 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
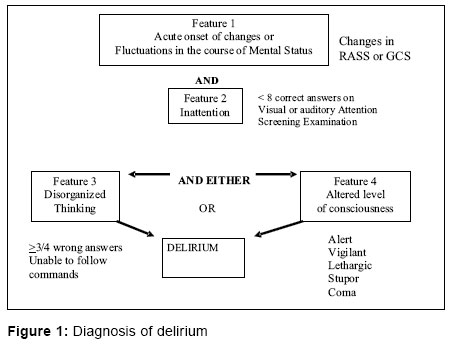
Indian Journal of Critical Care Medicine, Vol. 10, No. 4, October-December, 2006, pp. 215-218 Editorial Delirium in the ICU Divatia JV Department of Anaesthesia, Critical Care and Pain, Tata Memorial Hospital, Mumbai Code Number: cm06029 Delirium is a disturbance of consciousness characterized by acute onset, rapid fluctuations in mental status and impaired cognitive functioning.[1] The patient's ability to receive, process, store and recall information is strikingly impaired. The patient may be agitated or lethargic. It is perhaps better known by its synonyms including intensive care unit (ICU) psychosis, acute confusional state, toxic encephalopathy organic brain syndrome, etc. Delirium is unfortunately often regarded as ICU psychosis or a behavioural disturbance due to the environment in the ICU. However, the mnemonic for the differential diagnosis I WATCH DEATH (Infections, Withdrawal, Acute metabolic encephalopathy, Trauma, central nervous system (CNS) pathology, hypoxia, deficiencies, endocrine disorders, acute vascular insufficiency, toxins and drugs, Heavy metals) is testimony to the fact that delirium may be the symptom of a serious underlying life-threatening disorder.[2] The article by Rudra et al in this issue of the Indian Journal of Critical Care Medicine[3] is timely and important because in reviewing the subject of postoperative delirium, it also draws attention to the larger problem of delirium in critically patients in the intensive care unit. Delirium appears to be an independent risk factor for mortality in ventilated ICU patients. Mortality may exceed twice the six-month mortality rate of nondelirious patients. It may also be associated with longer hospital stay and with a higher rate of cognitive impairment at discharge.[4] It is therefore important to diagnose and manage delirium. However till recently, the diagnosis of delirium in the ICU was imprecise and not standardized, leading to wide variations in the incidence of delirium in various studies and difficulty in interpreting their results. Recently, the confusion assessment method has been refined and validated for use in ICU patients, the CAM-ICU.[5],[6] This can be performed at the bedside and takes less than two minutes. Changes in mental status are best determined using the Richmond Agitation-Sedation Scale (RASS). This is superior to the Glasgow Coma score or other sedation scores as it also includes eye-contact, rather than eye-opening alone, in the assessment.[7] Inattention is determined by responses to the attention screening examination (ASE), in which the patient has to identify cards previously shown to him. Disorganized thinking is detected by answers to four standard questions or inability to follow simple commands.[6] Using the CAM-ICU, Ely et al found delirium to be present in 40% patients who appeared alert or rousable and in 80% of all mechanically ventilated patients.[5] The diagnosis of delirium requires the presence of acute changes or fluctuations in mental status and inattention and either disorganized thinking or altered consciousness, which may range from alert to stupor or coma [Figure - 1]. Thus delirium may be present even in a patient with reduced level of consciousness. While it is easy to suspect and diagnose delirium in patients who are agitated and violent, it is likely to be missed in patients who are mentally obtunded (hypoactive delirium). The CAMS-ICU allows diagnosis of hypoactive delirium. In a study of over 600 ICU patients,[8] a mixed-type delirium involving periods of hypoactivity and withdrawal and occasional periods of restlessness was found to be the most common subtype of delirium. Pure hyperactive delirium was quite uncommon, occurring in fewer than 2% of patients and exclusively in patients younger than 65 years of age. Strictly hypoactive delirium occurred in 45% of patients and was the most frequent type of delirium observed in elderly patient. Mental changes seen in hypoactive delirium may lead to adverse outcomes such as reintubation, with the increased risk of nosocomial pneumonia. In addition, hypoactive delirium is associated with aspiration, pulmonary embolism, decubitus ulcers and other complications related to immobility. On the other hand, hyperactive patients are at risk of self-extubation, pulling out central lines and other catheters, causing self-harm, falling out of bed and also harming caregivers. They are often given higher doses of sedatives that may prolong the duration of mechanical ventilation and leave them in a state of prolonged cognitive dysfunction.[1] Delirium may be thought of as a response of the central nervous system during systemic inflammation.[9] When confronted with systemic inflammation, the central nervous system evokes a cytokine cascade that can affect neuronal activity, resulting in delirium. There is an imbalance between the excitatory dopaminergic neurotransmitter system and the inhibitory GABA and cholinergic system. It is also interesting that acetylcholine inhibits proinflammatory cytokine release. Inhibition of acetylcholine not only causes delirium, as with anticholinergic drugs, but may also trigger an inflammatory response in the CNS. Also, the GABA agonists like benzodiazepines are well known to cause impaired cognitive function leading to confusion and delirium. Sedation with dexmedetomidine, an alpha-agonist, produced much less delirium than propofol or midazolam,[10] both of which are GABA agonists. The article by Rudra et al[3] nicely outlines the risk factors for delirium. These risk factors can be classified as host factors, the acute illness itself and iatrogenic or environmental factors. Most of the risk factors have been described in hospitalized non-ICU patients, but are likely to be applicable to ICU patients as well. Mechanical ventilation increases the risk of delirium three-fold. Increasing age and severity of illness also increase the risk.[8],[11] Use of benzodiazepines, opiates and other psychoactive drugs also significantly increase the risk of delirium.[12],[13],[14] The altered pharmacokinetics of sedatives and analgesics in critically patients, especially the elderly patients, makes the responses to seemingly 'normal' doses difficult to predict.[1] Sedation is one of the commonest interventions in mechanically ventilated ICU patients. Great care must be taken during both, the delivery of sedation and its withdrawal once patients start improving. Sedation must be titrated to a definite end-point, using a sedation scale such as the Ramsay scale or the RASS. Just as we do not give arbitrary doses of vasopressors but titrate them to the blood pressure, sedatives too must be delivered in a titrated fashion. The SCCM recommends that all critically ill patients be monitored for level of sedation and for delirium.[15] The CAM-ICU appears to be useful to in this regard. Despite the fact that ICU patients have multiple risk factors for delirium, it is possible to reduce the incidence and severity of delirium. This includes careful titration of sedation initially and when patients are waking up, facilitating early mobilization, maintaining sleep-awake cycles, ensuring rest, analgesia and comfort and visits by family members.[1] Once delirium is identified in ICU patients, management should focus upon identifying potential precipitating factors, providing supportive care and preventing further complications.[16] Once life-threatening complications such as hypoxemia, hypoperfusion, metabolic derangements, severe pain and infection have been excluded, attention should turn to the patient's medications and environment in an attempt to minimize any factor that might exacerbate delirium.[9] It may also be necessary to counsel family members and provide them reassurance regarding the patient's condition. Pharmacologic therapies to treat the symptoms of delirium should be reserved for patients demonstrating agitation with risk for self-harm, including pulling at catheters or endotracheal tubes and should occur only after nonpharmacologic treatment has been initiated. It is not uncommon to see a combative patient being sedated with a benzodiazepine; this may however make delirium worse. Benzodiazepines are not recommended in the initial management of delirium, except perhaps in alcohol or other withdrawal syndromes. The drug of choice is intravenous haloperidol,[15] a butyrophenone antipsychotic that acts a dopamine receptor antagonist. Despite potential adverse effects, notably prolongation of the QT interval and risk of ventricular arrhythmia, haloperidol is remarkably well-tolerated. It does not depress respiration and produces a mild, variable sedative effect. Extrapyramidal reactions appear to be infrequent with intravenous use. A recent retrospective study[17] suggests that the use of haloperidol in mechanically ventilated patients is associated with reduced hospital mortality, but delirium was not assessed as part of the study. Postulated mechanisms for the observed decrease in mortality include hypotheses that haloperidol may decrease the administration of sedative medication or that it may potentiate central-nervous-system-mediated anti-inflammatory pathways, including the direct inhibition of certain proinflammatory cytokines by haloperidol.[17],[18] The findings of these study are interesting and intriguing. By no means can this be interpreted to mean that haloperidol should be used outside the context of delirium. However it does lay the ground for a randomized trial of haloperidol in delirious and nondelirious patients. The newer antipsychotics risperidone and olanzapine may be helpful, as they affect not only dopamine, but serotonin, acetylcholine and noradrenaline as well. However there is little published literature on these agents. Summary Delirium is an important manifestation of CNS dysfunction in the ICU. Any change in mental status should not be attributed to "ICU psychosis". It is important to recognize the problem, appreciate the seriousness and rule out and treat life-threatening conditions that may result in delirium. Hypoactive delirium is difficult to diagnose, but it may be the initial or sole manifestation of a serious illness, such as sepsis, pneumonia, myocardial infarction or pulmonary embolism, especially in the elderly. Medications are the commonest causes of postoperative delirium. The CAM-ICU is a useful tool in diagnosing and monitoring delirium and should be used frequently in the ICU. Non-pharmacological methods of preventing and treating delirium must be tried and when necessary, hyperactive delirium may be controlled with intravenous haloperidol.References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06029f1.jpg] |
| |||||||||

{kind=link}