 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
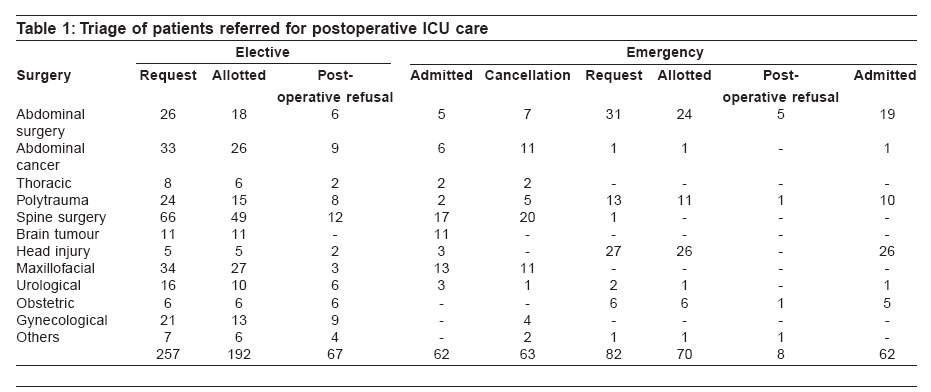
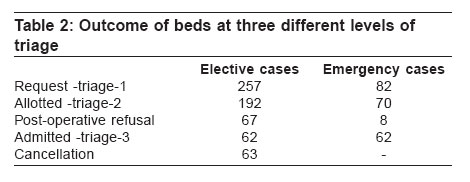
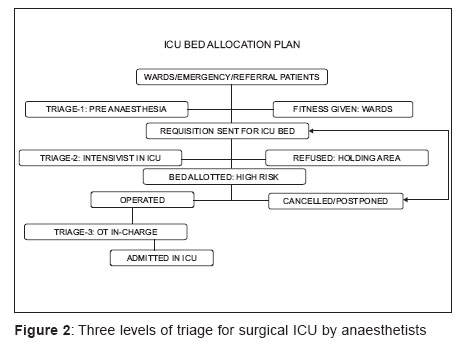
Indian Journal of Critical Care Medicine, Vol. 10, No. 3, July-September, 2006, pp. 167-170 Research Article Triage for surgical ICU: Anesthesiologist and intensivist as gatekeepers to ICU Shanker J, Ghorpode A, Upasani CB Critical Care Unit, Department of Anaesthesia and Critical Care, Grant Medical College and Sir J. J. Group of Hospitals, Byculla, Mumbai - 400 008 Correspondence Address:1362/154, Sector No-4, CGS Colony, Antophill, Mumbai - 400037 Email: jaidoc2003anesth@yahoo.co.in Code Number: cm06021 Abstract Background: The demand for critical care beds among the medical services has already exceeded its supply. Thus allocating intensive care unit (ICU) beds to emergency cases is even more difficult task after doing triage for high risk scheduled elective cases as they fulfill the threshold for post operative intensive care. Keywords: Post operative ICU care, surgical ICU, triage Intensive care unit (ICU) patients are heterogeneous groups with severe illness, multiple system dysfunction and co-existing medical problems. In such situation, which are the best approaches to organize and administer ICU beds within single health care institution? What criteria should be used to fairly select patients for ICU admission? Referrals of patients to surgical ICU are either emergencies or pre-booked elective high risk cases. If more beds were devoted to pre-booked elective high risk patients then fewer beds would be available for emergency cases and vice-versa. Our medical system always finds difficulty in refusal and rationing to beds while utilizing available resources, although ideally in a tertiary hospital, surgical ICU should be able to accommodate all referral trauma and emergency surgical patient.[1] There is an increasing role for intensivists and anaesthetists as gatekeepers to ICU, expectedly refusing admission to a patient due to resource constraints and where there is no potential benefit.[2] The process of triage and rationing decision has important implications for clinicians, patients, researcher, health policy maker and our society. Materials and Methods Design Retrospective observational study. Setting Level-3 surgical ICU with 7 beds including 2 isolation beds over 6 months. Every bed has multi-channel monitoring system along with ventilator. ICU has a back up of round the clock on floor lab services, Arterial Blood Gas and portable X-ray. We undertook an audit for all consecutively admitted postoperative ICU patients in emergency and elective situations. There were more elective cases than the available ICU beds. This made our ICU team to redefine our admission and refusal policies namely "triage for ICU". Providing at least one bed for postoperative emergency patient on daily basis was a part of our individual institutional practices. They were studied in two groups of pre-booked elective versus emergency cases. Admission criteria Depending on severity of pre existing illness and predicted outcome of disease the triage was done for all cases at three levels [Figure - 1]. Those requiring postoperative ventilatory and/or ionotropic support were allotted beds. Emergency cases were dealt with priority by keeping one extra bed per day. Admissions were given on first come, first served basis. Exclusions Cardiovascular and paediatric postoperative surgical cases were excluded as they were managed by other ICUs. Some patients were not referred because hospital staff knew that ICU was running to its maximum capacity. These patients may have got omitted from this retrospective study, which leads to further biases and cannot be eliminated in this study. Refusals Cases of terminal illnesses, advanced carcinoma for palliative or debulking surgeries and moribund ASA-V patients were refused. Beds were not allotted due to shortage of beds i.e., full occupancy or due to equipment failure. ICU triage plan Bed requisitions were received under two settings of pre-booked elective and emergency. Triage-1 First level of triage was done during preanaesthetic check-up and these high risk patients were further evaluated. Requisition forms in prescribed proforma were sent for level 2 triage, a day prior to surgery in all pre-booked elective cases. Triage-2 Urgency, refusals or appropriateness for admission was reassessed on prescribed proforma at second level triage by ICU in-charge. The subjective assessment of their appropriateness was also done by telephone in all such cases with respective operating surgical team. Final confirmation of availability of beds was done on the morning of surgery by ICU team. Pre-booked elective cases also got cancelled or postponed. Triage-3 The triage was done for all operated patients in OT or recovery room by OT anaesthetist in consultation with operating surgical team and stable patients were sent to wards. Statistical analysis Pearson's Chi square was used as test of significance for this comparative study. ' P ' value of < 0.05 was deemed significant. Finally, comparative study was done for elective and emergency bed allocation at all such three levels of triage. Results Total of 339 patients were referred. Pre operative anaesthetist did 257 elective and 82 emergency case referrals after level-1 triage [Table 1]. Out of these, 124 admissions met the criteria for postoperative ICU care with 62 (24%) in elective and 62 (76%) in emergency situations at the end of level-3 triage Table 2. The largest group was that of 66 elective spine surgery requisitions after triage-1. But, 49 requisitions were confirmed for bed allocation after triage-2. Among these 29 got operated, but only 17 met the criteria of post operative ICU care after triage-3. The elective neurosurgical cases were taken for surgery only when vacant beds were available and confirmed pre-operatively. Communication on phone pre-operatively to triage person made 11 beds available for elective neurosurgical cases at level-2 triage. Emergency craniotomy cases for head injury got allotment of beds at 26 times out of 27 and all of them were admitted for elective ventilation. All 12 elective and emergency Obstetric cases were allotted ICU beds and were dealt with priority at level-2 triage. We could allot 24 beds as against a total of 31 emergency requisitions of abdominal postoperative cases at level-2 triage. Emergency abdominal postoperative cases had high mortality as against emergency trauma patients in our study. Eleven out of 13 polytrauma cases got the beds in emergency situations. Triage at level-2 by intensivist made total of 85.4% emergency cases for bed allocation as compared to 74.7% of bed allocation in elective cases. P - value of 0.0449 was statistically significant for emergency cases. At the same time, triage at level 3 by OT in-charge anaesthetist for those who did not meet the criteria for post operative need of ICU care, spared allotted beds upto 11.4% for emergency cases as compared to 51.2% cases for post operative care in elective cases. P - value of 0.0179 ´10 -6sub was statistically highly significant for emergency cases. Due to multiple reasons 32.3% of cases were postponed. These included overcautious advance booking of elective cases, postponement due to lack of OT times, blood stock and many other resources. Discussion The concept of resource allocation on the ground of relative medical benefit is often referred to triage, the process in medical science of finding the most appropriate dispositions for a patient based on an assessment of the patients illness, probable outcome and its urgency. Whereas, rationing by a medical expert is the withholding of medically beneficial services because it costs someone other than the patients.[3] Thus health care resources allocation compasses rationing and triage. These are not singular events but rather complex and multifaceted processes. While doing triage the following points were considered.[4] First of all, patients were allotted beds on first come first served basis. Those with greater potential benefits got priority in terms of triage. Again, all did not receive same level of monitoring. But depending on the severity of illness, appropriate patients received invasive arterial and central venous pressure monitoring. Different thresholds for admission and refusal existed and were different at different times of bed availability. All repeated requisitions in elective surgical cases got priority for allotting the ICU beds for the next time Figure 2. Admitted patients were not discharged prematurely to create a bed for a new admission. Refusal of terminally ill patients helped the ICU staff to cope up with tremendous work pressure resulting from the burden of providing inappropriate care to dying patients and at the same time those of resource implications. But refusals due to unavailability of beds were reasonably cared for at places like emergency wards, OT recovery rooms and casualty. Similar audited result may be useful for future research and policy making. Conclusions Individual institutional practice of providing at least one emergency bed on daily basis against triage of elective cases was helpful for allotting beds for emergency cases. All cases should he triaged and beds should be made available for patients with disorders from which they are likely to recover.[5] More number of cancellations of pre-booked surgery shows that ICU bed non-availability is not the only reason in postponement of surgeries. Further research is warranted to access the merit of telephonic triage and out of ICU assessment. Higher quality studies are needed to address how ICU rationing and ICU triage decisions could be made. Similar systemic and well planned study will play a role model to provide valuable inputs in providing quality care for more patients through better targeted and more efficient services. However the impact of ICU bed rationings on patient outcome remains uncertain. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06021t2.jpg] [cm06021t1.jpg] [cm06021f2.jpg] [cm06021f1.jpg] |
| |||||||||

![[Figure - 1]](/showimage?cm/photo/cm06021f1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}