry-pasteurization, moist-autoclaving) and chemical methods (per acetic acid, glutraldehyde) are used. While using heat, it is important to know the temperature, duration of exposure and type of heat used. While using chemical disinfection, it is important to know the type of chemical and its concentration and exposure time. Cleaning and disinfecting of accessories It is not recommended to re-use disposable interfaces. The following recommendation is only for re-usable interfaces. Re-usable masks should first be cleaned, prior to using any disinfection or sterilization method. Steps
Reusable ventilator tubing is difficult to sterilize by these methods because of its long length and should preferably be autoclaved. All fabric accessories (headgear, chin straps) should be washed at 65 degree centigrade cycle for 10 minutes and dried before use. This cycle is available on most washing machines. Drying of all masks and accessories should take place in room air and not in sunlight. Automated combined washing/disinfecting/drier systems are available, though they add cost. Recommendations 1. Each unit should have a person designated
for maintenance of ventilators. Qualified personnel should do preventive
maintenance according to the manufacturer′s
recommendations (level III). Practice Points for equipment
Practical Application Patient selection The success of NIV depends on selecting the right patient. This process should take into account the diagnosis, clinical status of the patient, risk of failure and clinical judgment of the caregiver. One must also consider the evidence supporting the effectiveness of NIV in that particular patient. It has been recommended that the need for ventilation according to clinical criteria must first be established [Table - 4]. Practice Points Application of NIV using portable pressure ventilator (139) 1. Choose the correct interface. When NIV is being initiated for acute respiratory failure, close monitoring and the capability to initiate endotracheal intubation and other resuscitation measures should be available in the same setup. Start NIV preferably in the ICU or in the emergency room in acute respiratory failure. Application of NIV using a critical care ventilator 1. The first step is to select a ventilator, which is capable of fulfilling
the needs of the patient. Using pressure approach
Monitoring Monitoring is important not only for optimizing ventilator setting, but also to warn against impending catastrophe if NIV fails.[93] 1) Subjective response Once NIV is successfully initiated the smooth adaptation of the patient to the ventilator is very important. One should try to make the patient comfortable by loosening the head strap or changing the interface. NIV should alleviate his symptoms like dyspnea. Once the patient is more comfortable, he tolerates NIV better. 2) Physiological response Simple vital sign should show an improvement. These can be assessed by examination of chest wall movement, heart rate, respiratory rate, mental state and patient coordination with the ventilator. One of the first signs of a good response to non-invasive ventilation is a drop in the respiratory rate within a first few hours. Evaluation of the patient ventilator synchrony is difficult without visualization of flow and pressure waveforms. This is possible in ICU ventilators with graphic displays and advanced NIV ventilators. Air leak and patient ventilator asynchrony should be monitored and corrected as and when required and one must remember that the tidal volume displayed may be misleading, particularly during use of bi-level ventilators. The readout is usually inaccurate in the presence of air leaks. 3) Adequate gas exchange Oxygen Saturation or pulse oxymetry in the acute setting is a most fundamental measurement and should be maintained> 90%. ABG is used to judge the effectiveness of noninvasive ventilation. In acute respiratory failure, ABG should be checked at baseline and at 1-4 hours. A number of studies have shown that improvement in arterial blood gas tensions particularly in pH, after a short period of NIV predicts a successful outcome.[3],[43],[102],[108] It is recommended that ABG be done at least once a day in stable patients. Before discontinuing NIV, the patient′s ABG without NIV for one hour may be a good guide to predict weaning from NIV. Problems and Complications NIV is both safe and well tolerated in both acute and chronic settings, when applied in appropriately selected patients. However, there can be problems, which can be solved by judicious application of NIV. A) Problems related to the interface Interface related problems are the most commonly encountered complications of NIV. An improperly fitting mask and excessive strap tension cause discomfort (30-50%), nasal bridge redness (5-10%), feeling of pressure over nose[3] and claustrophobia (5-10%). The discomfort at the point of skin contact is related to the strap tension necessary to control air-leak. Pressure sores occur when excessive pressure is applied for too long.[140],[141] Practice Points
B) Problems associated with air pressure and flow
Practice Points
C) Problems associated with intolerance to NIV Intolerance to NIV may be due to mask intolerance or patient ventilator asynchrony. Improper size or fitting of mask and excessive strap tension are the important reason for mask intolerance
Practice point
D) Problems associated with failure to ventilate adequately Failure to ventilate could be due to air leaks, rebreathing, poor patient compliance or progression of the primary disease.
Major complications Major complications are infrequent (5%) if the patient is appropriately selected. They include 1. Delay in intubation and worsening of prognosis. Practice point
Location of NIV It is understandable that various countries have different standards of care and definitions of ICU, high dependency unit (HDU) and general ward. Even in our country, model of hospital care varies from city to city. Different patterns of staffing, facilities, resources, degree of training and monitoring systems may be prevalent in ICUs, HDUs and general wards. For discussion purposes on NIV we will define these areas as mentioned below: 1) Intensive care unit: ICU is a unit with high ratio of medical staff
to patient. Facilities for invasive ventilation and invasive /noninvasive monitoring
are present. As one does not require sedation and paralysis for NIV, it is possible to apply this modality outside the ICU. It is expected that the application of NIV outside the ICU will ease the pressure on ICU beds. Randomized controlled trials have proved the effectiveness of NIV in both ICU and wards.[17] One must remember that these studies were done in units committed to ventilation by noninvasive approach and with required expertise. This factor, more than any other, has been important in determining the outcome. The out come of NIV is remarkably similar in different settings viz. research institutes and peripheral usual care providers.[147] Studies have shown that regardless of the location, the success of NIV is similar between community teaching hospitals and ICUs across Europe.[148] When a well-trained staff is available, it really does not matter. There are only a few prospective randomized controlled studies of NIV outside the ICU.[11],[23],[25],[146],[151] These studies lacked the number, which precluded conclusive inferences. However, in a large study[17] covering 13 centers (n=236), NIV was applied in the general wards by the usual ward staff, using a bilevel device in spontaneous mode, following a simple protocol. The study showed that with NIV treatment failures could be reduced from 27 to 15% ( P < 0.05) and mortality in these patients reduced from 20 to 10% ( P < 0.05). In patients with pH < 7.3, results of initial treatment in the ward was inferior to that of patients treated in the ICUs. It was also demonstrated that early NIV in a general ward resulted in a better outcome than providing no ventilatory support for acidotic patients outside the ICUs. However most of the patients studied were those with acute exacerbation of COPD. The results thus indicated that NIV could be applied with benefit outside the ICU by trained usual ward staff and early introduction of NIV in a general ward results in a better patient outcome. There are no RCTs of NIV outside ICUs in patients with hypoxemic respiratory failure or for weaning. Currently, some data is available from the study of Antonelli et al .[51] Although, theoretically NIV can be applied in the Emergency Department (ED), in India the distinction between ED and ICU fades away in many hospitals. Most patients with an acute exacerbation of COPD coming to ED do not actually need NIV. Those patients who remain acidotic and tachypnoeic after a while after starting standard medication, should be put on NIV in the ED. However, it is imperative that staff trained to initiate and monitor NIV is available in the ED. CPAP has been shown to be of benefit in acute cardiogenic pulmonary edema.[54],[56] in the emergency department. The time spent in emergency ward will vary from hospital to hospital. In some hospitals as soon as the patient is stabilized and bed is arranged, he is shifted to the ward. Others have observation facilities for few hours. NIV can be started in the emergency ward and the patient quickly transferred to a place where mask expertise is available. Success of NIV depends on the initial evaluation and/or the response to a short-term trial. This obviously depends upon the skill of the staff and basic minimal monitoring of parameters to detect early failure.[150] The first few hours are of vital importance and it is mandatory to monitor parameters (SpO 2 , arterial Blood Gases, vital signs, patient comfort, mask leaks and the patients ability to expectorate) by trained personnel, be it a nurse, respiratory therapist or a physician. There is not much information especially in randomized clinical trials in the literature on ′who′should perform NIV. In fact many of the guidelines published have taken for granted the automatic and universal existence of respiratory therapists. In a country like India respiratory therapists are scarce and nurses are not trained in NIV. So for some time to come, it will be the physicians who will take primary responsibility of initiating and monitoring NIV. It is important that the attending staff be able to detect the non-responding patient by frequent clinical examination and persistently abnormal blood gases. They should also be familiar with the equipment, explanation of the procedure to the patient and potential complications of NIV. Nurses, physiotherapists or respiratory therapists may be the caregivers and this will also depend on local availability and enthusiasm and expertise. If a patient has pH < 7.3, they are better managed in HDU or ICU. Recommendations 1. In acute respiratory
failure, NIV can be provided in many locations in the hospital like in ICU,
high dependency area, respiratory ward or NIV unit, emergency
ward or general ward. However, in India for the time being ICU is the best
place.
8. NIV should be applied in the ward on only those patients who are suffering
from a disease state where the role of NIV has been established.
b. Patients who can protect their airways. c. Requirement of intubation appears unlikely. Trained staff nurse should be available to monitor patient frequently. It is also essential to have good nurse to patient ratio with a minimum of one to four in the ward.
b. Patient suffering from COPD, cardiogenic pulmonary edema, acute respiratory failure in obstructive sleep apnea and mild cases of hypoxemic respiratory failure. c. PH < 7.3 but more than 7.2. Those patients who have a greater likelihood of failure should always be ventilated in the ICU i.e., pneumonia, ARDS and asthma. Starting NIV Service (156) NIV services can be started if the following conditions are fulfilled.1. Availability of necessary equipment. A simple pressure targeted machine would be ideal. 2. There should be supply of range of nasal and facemasks and tubes. 3. Facility for cleaning and disinfecting mask and tubing should be available. 4. Trained staff with basic knowledge of NIV, masks and ventilatory circuit should be available. They should know how to adjust setting, how to manage leaks and minor problems including cleaning and disinfecting . 5. Nurses with previous experience in the ICU / NIV are useful. 6. One physician trained in NIV should be available on call 24 hours a day. Management of Copd with Limited Resources COPD, the 12th most common disease worldwide, is a major cause of mortality and morbidity. The 2002 WHO world health report lists it as the fifth leading cause of death in the world.[155] It is expected that by 2020, COPD will become the third most common cause of death.[156] The burden of COPD is high in developing countries. The morbidity data greatly underestimates the true prevalence of the disease due to under reporting. The median values of prevalence rates of COPD in India have been estimated to be 5% in males and 2.7% in females. In 1996 the total number of adult patients more than 30 years of age was estimated to be 8.16 million males and 4.21 million females.[157] The comparatively higher prevalence rates of COPD in women in developing countries is due to a high exposure to indoor particulate air pollution caused by cooking with biomass fuels in poorly ventilated dwellings. Thus we face a large, often underestimated, burden of COPD, which is predicted to assume epidemic proportions in the next decade. Patients with COPD are prone to exacerbations as their disease progresses. Exacerbations in COPD are associated with significant morbidity and mortality. In a large study, connors and colleagues studied more than 1000 patients admitted to hospital with severe hypercapnic exacerbations of COPD. Half of these patients had to be admitted to the ICU, with 35% of them needing mechanical ventilation. Hospital mortality was 11%.[158] Seneff et al have also demonstrated a high in-hospital mortality of 24% in COPD patients admitted to the ICU.[159] In our country, a large number of patients with COPD die due to a lack of management facilities when they present in acute exacerbations with hypercapnic respiratory failure. These patients cannot on most occasions be shifted to a well equipped centre as facilities for invasive ventilation are few and the numbers of ICU beds are far less than needed.[160] There is, therefore, a pressing need for simple, inexpensive but effective therapeutic interventions for treating critically ill patients even in centers where ICUs are not available.[161] NIV reduces the need for intubation, risk of treatment failure, length of hospital stay and mortality in these patients. Although earlier studies of NIV in COPD patients have been reported in an ICU setting, there is now enough evidence that NIV can be initiated even in general wards with simple ventilators. In a landmark prospective multicentric study in patients of COPD in 14 centers in UK, Plant et al demonstrated that the need for intubation was reduced from 27 to 15% by NIV in general wards and hospital mortality was reduced from 20 to 10%. The ward staff with little or no previous experience was able to administer NIV after training. NIV was administered with an unsophisticated ventilator and only the levels of inspiratory and expiratory pressures were adjusted according to a simple protocol. A study of ward based NIV for acute exacerbations of COPD confirmed that it is a highly cost-effective treatment.[102] This data suggests that non-invasive ventilation in wards can avoid admissions to intensive care units and reduce both costs and deaths, especially in developing countries. In a survey of NIV in patients with acute exacerbations of COPD in UK, about 20% centers used clinical guidelines without ABG to select patients for treatment with NIV, These included exhaustion and failure to improve on standard treatment.[162] In a study, Plant et al[163] have estimated that 46.7% patients admitted to a district general hospital in UK were hypercapnic and 20% had respiratory acidosis (pH < 7.35).[12] On the basis of this data, a typical district general hospital in UK (population served 250 000) will admit 90 patients requiring NIV per year. No such data is available in our country and hence an accurate assessment cannot be made for the need for NIV in COPD patients. There was however a consensus in the panel that the number of patients deserving treatment is large with a wide demand supply gap. The skills required for NIV are easily learnt and the equipment required is relatively inexpensive. The complication rate is very low when compared to invasive ventilation. Physicians and nurses can use NIV early outside the ICU to prevent deterioration in the patient′s condition as NIV can be started at an early stage in the evolution of respiratory failure. Reversing respiratory failure is likely to be easier at an early stage when, theoretically, lower pressures used for shorter periods may improve the physiological disturbances. NIV in general wards, thus appears to be a suitable treatment modality for low-income countries because of the limited availability of ICU facilities. The expert panel therefore believes that there is evidence to support the use of NIV in acute exacerbations of COPD even in smaller centers without ICU facilities. Another significant question raised by some members and the international reviewer was whether or not NIV can be administered in selected COPD patients with acute exacerbations in the absence of facility for ABG. Equipment for NIV and oxymetry is much easier to install and maintain than a blood gas testing facility. The expert panel believes that this simple and inexpensive modality should be tried in selected patients even in the absence of blood gas testing facility or ICU, if well trained staff is available. At present such patients get only medical treatment and many of them die due to unavailability of any ventilatory support. Of course it may lead to overuse of NIV but it will save many lives. Recommendations 1. "NIV can be used if the arterial blood
gases report of a patient with acute exacerbation of COPD shows a pH< 7.35
with a paCO2> 45 mm Hg, even if facilities for invasive ventilation are not
available" (level
III)
b) Use of accessory muscles with paradoxical chest and abdominal movements or onset of new physical signs-cyanosis, peripheral edema or mild confusion, lethargy or alteration in sensorium. c) Appearance of signs of hypercapnia-peripheral venous dilatation, tachycardia despite optimal oxygen saturation, bounding pulse with wide pulse pressure, asterixis (flaps), throbbing headaches. d) Persistent or worsening hypoxemia despite supplemental oxygen. e) Significant co-morbid disease-cardiac, uncontrolled diabetes etc. 3. In circumstances of NIV application in the absence of ABG facilities or invasive ventilatory support and ICU care physicians must educate themselves on the signs of failure of NIV support and refer patients to a higher level of care if feasible after 4 hours of trial. (Level III) Practice Points In addition to trained staff, the following minimum equipment should be available before NIV service can be initiated:
Areas where we Need Research We need research in certain areas like maintenance and disinfection of masks and comparison of various masks and their cost effectiveness. In addition, we need epidemiological studies on Noninvasive ventilation practices in India. There is urgent need to develop and validate indigenous masks and ventilator systems to decrease the cost of this modality.Acknowledgment We are thankful to Dr. Laurent Brochard who not only reviewed but also has been actively involved in the making of these NIV guidelines and Dr. Kaushal Pant who helped in editing the final draft. We are also thankful to Dr. Nicholas Hill for reviewing these guidelines. Funding: ISCCM sponsored the air ticket for all the guidelines committee members to attend the meetings. Conflict of interest: None References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06019t3.jpg] [cm06019t4.jpg] [cm06019t1.jpg] [cm06019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}