 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
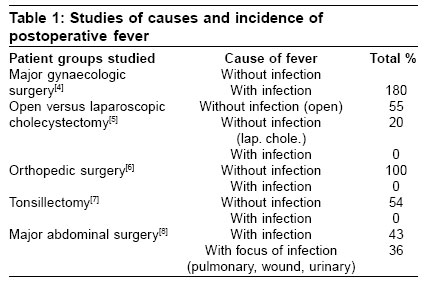
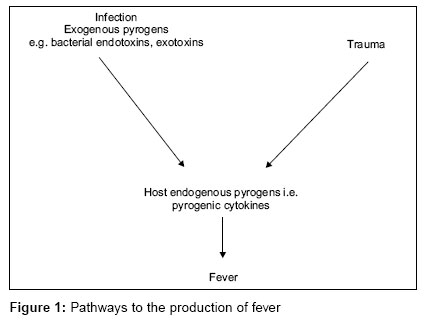
Indian Journal of Critical Care Medicine, Vol. 10, No. 4, October-December, 2006, pp. 264-271 Teaching Aids Postoperative fever Rudra A, Pal S, Acharjee A Department of Anaesthesiology, Calcutta National Medical College, Kolkata - 700 014 Code Number: cm06039 Abstract Postoperative fever is one of the most common problems seen in the postoperative ward. Most cases of fever immediately following surgery are self-limiting. The appearance of postoperative fever is not limited to specific types of surgery. Fever can occur immediately after surgery and seen to be related directly to the operation or may occur sometime after the surgery as a result of an infection at the surgical site or infections that involve organs distant from the surgery. Therefore, during evaluating postoperative fever, it is important to recognize when a wait - and - see approach is appropriate, when further work-up is needed and when immediate action is indicated.Keywords: Postoperative, fever Fever Fever is a rise of the normal core temperature of an individual that exceeds the normal daily variation and occurs in connection with an increase in the hypothalamic set point. According to studies of healthy individuals 18 to 40 years of age, the mean oral temperature is 36.8° ± 0.4°C (98.2° ± 0.7°F) with low levels at 6 am and higher levels between 4 to 6 pm. The maximum oral temperature is 37.2°C (98.9°F) at 6am and 37.7°C (99.9°F) at 4 pm; these values define the 99th percentile for healthy individuals. In light of these studies, an am temperature of greater than 37.2°C (98.9°F) or a pm temperature of greater than 37.7°C (99.9°F) would define a fever. However, there is no coding definition or uniform clinical definition of a significant fever. Temperatures exceeding 38°C (100.4°F) and persisting for more than two postoperative days are generally considered to be clinically significant.[1] Measurement of body temperature Temperature taken orally is about 0.5°C higher than that taken in the axilla or is about 0.5°C below than that taken rectally. Rectal temperature is considered core. The lower oral readings are probably attributable to mouth breathing, which is a particularly important factor in patients with respiratory infections and rapid breathing. Lower oesophageal temperature closely reflects core temperature.[2] Incidence The incidence of postoperative fever is remarkably high. However, published incidence rates range widely (from 14% to 91%)[3] depending on how fever was defined and the patient population of the study. Though fever is common, infection is found as the cause in less than one-half of febrile patients. Studies have determined that the incidence of postoperative fever in patients undergoing various surgical procedures is not a specific marker of infection in those settings [Table -1]. The overall sense from [Table -1] is that, postoperative fever is more likely to be due to the inflammatory response to the trauma of surgery and not a response to the infection. The greater surgical trauma, (e.g., open cholecystectomy versus laparoscopic cholecystectomy) the more likely is postoperative fever to occur without the occurrence of infection. The general consensus of workers in this field is that postoperative infection as a cause of fever after surgery is diagnosed best by specific symptoms and signs attributable to the infection. Although the trauma of surgery and infections are the two most common causes of fever, there are other less common but important causes, including medications, blood transfusion, deep venous thrombosis and pulmonary embolism, myocardial infarction and pancreatitis. Medications are a frequent cause of fever. Probably the most common medications causing fever are antibiotics, which can cause great confusion. Another uncommon but important cause of fever in the postoperative period is alcohol withdrawal. Patients who present with a fever and delirium postoperatively must have alcohol withdrawal in differential diagnosis because appropriate treatment can reduce the significant morbidity and mortality of this clinical problem. It has been classical teaching that pulmonary atelectasis after abdominal surgery is a common cause of postoperative fever. A study conducted to determine the relation of postoperative fever and atelectasis found, however, no relation between atelectasis and fever postoperatively.[9] The daily incidence of atelectasis increased after surgery, whereas the incidence of fever decreased. Pathophysiology Fever may be a transient and trivial sign, which resolves rapidly with no treatment (e.g., the immediate mild fever seen in many postoperative patients). It may, however, be a sign of serious significance presaging the onset of systemic inflammatory response syndrome (SIRS) and multiorgan dysfunction syndrome. Clearly, it is important to be able to identify which patients fall into the former category and which into the later. Infection may cause fever, as part of the inflammatory response of the host to invasion by microorganisms and the production of toxins by these organisms. Gram-negative bacilli have lipopolysaccharides (endotoxins) as structures in the cell wall that act as pyrogens (the term pyrogen is used to describe any substance that causes fever). Gram-positive cocci produce exotoxins, which are excreted from the bacteria and which are pyrogens. The pyrogens produced from either gram-negative or gram-positive bacteria are considered as exogenous pyrogens (i.e., coming from sources other than the host). Exogenous pyrogens stimulate monocytes and macrophages of the infected host to produce substances called pyrogens or pyrogenic cytokines. Pyrogenic cytokines have various effects on stimulating or controlling the inflammatory response and fever. Cytokines act as intercellular mediators and messengers controlling the host response to injury and infection.[10] The pyrogenic or proinflammatory cytokines, interleukin 1 (IL-1), is a primary activator of the febrile response to tissue injury and the local inflammatory response to infection.[11] Trauma, including the trauma associated with surgery, elicits the production of pyrogenic cytokines in the absence of infection. Fever may occur. The production of host endogenous pyrogens or pyrogenic cytokines, is the final common pathway through which fever occurs from such diverse causes as infection and trauma in the absence of infection [Figure - 1]. Normal thermoregulation The control of body temperature depends upon the following components:
Setting of body temperature and detection of core temperature in the preoptic nucleus is done by hypothalamus. Moreover, posterior hypothalamus compares the core and peripheral temperatures with the set temperature. Furthermore, it induces appropriate actions to restore the body temperature to the set temperature. When the body temperature is higher than the set temperature then, the mechanism of heat loss will be controlled by the anterior hypothalamus. However, the posterior hypothalamus controls the mechanisms for heat gain. Elevation of the hypothalamic set point by cytokines[2] During fever, levels of prostaglandin E 2 (PGE 2 ) are elevated in hypothalamic tissue and the third cerebral ventricle. The concentrations of PGE 2 are highest near the circumventricular vascular organs (organum vasculosum of lamina terminalis) - networks of enlarged capillaries surrounding the hypothalamic regulatory centers. Destruction of these organs reduces the ability of pyrogens to produce fever. From the results of the animal studies, it appeared that both exogenous and endogenous pyrogens interact with the endothelium of these capillaries and that this interaction is the first step in initiating fever, i.e. in raising the set point to febrile levels. SIRS and sepsis SIRS is a term applied to the febrile inflammatory process that occurs after surgery. SIRS can have either infectious or noninfectious causes.[12] Sepsis is the term used to describe the systemic inflammatory response resulting from infection.[12] These two terms are used frequently to describe fever occurring after surgery, which may be due solely to cytokine activation from surgery itself or due to an infection complicating surgery. Defense mechanisms of the host, alteration by surgery and increased morbidity caused by infection. Increased incidence of infection after surgery may depend upon the increased production of pro-inflammatory cytokines and other anti-inflammatory cytokines. The greater the trauma associated with the surgical procedure (e.g., open cholecystectomy versus laparoscopic cholecystectomy) it is more likely to activate the cytokine response with subsequent fever and also greater effect is found on the type 1 and type 2 (Th-1, Th-2) helper T lymphocytes. Th-1 cells are involved with cell-mediated immunity and produce IL-2, whereas Th-2 cells are involved with antibody-mediated immunity and produce IL-10.[13] Immune systems and local defense mechanisms are also affected in addition to these systemic effects due to anesthesia and surgery. Evaluating postoperative infection Infection is more likely to be present in a patient with a fever that develops after the first two days following surgery.[14] Most common infections occurring after surgery:
Wound infections The surgical incision interrupts the integrity of the defense mechanism of skin. Surgical wound infection depends on: a) The type of surgery performed (e.g. cholecystectomy versus colon resection) Urinary tract infection More likely to occur in women and in patients who are in need of prolonged catheterization. Postoperative pneumonia A. Mechanically ventilated patients are at high risks because:
B. Age Intravenous catheter- related infections Can be caused either by peripheral catheters (usually leading to thrombophlebitis or cellulitis) or by central catheters (usually causing bloodstream infection). Intra-abdominal infection Prosthesis infection It may manifest within a few days of surgery, especially if it is caused by Staphylococcus aureus. Clinical correlation The timing of fever relative to the postoperative day (POD) will indicate the most likely cause. The five W's of postoperative fever - Wind, Water, Walking, Wound and Wonder drugs - as a useful memory tool could help a physician when he is following patients after surgery.[15],[16] POD 1-2: Wind: Atelectasis (without air) often cause fever. Reasons include being on a ventilator, inadequate sighs during surgery and (in the general surgery patient) incisional pain on deep breathing. This is treated with incentive spirometry because there is evidence that deep inspiration prevents atelectasis better than just coughing . POD 3-5: Water: Urinary tract infections (UTIs) are common here. Foley catheters are sometimes still in place. POD 4-6: Walking: Deep venous thrombosis can occur. This is more of a problem in patients undergoing pelvic orthopedic or general surgery than in head and neck surgery. Subcutaneous low dose heparin and venous compression devices reduce the incidence of thromboembolization . Walking the patient on POD1 is the best way to prevent this complication. POD 5-7: Wound : Most wound infections occur during this period. Preoperative antibiotics are important to prevent or reduce the risk of infection in head and neck surgery that crosses mucosal linings. POD 7+: Wonder drugs : Drugs can cause fevers.(Note that in obstetrics and gynaecology, this W is "womb" and it precedes "Wonder drugs"). Noninfectious causes must be considered with infectious causes in the postoperative patient because fever resulting from infection and trauma (i.e., surgery) are produced through the release of similar cytokines. However, fever in patients without evidence of infection occurred closer to the surgical procedure and lasted for a shorter time than did fever resulting from infection. Therefore, empiric antibiotic therapy may not be necessary in these cases, when the fevers are not associated with infections. Assessment of The Pyrexial Patient [2],[17]Fever should never be ignored. Appropriate evaluation of early postoperative fever includes a careful history, a targeted physical examination and additional studies if indicated. Preoperative course Details of the period before hospitalization can be critical. For example, a patient with a hip fracture may have fallen because of an occult urinary tract infection, pneumonia or cardiac arrhythmia. Details of the procedure Duration of surgery, blood products administered and any complications may be important. Nursing information Often important, such as if the patient has diarrhea or is coughing. History
Physical examination A meticulous physical examination should be done on a regular basis. All the vital signs are relevant. The temperature may be taken orally or rectally, but the site used should be consistent. A careful search for the infective cause should be made :
Investigation The tempo and complexity of the workup will depend on the pace of the illness, diagnostic considerations and the immune status of the host. Infective causes of pyrexia should be differentiated from non-infective causes by the history and clinical examinations. However, presence of a noninfective cause does not necessarily exclude an infective cause, e.g. patients with alcohol withdrawal may also have pneumonia. Identification of a causative organism and its antibiotic sensitivities should always be attempted. It is important to sample if possible before starting antibiotics to prevent interference with the culture. Bacteriological assessment Includes blood culture, sputum, pleural or peritoneal aspirate, urine, skin and wound swab of discharge or needle aspiration, stool, cerebrospinal fluid (by lumbar puncture), intravascular catheters, aspiration of tissue fluid from spreading edge of cellulitis, should be cultured on removal. Hematological tests In the presence of infection, polymorphonuclear leucocyte count is usually raised. However, in severe infections or in the immunosuppressed or malnourished patient, the leucocyte count may be normal or reduced. Platelet count is usually elevated as part of the normal response to stress. However, it may be markedly reduced if disseminated intravascular coagulation has developed. In the later stages of infection or when the patient is resuscitated with a large volume of colloid, there will be reduced hemoglobin concentration. Coagulation screen is essential for patients with severe sepsis and immunological tests are required in the patients with transfusion reactions. Serum biochemistry
ECG and Echo cardiography For the assessments of myocardial ischaemia, mechanical anomalies of cardiac function and the presence of intracardiac thrombosis. Outcome of diagnostic efforts In most cases of fever, either the patient recovers spontaneously or the history, physical examination and initial screening laboratory studies lead to a diagnosis. When fever continues for two to three weeks, during which time, repeat physical examinations and laboratory tests are unrevealing, the patient is provisionally diagnosed as having fever of unknown origin. Usefulness and cost-effectiveness of routine work-up[19] Majority of fever work-ups were of low clinical yield and added moderate cost. Significant infection is associated with surgery for malignancy, bowel resection, number of febrile days, higher fever and moderately increased white blood cell count. Only patients with these characteristics are most likely to benefit from laboratory and/or radiographic workup of fever. Treatment Treatment of the noninfective cause of pyrexia The routine use of antipyretics given automatically as "standing", "routine" or "prn" orders to treat low-grade fevers in adult patients is entirely unacceptable. This practice masks not only fever but also other important clinical indicators of a patient's course. The objectives in treating fever are :
Antipyretics Aspirin and paracetamol interfere with the production of prostaglandins via the inhibition of cyclo-oxygenase. Prostaglandin is the central messenger in the production of pyrexia, which help to lower the hypothalamic set point. However, antipyretics are indicated if the patient's temperature approaches more than 39°C. Reducing fever with antipyretics also reduces systemic symptoms of headache, myalgias and arthralgias.[2] Oral aspirin and nonsteroidal antiinflammatory drugs (NSAIDS) effectively reduce fever but can adversely affect platelets and gastrointestinal tract.[20] Therefore, paracetamol is preferred to all of these agents as an antipyretic. In children, paracetamol must be used because aspirin increases the risk of Reye's syndrome. If the patient cannot take oral antipyretics, parenteral preparations of NSAIDs and rectal suppository preparations of various antipyretics can be used.[2] Approach to the treatment of infection as the cause of postoperative fever The treatment of infection in surgical patients can be described as under:
Antibiotics The appropriate antibiotic for the sensitives of the cultured organisms should be used. However, in the absence of bacteriological information therapy should be given on a 'best guess' basis. The dose of antibiotic depends on age, weight, renal function, allergies and severity of infection as well as toxicity of the antibiotic. Life-threatening infections require intravenous therapy. The duration of therapy should be long enough to cure the infection but should not be unduly prolonged to prevent the risk of developments of resistant organisms. Fluid resuscitation[21] Hypovolaemia is an early feature of developing septic shock and SIRS bacteraemia. Vigorous fluid replacement may abort the progress to the 'cold' shock. Therefore, expansion of plasma volume is required with the usage of gelatine solutions or starch solutions in addition to crystalloid. Ionotropes and vasoactive agents Systemic infections may have a myocardial depressant effect. Thus, ionotropic support may be required with adrenaline, dobutamine or dopexamine. Dopamine may be indicated to produce renal vasodilatation in cases of diminished renal function. Respiratory support Seriously ill, infected patients have deranged gas exchange and require oxygen therapy. Surgical therapy Elimination of a source of infection is one of the main principles of the management of surgical infections.
Summary Postoperative fever should alert the caregiver to the possibility of an infection complicating the recovery of the patient, but the presence of fever is not a reliable indicator of the presence of infection and the absence of fever does not guarantee that the postoperative patient is infection-free. The outcome for a patient with postoperative fever is dependent on the cause. Therefore, postoperative fever should be evaluated with a focused approach rather than in "shotgun" fashion. Noninfective causes generally have a better outlook than infective causes. The outcome for the infected patient is dependent on the rapid identification of the cause, appropriate resuscitation, antibiotic treatment and appropriate surgery to eliminate the source. For pediatric oncology patients who are often immunocompromized, a postoperative fever may indicate an infection, which can lead to significant complications if not treated promptly. Although a full septic work-up may be unnecessary, additional investigations such as blood cultures may be warranted and an antibiotic therapy should be considered for some or all febrile postoperative cancer patients.[22] References
Copyright 2006 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm06039t1.jpg] [cm06039f1.jpg] |
| |||||||||

{kind=link}
{kind=link}