 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
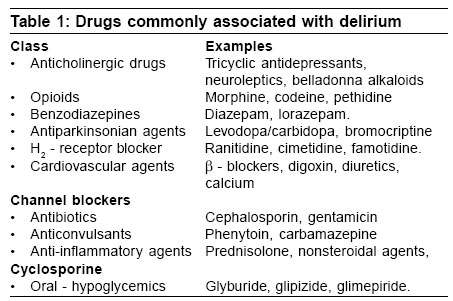
Indian Journal of Critical Care Medicine, Vol. 10, No. 4, October-December, 2006, pp. 235-240 Review Article Postoperative delirium Rudra A, Chatterjee S, Kirtania J, Sengupta S, Moitra G, Sirohia S, Wankhade R, Banerjee S Apollo Gleneagles Hospital, Kolkata Code Number: cm06033 Abstract Postoperative delirium (POD) is frequently under diagnosed and more often than not, under treated. It is the final common manifestation of multiple neurotransmitter abnormalities; with features of impaired cognition, fluctuating consciousness and a disturbed sleep-awake cycle. At least 15% of elderly patients undergoing major procedures have POD, with an associated increase in mortality. Various risk factors and batteries of clinical examination have been devised to diagnose delirium, followed by a multifaceted approach to treatment, using biopsychological along with pharmacological intervention.Keywords: Delirium, postoperative complications Mental impairment following surgery has been a topic of interest for many years. The acute confusional state known as delirium - is one of the most frequently encountered complications observed postoperatively. The word delirium is derived from the Latin term meaning "off the track". Postoperative delirium, a transient mental dysfunction, can result in increased morbidity, delayed functional recovery and prolonged hospital stay in the elderly. The distinguishing features of this transient global disorder are impaired cognition, fluctuating level of consciousness, altered psychomotor activity and a disturbed sleep-wake cycle. It is usually seen on the first or second postoperative day and symptoms are often worse at night. The condition can be silent and go unnoticed or it may be misdiagnosed as depression. The postoperative delirium is defined as clinical situations in which patients think and speak incoherently, are disoriented and show impairment of memory and attention. The mini- mental status examination (MMSE) and other tests can assess speech, consciousness, perception orientation, coherence, memory and motor activity.[1]. The MMSE is easy to conduct, reliable and can be used for serial testing in fluctuating conditions. The mortality associated with delirium is high. Delirium is approximately twice the mortality rate as patients without delirium.[2] Incidence and Etiology The incidence of delirium is approximately 15% in elderly patients after major elective procedures but much higher following cardiac procedures and surgery for hip fractures.[3] The mechanism of delirium is controversial. There is probably no final common pathway to delirium, rather delirium is the final common symptom of multiple neurotransmitter abnormalities. One hypothesis for the mechanism behind postoperative delirium is a decrease in the oxidative metabolism of the brain, which results in the decline of neurotransmitter levels within the brain and causes mental dysfunction. Another hypothesis suggests that an increase of serum cortisol from the stress of surgery or anesthesia may be responsible for postoperative confusion.[4],[5] However another group of workers hypothesized the role of the cholinergic pathways in the pathogenesis of delirium. Production of acetylcholine is decreased in specific medical conditions that precipitate delirium. Serum anticholinergic activity correlates with delirium severity in postoperative patients. Medications with anticholinergic activity frequently can cause confusion in the elderly [Table -1]. Anesthesia Preoperative assessment of the patient's physical and mental status and medications is very important. Preexisting sensory or perceptual deficits compound a patient's chances of developing confusional states.[6] The mainstay of intraoperative preventive measures is maintaining good oxygenation, normal blood pressure, correct drug dosage and normal electrolyte levels. Drug cocktail should be avoided. Atropine, scopolamine and flurazepam should be used only if necessary and the dose should be as low as possible. Glycopyrrolate may be a better choice than atropine as the former is a quarternary amine and should cross the blood-brain barrier less effectively than will atropine. Ambulatory surgery should be encouraged because elderly patients are maintained better in the familiar home environment. Adequate postoperative analgesia, especially in patient who cannot communicate easily because of endotracheal tube or tracheostomy, is crucial. Nurses should be well-versed in detecting the earliest signs of delirium, which in the elderly may be withdrawal rather than agitation. The central nervous depressants, H 2 -anatagenists, anticholinergies, digitalis, phenytoin, lignocaine and aminophylline should be used with discretion. In general, drugs with short elimination half-lives are preferable to long-acting drugs.[7]Associated Dangers Delirium is a common cause of falls, resulting in fractures in old age - and a large proportion of old patients arriving at the emergency department are already delirious on admission. About one third of older patients with hip fractures are usually delirious even before surgery and another third usually develop delirium postoperatively. The longer the waiting time for an operation, the greater the risk that patients will develop delirium.[8] The uncooperative patient in postoperative period may get dehydrated and pull out catheters, drains and tubes. Postoperative delirious patients are prone to fall out of bed and thus, fractures or intracranial bleeding may occur.[5]Diagnosis [9]Patient becomes acutely agitated, uncooperative, confused following surgery and tends to fluctuate during day. Very often, the patient is agitated during the night but calm at daytime. Main features are loss of orientation for time and impairment of attention and memory, whereas hallucinations are less frequent. However, delirium can develop at any time during hospitalization. To assess the patient's degree of cognitive impairment, it is vital to have established a baseline for comparison. Therefore, a good preoperative evaluation should include a formal cognitive assessment in patients at risk of developing delirium. The most severe episodes of delirium usually occur in the evening (sun downing) in conjunction with excessive stimulation and disruption of the sleep-wake cycle. In addition to these criteria, patients with delirium may exhibit visual and auditory hallucinations, anxiety, agitation, altered psychomotor activity. If delirium is suspected during postoperative period, initial focus should focus on the patient's level of consciousness by the assessments of level of orientation and any deficit in memory. Furthermore, conversation may reveal a disorganized thought process or be devoid of any content. Delirium may be identified with the help of formal cognitive tests like, the MMSE,[10] the confusion assessment method (CAM) score[11] [Table -2] and the delirium writing test[11] [Table -3]. Physical examination
Risk factors[12],[13],[14],[15],[16],[17],[18],[19] In all likelihood, patient predisposition, type of surgery and postoperative factors may be more important to the development of delirium than the choice of anesthesia. A painstaking prospective study of the risk factors for postoperative delirium has been carried out.[20] Independent predictors of delirium were:
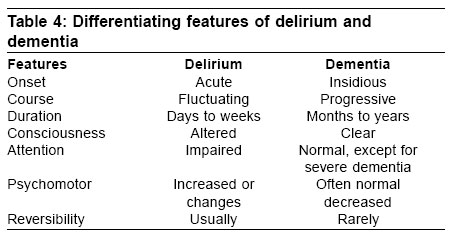
Differentiation from dementia It is important to recognize that patients with dementia are at increased risk for delirium and that delirium and dementia may coexist[26] [Table -4]. Management[27] Delirium is par excellence a disorder requiring a multifaceted biopsychological approach to assessment and treatment and the management strategies include both nonpharmacologic and pharmacologic interventions. Nonpharmacologic intervention Physical interventions Initial intervention includes general measures to support cerebral function, such as intravenous hydration and appropriate nourishment. Supplemental oxygen has been found to be highly effective in patients who developed delirium following thoracotomy for pulmonary malignancy. This intervention may also facilitate recovery in other patients whom oxygenation is not optimal, such as those with postoperative pneumonia. Physical restraints, once a mainstay in the treatment of delirium, are now used only when all pharmacologic and nonpharmacologic interventions have failed. Environmental interventions The hospital environment is a significant factor in the management of delirium. Environmental manipulations are directed toward providing the right amount of stimulation for the patient, encouraging sleep, maximizing the patient's ability to perceive the environment accurately, maintaining safety and achieving familiarity and consistency for the patient. Ove- stimulation should be avoided, because it contributes to both confusion and insomnia. Delirious patients who are left alone without stimulation often withdraw. In such stimulations, regular interaction with hospital staff can be helpful. It is often helpful to place the delirious patient in a room close to the nursing station. Sun downing, a transient worsening of delirium that occurs in the evening hours, is presumably related, at least in part, to decreased stimulation. Hallucinations (visual and auditory) of delirium can be treated by controlled visual stimuli and by music. Adequate daytime lighting and a night light help the patient to perceive the environment accurately. Hearing aids, eyeglasses and other devices that assist sensory perception should be used whenever possible. One of the most helpful interventions is having family members stay with the patient. Cognitive interventions Reorientation is one of the most easily accomplished cognitive interventions. Place a clock and a calendar where the patient can see them easily. The patient should then be verbally reoriented to time and place several times over the course of the day. Repetition is recommended to compensate for memory impairment in the delirious patient. Psychological interventions The delusions expressed by a patient should not be directly disputed. Instead, alternative explanations of events should be offered and frequent reassurance should be given. Educational interventions Staff education on the recognition and treatment of delirium is essential to good delirium management. Staff members who are unfamiliar with the signs and symptoms of delirium may miss the onset of the syndrome Pharmacologic interventions The intent of pharmacotherapy should be specifically to manage an unsafe or significantly disruptive behaviour that is a manifestation of the syndrome; medications are rarely effective in reversing delirium. Haloperdol It has become a popular choice because it has few anticholinergic side-effects, few active metabolites and can be administered orally or parenterally. Haloperidol is superior to benzodiazepines in treating delirium that has been caused by factors other than alcohol withdrawal. The dose of haloperidol is determined by the route of administration, the patient's age, the amount of agitation, the patient's risk of developing side-effects and the therapeutic setting. Low dose haloperidol (1 to 10 mg/day) improves symptoms in most patients. Haloperidol can be administered as a continuous infusion for patients who require frequent dosing. Important side-effects of haloperidol include excessive sedation, hypotension, extrapyramidal symptoms and ventricular dysrhythmia. Benzodiazepines Diazepam and lorazepam are the drugs of choice in alcohol and sedative withdrawal syndromes. Extra-pyramidal side effects of haloperiodol can be prevented by benzodiazepines when used as adjunct. Moreover, benzodiazepine may potentiate the effects of haloperidol, thereby allowing lower doses to be used for patients experiencing undesirable side-effects. Furthermore, haloperidol and benzodiazepine in combination can cause over sedation and life threatening hypotension and respiratory depression. Lorazepam has several advantages owing to its sedative properties, rapid onset and short duration of action. Lower doses are necessary in elderly patients, those with hepatic diseases or those receiving compounds that undergo extensive oxidative metabolism (e.g. cimetidine and isoniazid). The recommended upper limit for intravenous lorazepam is 2 mg every four hours. Giving adequate initial doses reduce the risk of paradoxical excitement. The major advantage of benzoidazepines is that, their effects can be rapidly reversed with flumazenil. A treatment regimen for severe cases requiring prompt, aggressive control of symptoms is outlined below:[28]
Monitor respiratory functions and level of sedation carefully. Consider administering fluma-zenil if there is evidence of significant toxicity. Other pharmacological interventions[29] Following drugs can be used in special circumstances. Opioid: For patients with terminal disease and in those whom pain is an aggravating factor, opioids may provide best palliation. Vitamin B: When vitamin B deficiencies are considered a possible cause, replacement of deficient vitamins is necessary, especially in alcoholics.[30] Physostigmine: It is effective in delirium caused by anticholinergic syndrome.[30] Note : Inspite of all the inteventions mentioned above, if delirium progresses to coma, standard treatment for control of airway, breathing and circulation should be instituted. Summary / Conclusion Fifteen dddpercent of the older patients have delirium at the time of admission to the hospital and another 25% develop the problem during the postoperative period. Patients with underlying dementia are at higher risk of having delirium than those with intact cognition. In addition, dehydration, multiple medications, infections, urinary retention and severe underlying illness may all contribute to the development of delirium. Instruments have been developed that are not only sensitive in diagnosing delirium but also differentiate it from dementia with the delirium rating scale[31] and the confusion assessment method.[32] In general, any change in mental status over baseline should be ascribed to delirium until proven otherwise and a diligent search for its cause pursued because delirium is associated with increased mortality.References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06033t1.jpg] [cm06033t4.jpg] [cm06033t3.jpg] [cm06033t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}