 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
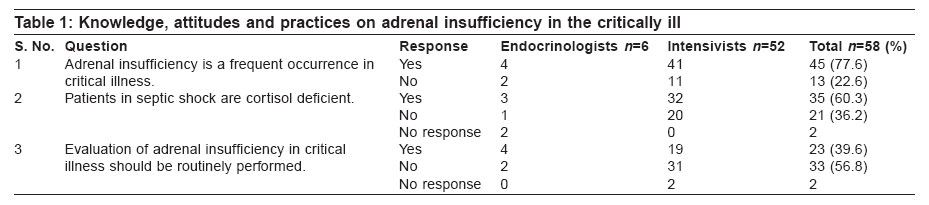
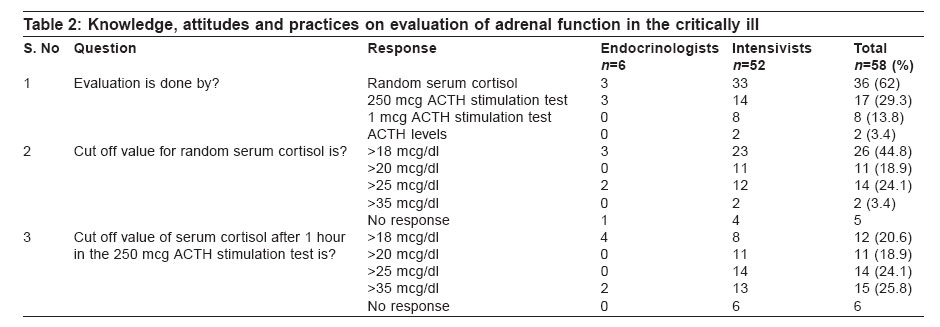
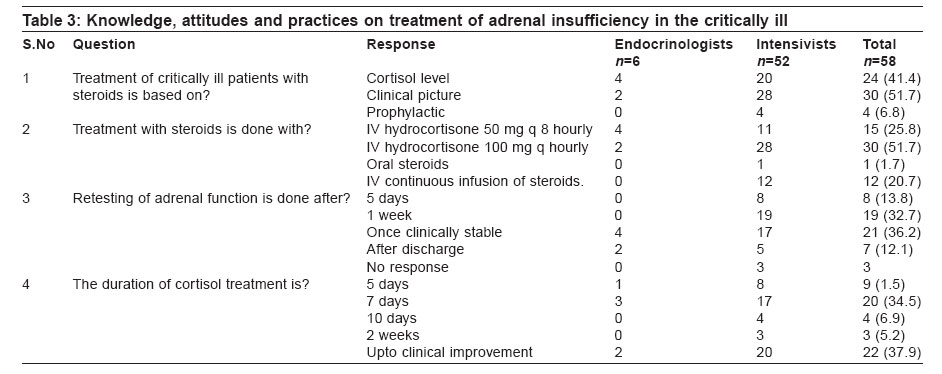
Indian Journal of Critical Care Medicine, Vol. 10, No. 3, July-September, 2006, pp. 176-180 Research Article Assessment of knowledge, attitudes and practices about adrenal insufficiency in the critically ill among endocrinologists and intensivists practicing in Chennai Sathya A, Srinivasan B, Parasuraman G, Ravikumar L, Mahadevan S, Sriram U, Gopichandran V Associates in Clinical Endocrinology Education and Research (ACEER), Apollo Specialty Hospital Annexe, Mount Road, Chennai Correspondence Address:Associates in Clinical Endocrinology Education and Research (ACEER), 319, GEO Towers III Floor, Apollo Specialty Hospital Annexe, Mount Road, Chennai - 600 035 Email: drushasriram@gmail.com Code Number: cm06023 Abstract Background: Adrenal insufficiency is a common occurrence in the critically ill and it is essential that intensivists and endocrinologists involved in the care of these patients have a good understanding of the concepts related to this condition. Objectives: To assess the knowledge, attitudes and practices about adrenal insufficiency in the critically ill among the endocrinologists and intensivists practicing in the city of Chennai. Materials and Methods: Questionnaires containing ten questions pertaining to adrenal insufficiency in the critically ill were sent to a total of six endocrinologists and 52 intensivists practicing in Chennai. Results: About 77% of all the respondents agreed to the fact that adrenal insufficiency is a frequent occurrence in critical illness. But 57% of them felt that there is no need for routine evaluation of critically ill patients for adrenal insufficiency. Random serum cortisol was selected by 62% of the responders as the method for evaluating adrenal function in the critically ill. There is clearly no agreement among the endocrinologists or the intensivists on the various cut off levels for diagnosis. Neither is there a clear consensus on the method followed for treatment of patients with adrenal insufficiency in the critical care unit. Conclusion: There is no concordance in the knowledge, attitudes or practices on adrenal insufficiency in the critically ill among the endocrinologists and intensivists in Chennai. There is a need for developing standard diagnostic and treatment guidelines and making it available for all the practicing endocrinologists and intensivists. Keywords: Adrenal insufficiency, critically ill, KAP The subject of adrenal insufficiency in the critically ill is of great interest. Research has led to the understanding of the pathophysiology of adrenal insufficiency in critical illness. Its recognition and management has been shown to alter the outcome in the critically ill patient. In this scenario it has become essential that all endocrinologists and intensivists have a clear understanding of the current guidelines for management of the critically ill with adrenal insufficiency. This questionnaire survey was conducted to assess the KAP of endocrinologists and intensivists about adrenal insufficiency in the critically ill. Objectives · To assess the KAP of endocrinologists and intensivists practicing in the Chennai city, about adrenal insufficiency in the critically ill. · To see if there is a common consensus among the endocrinologists and among the intensivists on the various issues regarding adrenal insufficiency in the critically ill. Materials and Methods The issues relating to adrenal insufficiency in the critically ill were considered. Questions were prepared to address each of the following aspects of adrenal insufficiency in the critically ill. · Incidence of adrenal insufficiency in the critically ill · Pathophysiology · Assessment of adrenal function in the critically ill · 250 mcg vs 1 mcg ACTH stimulation test · Treatment of adrenal insufficiency in the critically ill. The questions were totally ten in number. Adequate number of questions was asked to address all these issues; at the same time the number of questions was kept limited to avoid responder disinterest. Questions 1. Adrenal insufficiency is a frequent occurrence in critical illness. True/False 2. Patients in Septic Shock are cortisol deficient. True/False 3. Evaluation of adrenal insufficiency in critical illness should be routinely performed. True/False 4. How is adrenal insufficiency in critical illness evaluated? Random serum cortisol a. 250 mcg ACTH stimulation test b. 1 mcg ACTH stimulation test c. ACTH levels 5. The cut off value for random serum cortisol considered normal is? a. 18 mcg/dl b. 20 mcg/dl c. 25 mcg/dl d. 35 mcg/dl 6. The cut off value of serum cortisol for 250 mcg ACTH stimulation test at 1 h is: a. 18 mcg/dl b. 20 mcg/dl c. 25 mcg/dl d. 35 mcg/dl 7. Treatment of critically ill patients with steroids is based on a. Cortisol levels b. Clinical picture c. Prophylaxis 8. Treatment with steroids is done with: a. IV hydrocortisone 50 mg q 8 hourly b. IV Hydrocortisone 100 mg q hourly c. Oral steroids d. IV continuous infusion of hydrocortisone 9. Retesting of adrenal insufficiency is done after: a. 5 days b. 1 week c. Once clinically stable d. After discharge 10. Duration of cortisol treatment is: a. 5 days b. 7 days c. 10 days d. 2 weeks e. Up to clinical improvement These questions were hand delivered to the endocrinologists and intensivists in the city. They were asked to answer the questionnaires and return them in a week′s time. Endocrinologists were defined as physicians trained in the field of endocrinology either in India or abroad and practicing active endocrinology in the outpatient and inpatient setting. Intensivists were defined as physicians, surgeons or anesthesiologists who were currently involved in taking care of critically ill patients in intensive care units. Some of the questionnaires were also answered by postgraduate students in training in the field of intensive care. A total of six endocrinologists and 52 intensivists answered and returned the questionnaires. Results The results are tabulated in [Table - 1][Table - 2][Table - 3]. Some of the physicians did not answer some questions. The percentage of physicians who did not answer the questions was not very big and so is not likely to bring a big change in the results. About 77% of all the respondents agreed to the fact that adrenal insufficiency is a frequent occurrence in critical illness. But 57% of them felt that there is no need for routine evaluation of critically ill patients for adrenal insufficiency. While most of the endocrinologists felt that adrenal insufficiency should be routinely screened for in the critically ill, the intensivists felt that there was no need for a routine screening protocol. Random serum cortisol was selected by 62% of the responders as the method for evaluating adrenal function in the critically ill. Among the endocrinologists the opinion seems to be split midway between random serum cortisol and 250 mg ACTH stimulation test. There is clearly no agreement among the endocrinologists or the intensivists on the various cut off levels for diagnosis. Neither is there a clear consensus on the method followed for treatment of patients with adrenal insufficiency in the critical care unit. Discussion Relative adrenal insufficiency is a common manifestation in the critically ill. The cortisol levels although very high in absolute sense is relatively insufficient to control the inflammatory response. Important clinical clues for adrenal insufficiency in the critically ill include hemodynamic insufficiency despite adequate crystalloid replacement and ongoing evidence of inflammation without an obvious source.[1],[2],[3] There is a definite correlation between the cortisol levels and the severity of critical illness. It is difficult to assess what level of cortisol is adequate response to stress. Proposed minimal levels of random serum cortisol have ranged from 10 mg/dl to 34 mg/dl, but some studies have described that a cut off of 18 mg/dl best identifies patients with adrenal insufficiency.[6],[7],[8] There is a lot of controversy surrounding the utility of the ACTH stimulation test and the procedure to be adopted for this test in the critically ill patient. Annane et al . (2000)[5] in their landmark paper classified three prognostic groups based on the response to corticotropin stimulation test. One group had cortisol level at baseline greater than 34 mg/dl and peak stimulation with a difference greater than 9 mg/dl and it had a good prognosis. The second group had a baseline cortisol of 34 mg/dl and a peak stimulation difference greater than 9 mg/dl and this group had an intermediate prognosis. The third group had a baseline cortisol greater than 34 mg/dl and a peak stimulation difference < 9 mg/dl and this group had poor prognosis.[9] A threshold of 18 mg/dl of serum cortisol 1 h after ACTH injection has been set as normal adrenal reserve.[10] But this threshold has been challenged and said to be inappropriately low in critically ill patients. Critically ill patients with adequate adrenocortical reserve should raise their cortisol levels much higher than this to about 25 mg/dl. Some studies such as the Abdu, Elhadd, Neary et al study which compared with the 1 and 250 mg ACTH stimulation tests head to head did show some superiority of the 1 mg ACTH stimulation test over the 250 mg ACTH stimulation test, but there is no strong evidence to support one over the other.[11] It has also been argued that the change in cortisol level after stimulation of 9 mg/dl should not be used as the criteria for evaluation adrenal function as it only indicated the adrenal reserve and not the adrenal function. The next facet to be considered in this regard is the treatment of these patients. McKee and Finlay[12] randomized 18 patients with diagnosed adrenal insufficiency to glucocorticoid treatment versus placebo. One of the eight steroid treated patients died compared to nine of the 10 placebo treated patients.[12] Further evidence for benefit of corticosteroid treatment in the critically ill came from Bollaret et al and Briegel et al studies.[13],[14] In these studies although a random serum cortisol was obtained the treatment was not stratified based on the cortisol levels. In the study group there was significant reduction in mortality and morbidity. Annane et al randomized 200 critically ill patients to steroid therapy versus placebo. There was a significant 30% reduction in the mortality among the steroid treatment group.[15] The dose of 100 mg IV 8th hourly was recommended. In a meta analysis conducted by Annane et al . it was shown that long courses of low dose corticosteroids reduced mortality in 28 days in intensive care units and it does not adversely alter the risk of gastro duodenal bleeding, hyperglycemia or super infections.[16] In this background this survey was conducted to assess the level of knowledge of this evidence among the practicing endocrinologists and intensivists and their current practice patterns. What emerges from this survey is the fact that there is no clear consensus among the endocrinologists or the intensivists about adrenal insufficiency in the critically ill. There is a wide variability in their practice patterns. There are several probable reasons for this variability. The first factor, which needs to be looked into is the sample of the physicians who responded to these questionnaires. Only six endocrinologists in the city answered and turned in the questionnaires. The small numbers probably have an effect on the results. Among the intensivists some of them were trained in critical care medicine. Most of them were intensivists in practice with no formal training in intensive care medicine. Some of them were residents and registrars in training. This is probably the reason for the wide variability in the responses. The second factor, which is important, is the lack of consensus meetings and hospital protocol framing committees, which can set standard treatment protocols specific to each hospital. If such systems could exist this would standardize the treatment of patients across the board and it also gives adequate time for the involved physicians to review the topics under consideration. The third important factor is the lack of inter-disciplinary meetings and discussions where the members of different specialties could get together and discuss topics of common interest. This would help to make the practice patters uniform in field such as adrenal insufficiency in critically ill where the treatment could be managed by either the endocrinologists or the intensivists. Conclusion From this study the authors suggest that there is a need to develop standard diagnostic and treatment guidelines for adrenal insufficiency in the critically ill and make it available to the endocrinologists and intensivists so as to evolve a uniform practice pattern. This could be done by organizing interdisciplinary meetings in the hospitals where all specialists could participate and contribute to the formation of the guidelines.Acknowledgements The authors acknowledge the contributions of Mrs. Meena Iyer for her administerial help, Ms. Sripriya Rao and Ms. Uma Kanniappan for their secretarial help and Dr Satish for his help in data collection. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06023t2.jpg] [cm06023t1.jpg] [cm06023t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}