 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
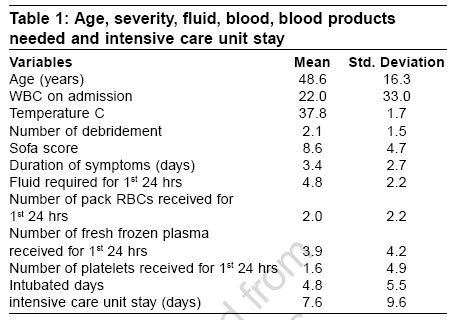
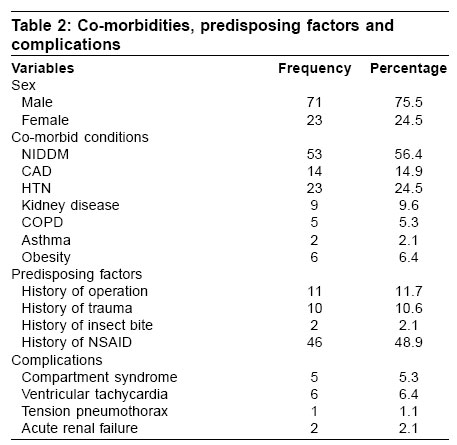
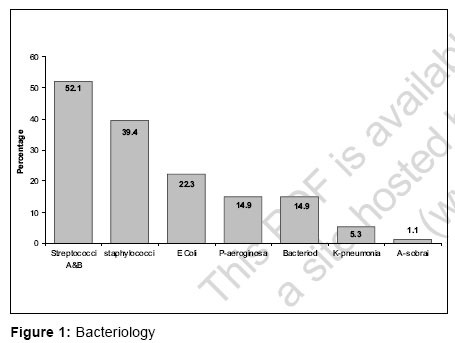
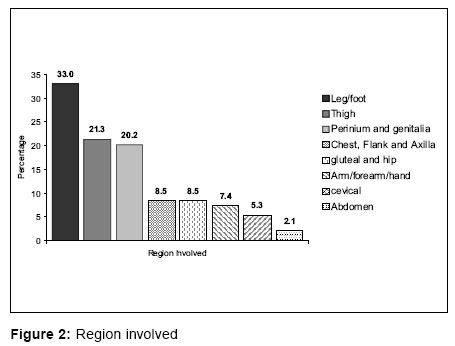
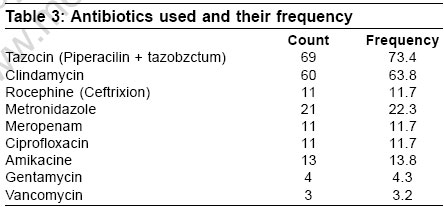
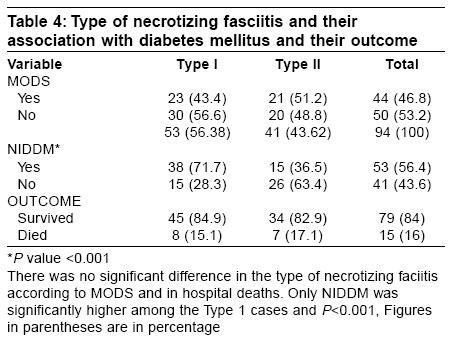
Indian Journal of Critical Care Medicine, Vol. 10, No. 4, October-December, 2006, pp. 225-229 Research Article Necrotizing fasciitis: A decade of surgical intensive care experience Shaikh Nissar Department of Anesthesia, Hamad Medical Corporation, Doha Code Number: cm06031 Abstract Necrotizing fasciitis is a rare disease, potentially limb and life-threatening infection of fascia, subcutaneous tissue with occasionally muscular involvement. Necrotizing faciitis is surgical emergency with high morbidity and mortality.Aim: Aim of this study was to analyze presentation, microbiology, surgical, resuscitative management and outcome of this devastating soft tissue infection. Materials and Methods: The medical records of necrotizing fasciitis patients treated in surgical intensive care unit (SICU) of our hospital from Jan 1995 to Feb 2005 were reviewed retrospectively. Results: Ninety-four patients with necrotizing fasciitis were treated in the surgical intensive care unit during the review period. Necrotizing fasciitis accounted for 1.15% of total admissions to our SICU. The mean age of our patients was 48.6 years, 75.5% of the cases were male. Diabetes mellitus was the most common comorbid disease (56.4%), 24.5% patients had hypertension, 14.9% patients had coronary artery disease, 9.6% had renal disease and 6.4% cases were obese. History of operation (11.7%) was most common predisposing factor in our patients. All patients had leucocytosis at admission to the hospital. Mean duration of symptoms was 3.4 days. Mean number of surgical debridement was 2.1, mean sequential organ failure assessment (SOFA) score at admission to SICU was 8.6, 56.38% cases were type 1 necrotizing fasciitis and 43.61% had type 2 infection. Streptococci were most common bacteria isolated (52.1%), commonest regions of the body affected by necrotizing fasciitis were the leg and the foot. Mean intubated days and intensive care unit (ICU) stay were 4.8 and 7.6 days respectively. Mean fluid, blood, fresh frozen plasma and platelets concentrate received in first 24 hours were 4.8 liters, 2.0 units, 3.9 units and 1.6 units respectively. Most commonly used antibiotics were tazocin and clindamycin. Common complication was ventricular tachycardia (6.4). 46.8% patients had multi organ dysfunction, 15 of them died giving mortality of 16% in this study. Conclusion: Necrotizing fasciitis is more common in males, diabetes mellitus was the most common comorbid disease, type 1-necrotizing fasciitis was more common and the most common regions of the body affected by necrotizing fasciitis were the leg and the foot. Keywords: Foot, leg, necrotizing fasciitis, streptococci, type 1 Necrotizing fasciitis is rapidly spreading and potentially devastating soft tissue infection. It is a progressive infectious process primarily involving fascia and subcutaneous tissue, with thrombosis of cutaneous microcirculation. Necrotizing fasciitis is a life and limb threatening surgical emergency that has been recognized for centuries dating back to Hippocrates in fifth century BC.[1] Wilson first used the term necrotizing fasciitis in 1952 to describe the disease.[2] A variety of terms have been used to describe the same condition including hospital gangrene, progressive bacterial synergistic gangrene, fuornier's gangrene, streptococcal gangrene and flesh eating bacterial infection. Necrotizing fasciitis is an uncommon disease and prognosis hinges on accurate early diagnosis and immediate institution of appropriate treatment. The purpose of present study was to analyze presentation, type of infection, predisposing and comorbid conditions, surgical and resuscitative treatment and outcome of this soft tissue infection. Materials and Methods Our hospital is a 1444 bedded tertiary medical care centre with a 12-bed surgical intensive care unit (SICU). The medical records of necrotizing fasciitis patients treated in SICU between Jan 1995 and Feb 2005 were reviewed retrospectively. Only those patients with histopathology confirming the diagnosis were included in the study. The variables that were examined in the present study includes age, gender, location of necrotizing fasciitis, duration of symptoms, presentation, predisposing factors, comorbid disease, severity of the disease, surgical and initial resuscitation, complications, intensive care unit (ICU) stay and outcome of this surgical emergency. Statistical analyses were performed with use of SPSS statistical software. Bivariate analysis was performed with chi-square test or fisher's exact probability test for comparisons of proportion between groups- P value < 0.05 was considered significant. Results Ninety-four patients with necrotizing fasciitis were treated at our SICU during the period under review, which accounts for 1.15% of total admissions to surgical intensive care unit during the said period. Mean age of our patients was 48.6±16.3 years [Table -1], 75.5% of patients were male. Non insulin dependent diabetes mellitus (NIDDM) was the most common comorbid condition (56.4%), 24.5% patients had hypertension (HTN), 14.9% had coronary artery disease (CAD), 9.6% had kidney disorders, 6.4% were obese, 5.3% had chronic obstructive pulmonary diseases (COPD) and 2.1% of these patients had bronchial asthma (Asthma). The common predisposing factor for necrotizing fasciitis in this study was operative procedure (11.7%), four patients developed necrotizing fasciitis after incision and drainage of abscess, one each after hip surgery, dilatation and curettage, episiotomy, abdominal surgery, above knee amputation, dental extraction and emergency treacheostomy. History of trauma (10.6%) and 2.1% patient had history of insect bite. 48.9% of our patients received nonsteroidal anti inflammatory drugs (NSAID) [Table -2]. All our patients had fever and leucocytosis on admission to the hospital. Mean duration of symptoms was 3.4 ± 2.7 days, number of debridment our patients had was 2.1 ± 1.5 times, Sequential organ failure assessment (SOFA) score at admission to SICU was 8.6 ± 4.7, fluid, packed red blood cell (PRBC), fresh frozen plasma (FFP) and platelet concentrate received were 4.8 ± 2.2 liters, 2.0 ± 2.2 units, 3.9 ± 4.9 units and 1.6 ± 4.9 units respectively in first 24 hours of admission to SICU. The intubated days were 4.8 ± 5.5 days and SICU stay was 7.6 ± 9.6 days [Table -1]. The common bacteria isolated from the necrotic tissue of these patients was streptococci (streptococci pyogenouseandstreptococci agalaectiace) (52.1%) then Staphylococcus aureus (39.4%) E. coli ( Eschercia coli ) 22.3%, Pseudomonas aeroginosa 14.9%, bacteriods 14.9%, Klebsiella pneumonia 5.3% and Aeromonas sobori in 1.1% of the patients [Figure - 1]. The most common region affected by necrotizing fasciitis was the leg and the foot (33%) then the thigh (21.3%), the prenium and the genitalia 20.2%, the chest flank and axilla 8.5%, gluteal and hip 8.5%, arm, forearm and hand 7.5%, cervical 5.3% and the abdomen involved in 2.1% of the patients [Figure - 2]. Eighty two percent patients received two antibiotics while 17% received three antibiotic combination, most commonly used antibiotics were tazocin (piperacilin + tazobactum) and clindamycin [Table -3]. Total 56.38%patients had type 1 necrotizing fasciitis and 43.4% of them multi- organ dysfunction syndrome (MODS) whereas 43.61% patients had type 2 necrotizing fasciitis and 51.2% of these cases had MODS. Type1 infection was significantly higher in diabetic patients. The overall mortality was 16%, in type 1 necrotizing fasciitis the mortality was15.1% while it was 17.1% in type 2 necrotizing fasciitis patients, the difference in mortality was not significant [Table -4]. Discussion Necrotizing fasciitis is a surgical emergency, early diagnosis, prompt and aggressive debridment and definitive therapy in the intensive care environment had been demonstrated to improve outcome of this patients.[3],[4] However since meleney's time, the mortality associated with necrotizing fasciitis remained high, with a reported cumulative mortality of 34% ranging from 6 to76%.[5] The difficulty in making early diagnosis is due to paucity of cutaneous finding in early course of the disease.[6] These patients usually present with triad of symptoms exquisite pain, swelling and fever. If patients received NSAID, these medications will mask the manifestation with the disease still progressing, leading to delay in diagnosis and management.[7] In this study, 48.9% patients had history of receiving NSAID. Necrotizing fasciitis usually had some predisposing factor such as trauma, surgery, scratch or insect bite.[8] In our patients, the most common predisposing factor was surgical procedure. Most of the patients who are affected by necrotizing fasciitis have pre existing condition that renders them susceptible to infections. Conditions that results in immonocompramization in such patients includes advance age, chronic renal failure, peripheral vascular disease, drug abuse and diabetes mellitus.[9] Diabetes mellitus was the common comorbid disease (56.4%) in our patients. In diabetic patients high blood sugar levels is good media for bacterial growth and predisposes to an environment of low oxygen tension and rich in substance for bacterial growth.[10] Necrotizing fasciitis can affect any region in the body, but most commonly effects extremities, perineum and truncal areas of the body.[11] Patients with necrotizing fasciitis present with local signs of infection but severe pain disproportionate to local findings and associated with systemic toxic manifestations.[12] All our patients had leucocytosis and fever at admission to the hospital; leucocytosis is one of the indictor in laboratory risk indicators for necrotizing fasciitis (LRINEC) score for early diagnosis and differentiating necrotizing fasciitis from other soft tissue infections with more then 90% sensitivity and specificity.[13] The new methods of diagnosis are computerized tomography (CT scan) magnetic resonance imaging (MRI) help make an early diagnosis of necrosis. MRI can detect the extent of necrotizing fasciitis and it can identify soft tissue edema infiltrating the facial plans, prior to local gangrenous cutaneous sign of infection, by many hours hence allowing rapid diagnosis and better outcome.[14] But magnetic resonance imaging is not available in many situations and can delay the surgical procedure, secondly it can over- estimate the extent of deep facial involvement as the sensitivity of MRI exceeds its specificity.[15] Other tests are needle biopsy or finger test, which can be performed at the bedside, in the ward.[16] Patients included in our study were admitted to the surgical intensive care unit before or after debridment (mean SOFA score 8.6). The patients with necrotizing fasciitis had large volume of extra cellular fluid sequestrated in edematous wound or have capillary leakage, may have hemolysis and coagulation disorder.[17] These patients may present to the hospital in a toxic shock state necessitating intensive care setup for proper management of these patients. During the first 24 hours of admission to SICU these patient received more then 4.8 ± 2.2 liters of fluid, 2.0 ± 2.2 units PRBC, 3.9 ± 4.2 unit FFP,1.6 ± 4.9 units of platelet concentrate. Prompt and aggressive surgical debridment in corner stone of management of this soft tissue infection, number of debridment in our patients was 2.1 ± 1.5 times. After diagnostic delay, the most common pitfall was inadequate surgical debridment. The debridment should be aimed to remove all necrotic tissue, may be on a daily basis until the local infectious processes has been arrested.[18] Necrotizing fasciitis has been divided into two types on the basis of microbiological culture. Type 1 necrotizing fasciitis is polymicrobial, usually caused by aerobic and anaerobic organism while Type 2 necrotizing fasciitis is caused by streptococci alone or with staphylococci.[19] In our study 56.38% patients had type 1 infection and 43.62% had type 2 necrotizing fasciitis, 71.7% of diabetic patients had type1 necrotizing fasciitis, it learned from literature that type 1 necrotizing fasciitis was common in patients with diabetes mellitus.[20] The toxic shock syndrome is commonly associated with type 2 necrotizing fasciitis and so is the multi organ dysfunction and mortality in these patients.[21] In this study, 46.8% patients went into multi organ dysfunction and 51.2% of type 2 necrotizing fasciitis had MODS. Neutralization of circulating streptococcal toxins by administrating intravenous immunoglobulin is a desirable goal when hypotension present but definitive study and trail is needed to recommend its routine use, hyperbaric oxygen in treatment of this disease also needs clinical trail to justify it use.[22] In our study, most of the patients received two antibiotics and the commonest were tazocin and clindamycin. When necrotizing fasciitis was treated with high doses of penicillin alone, it was less effective than expected, while the initial therapy with combination with protein synthesis inhibiting antibiotics especially clindamycin had a favorable outcome.[23] Importance of use of clindamycin in treatment of necrotizing fasciitis as its use was associated with a reduction in mortality rate in necrotizing fasciitis; clindamycin is known to decrease the production of streptococcal toxins and enzymes even at sub inhibitory concentrations.[24] When treating type1 necrotizing fasciitis aminoglycoside has to be added to the therapy. In this study our patients had a few unusual complication; 6.4% had ventricular tachycardia, 5.3% had compartment syndrome causing acute renal failure and one patient of staphylococcal necrotizing fasciitis had tension penumothorax [Table -1].[25] Overall mortality in our patients was 16%, which is lower, rang mentioned in literature. Conclusion Necrotizing fasciitis was more common in male and diabetic patients. Type 1 necrotizing fasciitis was common in our study and leg and foot was common region affected, overall mortality was lower, there was no significant difference in mortality in type 1 and type 2 necrotizing fasciitis patients.[26]References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06031t4.jpg] [cm06031t1.jpg] [cm06031t2.jpg] [cm06031f2.jpg] [cm06031t3.jpg] [cm06031f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}