 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
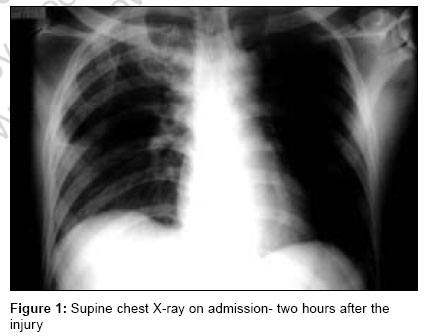
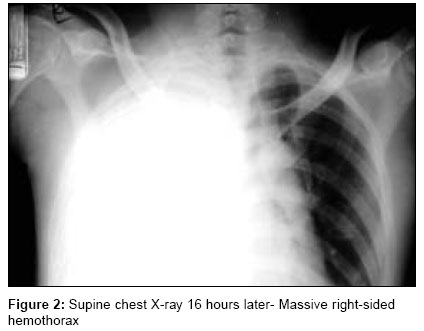
Indian Journal of Critical Care Medicine, Vol. 10, No. 4, October-December, 2006, pp. 254-256 Case Report Delayed life-threatening hemothorax without rib fractures after blunt chest trauma Chinnan NevinKollannoor, Mohamed Shabaan AshrafIbrahim, Palkar SudheerD Department of Anesthesia and ICU, King Khalid Hospital, Najran Code Number: cm06036 Abstract Delayed hemothorax in blunt chest trauma is described as a late presentation of hemothorax after a normal chest X-ray on admission. To detect this clinical entity a repeat chest X-ray is advised after six hours, especially when the first radiograph reveals rib or thoracic vertebral fractures or any significant injury to the thoracic viscera. However, this repeats chest X-ray examination is often not done in patients in whom a significant thoracic trauma has been excluded in the primary and secondary survey. Here, we discuss a case of massive delayed hemothorax after 16 hours of the blunt chest trauma despite a near normal admission chest X-ray and absence of significant chest trauma in the primary and secondary surveys.Keywords: Blunt chest trauma, delayed hemothorax Case Report A middle-aged male driver was transferred from a primary health care center having suffered a road traffic accident two hours ago. On primary survey he was conscious oriented, tachypneic [25/min], tachycardia [110/min] and normotensive [110/70 mm Hg]. He had sustained a fracture of his right femoral shaft. There was no other long bone injury. Examination of chest, abdomen and pelvis were unremarkable except for a few abrasions on the right mammary region. Abdominal ultrasound and pelvic X-rays were normal. Supine chest X-ray [Figure - 1] was near normal except for a slight haziness of the right hemithorax. No fractures or dislocations of the thoracic skeleton or abnormalities of the cardiac silhouette were seen in the admission chest X-ray. During the next two hours, he received intravenous fluids [Ringer lactate 2000 ml] and analgesics [pethidine-100 mg] and was admitted to the surgical ward. Nearly 16 hours after admission, the patient started complaining of chest discomfort associated with a fall in blood pressure to 90/60 mm Hg, low volume pulse and tachycardia [120/ min]. Chest examination revealed diminished air-entry in the right axillary, mammary and infra-mammary regions and a dull note on percussion. Immediate bedside chest X-ray revealed massive right-sided hemothorax [Figure - 2]. Subsequent intercostal tube insertion drained 1700 ml of blood. The patient was hemodynamically resuscitated with another 2000 ml of crystalloids and three units of packed RBCs and taken up for urgent thoracotmy. Intraoperatively, the right internal mammary artery was found to be lacerated and there was a disruption of the second costochondral junction. The patient's postoperative course was uneventful and was discharged seven days after internal fixation of the fracture. Discussion The incidence of delayed hemothorax in blunt chest trauma, as reported by two recent studies ranges from 5-7.4%.[1],[2] In both the studies, all cases of delayed hemothorax had at least one rib fractured on X-ray examination. Most of them were managed by either chest tube drainage or thoracentesis (as far as I am aware, thoracentesis is same as chest drain except a drain may or may not be inserted! However, I find it extra-ordinary that a chest drain is not used in a 'massive haemothorax'! Can the authors please make it clear what they mean by thoracentesis? Some of the delayed hemothoraces in the previous reports were not massive and were reported on follow-up chest X-ray. In some of these patients, the treating physicians chose not to insert chest drain and opted for needle thoracentesis. The usual presentation of delayed hemothorax is worsening pleuritic chest pain and dyspnea in patients with multiple displaced rib fractures, often 18-48 hours after the injury.[3] The possible sources of bleeding in delayed hemothorax could be the lung parenchyma, intercostal vessels, internal mammary artery or the azygous veins.[4],[5],[6] Irrespective of the source of bleeding, the fundamental principles of management are hemodynamic resuscitation, early thoracotmy and surgical control of bleeding if necessary. Our case is unique in that a massive life-threatening hemothorax developed even in the absence of rib fractures. Also, it required thoracotmy to control the bleeding. The admission Chest X-ray taken in supine position (bed side) showed mild haziness of the right hemithorax. This was suspicious, if not conclusive, of a hemothorax. However, an empirical insertion of an intercostal drainage tube at this stage was deferred as the patient was hemodynamically stable and maintained good oxygenation on room air. Moreover, any persistent blood loss into the pleural space would have shown up in the initial chest X-ray (2 hours after the injury) as an opacified hemithorax. An early CT-scan would have probably semi-quantified the underlying hemothorax. But even this would not have contributed much towards the definitive management as the massive hemothorax developed over the next 16 hours. A high degree of clinical suspicion and continued assessment of trauma victims is the only way to diagnose such unusual clinical presentations. "Pubmed" search showed two case reports of delayed hemothorax after blunt trauma without evidence of any rib fractures.[4],[7] One of these also was due to internal mammary artery injury[4] requiring thoracotmy and ligation. A mild haziness of the hemithorax in the supine chest X-ray may be the only sign in a trauma victim suggesting the development of a delayed hemohorax. All such patients may benefit from repeated careful clinical examinations and/or follow-up chest X-ray. Acknowledgements We are indebted to our chief of Anaesthesia and ICU, Dr. Kurnool Shaikh Syed Hussain and to all our colleagues and staff for their support and co-operation.References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06036f2.jpg] [cm06036f1.jpg] |
| |||||||||

{kind=link}
{kind=link}