 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
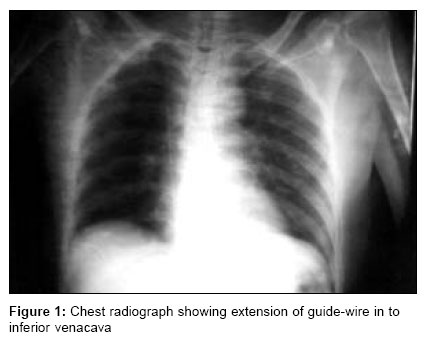
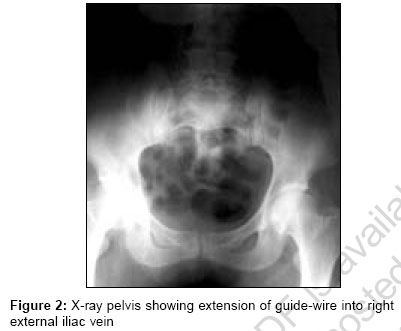
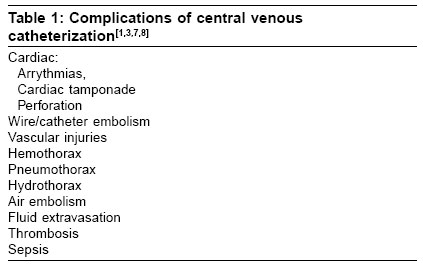
Indian Journal of Critical Care Medicine, Vol. 10, No. 4, October-December, 2006, pp. 257-259 Case Report Guide-wire embolism during subclavian vein catheterization by Seldinger technique Narendra H, Baghavan KR Dr. Narendra H, GCRI, NCH Campus, Asarwa, Ahmedabad Code Number: cm06037 Abstract Percutaneous cannulation of central veins by Seldinger technique is a popular approach in intensive care settings. We report a case of embolization of a complete guide-wire during such a procedure. Our case differs from the few earlier reported cases in that subclavian vein was the entry site. While reviewing the available literature, we discuss few reasons and management of such a mishap.Keywords: Central venous catheterization, complications, guide-wire embolism, seldinger technique Introduction From the time Aubaniac first reported use of central venous catheter in 1952 for hemodynamic monitoring the spectrum of indications have widened. Current indications include inadequate peripheral venous access, central venous pressure monitoring for optimal fluid management, rapid fluid replacement, administration of vasoactive and phlebitic drugs, long-term venous access, hemodialysis, plasmapharesis and total parenteral nutrition.[1],[2],[3] Insertion sites used for percutaneous central venous catheterization (CVC) are internal jugular vein, subclavian vein, femoral vein and peripherally inserted central catheters through cephalic, basilic or saphenous veins. Percutaneous infraclavicular subclavian vein catheterization by Seldinger technique is a popular approach.[1] The technique involves initial needle insertion into the vein, followed by a guide wire to permit passage of a catheter. We report a case wherein during such a procedure the guide-wire was inadvertently pushed into venous system that was surgically extracted from right common iliac vein. Our case differs from the others in that the subclavian vein was cannulated. Most of the times the mishap is immediately recognized, with few exceptions available in literature.[4],[5] Case Report A 64-year-old lady admitted in the intensive care unit of our hospital with a diagnosis of viral encephalitis required a central venous line for the purpose of fluid management. Intensivist decided to cannulate right subclavian vein by percutaneous infraclavicular approach using Seldinger technique. Patient was placed in the Trendelenberg position, part-painted and draped. Initial cannulation was done with needle attached to a syringe directed towards sternal end of opposite clavicle below midclavicular point. Guide-wire was introduced through the needle and needle was withdrawn. Track was dilated with dilator. While threading the catheter over guide-wire, it was inadvertently pushed into the subclavian vein. Immediately procedure was abandoned. A chest radiograph was taken [Figure - 1], which showed guide wire in inferior vena cava. Surgical consultation was sought. Fluoroscopic examination revealed migration of guide-wire to the right external iliac vein [Figure - 2]. We decided to extract the guide-wire by open surgery, as there was no facility for interventional radiological extraction. Patient was heparinised and systemic antibiotics started and guide wire was successfully surgically extracted. Patient recovered well and was discharged.Discussion Clinicians, whose training and experience may vary considerably, perform CVC. The procedure is done in a variety of hospital settings like intensive care units, emergency departments, operation theatres, pre and postoperative wards, hemodialysis units, cardiac catheterization units etc. The frequency of complications associated with percutaneous CVC varies largely due to differences among selected venous entry site, experience of the operator and other risk factors. In general it is around 0.3-12%. Investigators have correlated an increased incidence of complications and insertion failure with operator inexperience.[3],[6] Complications are multiple and are listed in [Table -1]. In the case reported by us above,. While advancing the catheter, proximal end of the guide-wire should have been under the control of operator in order to prevent entire guide-wire entering venous system. Guide-wire migrated from subclavian vein to the right atrium to inferior venacava and landed in external iliac vein just below bifurcation of common iliac vein on the right side. Though it is possible that many such cases are not reported because of their iatrogenic origin and may reflect inexperience of the operator, some reports have been published elsewhere. Schummer et al reported four different cases of loss of guide in different clinical scenario. All cases occurred during percutaneous catheterization of internal jugular vein by Seldinger technique. Those who were inexperienced in the technique performed procedures. They attributed the mishap to inattention, inexperienced operator (either Seldinger technique or actual CVC per se) and inadequate supervision of trainees or over-tired staff.[4] Batra et al . reported guide-wire embolism during internal jugular vein cannulation. They observed that introduction of excessive length of guide-wire during the placement of catheter can result in such problems.[9] Andrews et al fluoroscopically calculated the safe length of guide-wire insertion from venous access site to superior venacava-atrial junction as 18.4 cm for right subclavian vein.[10] Valero et al. described a case in which burn patient suffered embolization of entire guide-wire during replacement of central catheter through Internal jugular vein, which had migrated to iliac fork. It was removed by using percutaneous interventional radiological technique.[8] Duong et al . reported guide- wire migration to inferior venacava through internal jugular vein.[11] In an analysis of central line complications from ASA closed claims project, out of 75 claims related to central lines, 10 accounted for wire or catheter embolism. All of them occurred in the period 1978-89 (10 out of 49 claims) and none after 1990. None of them caused fatalities.[7] Our case differs from the above cited case in that right subclavian vein was cannulated. Complications of leaving guide-wire in-situ are thrombosis, infections (septic thrombophlebitis and endocarditis), post-phlebitic syndrome, pulmonary embolism, arrythmias, cardiac and vascular damage. Most of the times the mishap is immediately recognized, with few exceptions seen in literature.[4],[5] Reynen reported a patient who had a 40 cm guide-wire in his pulmonary vasculature for 14 years, before detection. It was managed without intervention as guide-wire was adherent to vessel wall.[5] In addition to the possibility of losing whole guide-wire, one must also consider the embolization of fragments, which can easily reach pulmonary artery. Majority of them can be removed percutaneously by interventional radiological methods. Various techniques used to extract vascular foreign bodies are loop snares, dormia baskets, hooked or pigtail catheters and endovascular forceps.[4],[5] Transvenous retrieval using angioscopic forceps is recommended mainly for emboli in superior venacava or right atrium.[12] Still conventional surgery has a role especially in centers like ours where such facilities are lacking or when the percutaneous extraction fails.[8] Management of high-risk patients is individualized depending on assessment of operative risk and morbidity and mortality associated with leaving material in-situ . Whenever nonoperative approach is chosen, steps are taken to prevent potential thrombotic and infective complications.[12] In Summary, embolization of entire guide-wire can be due to lack of experience in the insertion technique or due to situation of hemodynamic instability in patients with poor alternate venous access, leading to errors caused by rapid advancement of catheter. Hence recommendations are to perform the procedure by an experienced operator (50 or more insertions)[1] or under supervision, guide-wire not to be pushed too far (Upper limit 18 cm from the insertion site)[10] and while threading the catheter over guide-wire, guide-wire should at all the times be held firmly by other hand. Catheter should be rail-roaded over the guide-wire into the vein and not pushing the catheter and guide- wire together. Whenever complication arises, early recognition and prompt intervention will prevent further morbidity and mortality. References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06037t1.jpg] [cm06037f1.jpg] [cm06037f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}