
|
Indian Journal of Critical Care Medicine
Medknow Publications on behalf of the Indian Society of Critical Care Medicine
ISSN: 0972-5229 EISSN: 1998-359x
Vol. 11, Num. 3, 2007, pp. 127-138
|
Indian Journal of Critical Care Medicine, Vol. 11, No. 3, July-September, 2007, pp. 127-138
Review Article
The role of selenium in critical illness: Basic science and clinical implications
Salama Alaa, Sakr Yasser, Reinhart Konrad
Department of Anesthesiology and Intensive Care, Friedrich-Schiller-University Hospital, Jena
Correspondence Address:Dr. Konrad Reinhart, Department of Anesthesiology and Intensive Care,
Friedrich-Schiller-University, Erlanger Allee 103, 07743 Jena, Germany.
E-mail: konrad.reinhart@med.uni-jena.de
Code Number: cm07024
Abstract Over the last century, our understanding of selenium has progressed considerably and we have come to recognize it as an essential component or cofactor of enzymes throughout metabolism, such as glutathione peroxidase (GPx), thioredoxine reductase and iodine deiodinase. GPx acts against hydrogen peroxide and lipid peroxidation and is an important line of defense against free radicals; thioredoxine reductase is involved in nucleus redox status; and iodine deiodinase is involved in thyroid hormone metabolism, which is frequently impaired in critically ill patients. Selenium also has an anticarcinogenic effect that is thought to be induced by the production of methyselenol, a selenometabolite that affects gene expression and modifies cell cycling and immune function. We review current knowledge concerning clinically relevant selenoproteins, discuss the potential role of these compounds in health and disease, review the epidemiology of selenium deficiency and its clinical implications with a special emphasis on critically ill patients and discuss the role of selenium supplementation in critical care settings.
Keywords: Organ dysfunction, reactive oxygen species, sepsis, trace elements
Introduction The essential trace element selenium was discovered in 1817 by the Swedish physician and chemist Jons Jakob Berzelius [1] and was named after Sκlenκ, the goddess of the moon. Only two selenium containing amino acids have been detected in proteins: Selenomethionine and selenocysteine. [2] The physiological role of selenomethionine-containing proteins remains unclear. [3],[4] However, selenocysteine is incorporated into proteins to form selenoproteins, which are involved in a variety of physiological functions. [1] Over the last century, our understanding of selenium has progressed considerably and we have come to recognize it as an essential component or cofactor of enzymes throughout metabolism, such as glutathione peroxidase (GPx), thioredoxine reductase and iodine deiodinase. [5],[6] GPx acts against hydrogen peroxide and lipid peroxidation and is an important line of defense against free radicals; thioredoxine reductase is involved in nucleus redox status; and iodine deiodinase is involved in thyroid hormone metabolism, which is frequently impaired in critically ill patients. Selenium also has an anticarcinogenic effect [7] that is thought to be induced by the production of methyselenol, a selenometabolite that affects gene expression and modifies cell cycling and immune function. [8] In the following sections, we will review the current knowledge concerning clinically relevant selenoproteins, discuss the potential role of these compounds in health and disease, review the epidemiology of selenium deficiency and its clinical implications with a special emphasis on critically ill patients and discuss the role of selenium supplementation in critical care settings. Historical Perspective In 1916, Gassmann et al ., [9] speculated on the biological importance of selenium as a component of bones and teeth of healthy individuals. Selenium′s reputation fell, however, when field research showed that selenium poisoning was the leading cause of "alkali" and "blind staggers" diseases, [10] threatening livestock in large farming communities. In addition, laboratory studies declared selenium to be a potential carcinogen. [11] Some decades later, Klaus Schwarz [12] provided strong evidence for a beneficial and essential role of selenium-containing (still not well defined) factor 3 against liver necrosis. [13] In the same era, Patterson and co-workers independently published a study in 1957 showing that selenium supplements prevented exudative diathesis in poultry. [14] In 1973, Turner and Stadtman [15] established that bacterial glycine reductase (EC 1.21.4.2) was a selenoprotein. Glutathione peroxidase was the first specific (that is genetically coded) mammalian selenoprotein to be discovered. In 1984, [16] Günzler et al ., discovered the amino acid sequence of GPx. This subsequently led to the establishment of selenocysteine as the 21 st proteinogenic amino acid. [17] In fact, the number of identified prokaryotic selenoproteins has increased by more than 100 to a total now of approximately 310. [18] Important Human Selenoproteins GPx was the first mammalian selenoprotein to be identified. [19] The GPx family includes seven isoenzymes in humans, of which GPx5 and GPx7 are not selenoenzymes. [20],[21] Apparently all the GPx share the same catalytic mechanism involving a strictly conserved triad formed by selenocysteine, tryptophan and glutamine. [22],[23] GPx play an important role in the body′s antioxidative armory. GPx reduce and thereby detoxify different types of peroxidases to their respective alcohols at the expense of (typically) glutathione. GPx1 is abundant in liver and erythrocytes, with its concentration being dependent on the nutritional selenium status. [1],[24] However, the vast majority of H 2 O 2 formed in erythrocytes is not detoxified by GPx but by catalase. [25] GPx2 is conserved under conditions of adequate selenium supply, [26],[27] and some authors suggest that it is the first line of defense against ingested hydroperoxides. [22],[28],[29] However, regulatory functions have also been suggested and it may be involved in apoptosis and proliferation. [30] GPx3 is present mainly in plasma [31] and its expression is induced by hypoxia. [32] GPx3 may have a regulatory function but this issue is not fully resolved. GPx4 exhibits the broadest substrate specificity and can even reduce phospholipid hydroperoxidase, even when integrated in membranes and may play a role as a universal antioxidant in the protection of biomembranes. [33],[34] GPx4 is also involved in redox signaling and regulatory processes, such as inhibition of lipoxygenase and apoptosis, [22],[35] and is required for sperm maturation. [36] The major selenoprotein in plasma is selenoprotein P (SelP). SelP provides more than 50% of the total plasma selenium. [37] It is transcribed in many tissues, yet the majority of the plasma SelP is secreted by the liver and presumably enters target cells via a receptor-mediated mechanism. [38] SelP is an established marker for nutritional (liver) selenium status [39],[40] and its primary function is storage and transport of selenium. [41],[42],[43] Nutritional selenium is delivered to the liver and used for SelP synthesis, which is toxologically - in contrast to most low molecular weight selenium compounds - rather inert. SelP is then secreted into the plasma and delivered to target tissues where SelP is transported intracellularly via receptor-mediated mechanisms. Within the cells, SelP and subsequently selenocysteine are degraded to liberate selenium, which is recycled for the synthesis of novel selenoproteins.
Selenium is also incorporated in the classical thioredoxin system, which is formed by thiorodoxin reductase (TrxR; TrxS2
+ NADPH + H+ → Trx(SH)2 + NADP+) and its associate substrate, the redox active protein, thioredoxin (Trx). Trx is reduced at the expense of NADPH. Reduced thioredoxin is reoxidized to provide reducing equivalents to various target molecules such as ribonucleotide reductase. [44] The thioredoxin system is involved in a myriad of cellular and intracellular processes. Thioredoxin reductase 1 (TrxR1) is a ubiquitous cytoplasmic housekeeping enzyme. It is capable of inducing apoptosis if the enzyme does not contain selonocysteine or if this residue is blocked, e.g. by chemotherapeutic agents. [45] Another important human selenoprotein is deiodinase (DIO), which cleaves specific iodine carbon bonds in thyroid hormones, thereby regulating their enzyme activity. Three types of thyroid DIO exist; types 1, 2, 3 have all been found to be selenoproteins. The thyroid gland has the highest per gram selenium content [46] as DIO and GPx and normal thyroid function depends on the two trace elements, iodine and selenium. Diminished DIO-1 levels are frequently encountered in low-T3 syndrome (accompanied by elevated levels of rT3), a clinical condition occasionally seen in critically ill patients, indicating the pivotal role of DIO-1 in the production of plasma T3 and in rT3 degeneration.
Other selenoproteins have been identified over the last two decades, the functions of which have not yet been fully characterized [Table - 1].
Etiology of Selenium Deficiency Selenium enters the food chain through plants, which take it up from the soil. Selenium deficiency has, therefore, been identified in parts of the world noted for their low soil content of selenium, such as volcanic regions. [47] Acid soil and complexation, frequently with iron and aluminum, also reduce the uptake of selenium by plants, as occurs in many parts of Europe [47] [Figure - 1]. At low or fairly low, selenium intake, serum or plasma selenium is well correlated with erythrocyte GPx activity. [47] At higher intakes, GPx activity reaches a plateau. [47] Serum or plasma selenium, being readily accessible, is therefore a useful marker of selenium status in populations with low levels of intake. However, levels of selenium intake that saturate the activity of plasma GPx, while satisfying the enzymatic or antioxidant role of selenium, are insufficient to optimize the immune response and reduce cancer risk.
The concentration of selenium in plasma is about 80% of that in whole blood. [8] Selenium concentrations in smokers, [48],[49] chronically ill persons, [50] the frail elderly, [51] children, [52] and pregnant and lactating women, [53],[54] may be 25%-30% lower than those in adult control subjects. [55] The value of plasma selenium levels in defining selenium deficiency remains, however, uncertain. While studies on selenium status and human immunodeficiency virus (HIV) disease have used a criterion of deficiency of < 85 ug/L, there is evidence that higher plasma levels are needed for optimal biological function. [5] In addition, selenium supplementation increased immune function in a study population with mean selenium levels > 130 ug/L, implying that these levels did not optimize immune function. [56]
In clinical nutrition, factors such as excessive metabolic demand for a given nutrient, increased losses or reduced intakes can participate in deficiency states. [57],[58] Severe selenium deficiency has been described in patients receiving selenium-deprived, long-term total parenteral or enteral nutrition. [59],[60] Low selenium status is also commonly observed in hepatic diseases, such as alcoholic cirrhosis and primary biliary cirrhosis, nutritional deficiency such as kwashiorkor, inflammatory gastrointestinal diseases and cystic fibrosis. [61]
Selenium in Various Disease Processes
Selenium deficiency-related diseases were first identified in livestock animals. [13] The most prominent examples in humans are Keshan disease, a dilatative cardiomyopathy primarily affecting children [62] and Kashin Beck disease, a disabling chondronecrosis. [63],[64],[65] Significantly lower serum selenium levels were also found in women who had either first-trimester or recurrent miscarriages. [66] Selenium is required for testosterone biosynthesis and the formation and the normal development of spermatozoa [67] and selenium supplementation significantly increased sperm motility. [67]
Numerous studies have suggested that deficiency of selenium is accompanied by loss of immunocompetence. [68] In addition, selenium supplementation, even in "selenium replete" individuals has marked immunostimulant effects, including an enhancement of the proliferation of activated T cells. [56] Moreover, activated T cells show upregulated selenophosphate synthetase activity, [69] directed at the synthesis of selenocysteine, the essential building block of selenoproteins. Immune dysfunction has been found to be secondary to the deficiency of selenium in HIV-infected patients and in persons with other diseases. [70] This dysfunction includes an impaired T cell response, decreased lymphocytes, including T cells, impaired phagocytic function and decreased immune cytotoxicity. Among HIV-infected pregnant women, low plasma selenuim levels were associated with increased risks of fetal death and HIV transmission through the intrapartum route. [71] Beck and colleagues have shown that in selenium deficient hosts, harmless viruses can become virulent. [72] If these findings were applicable to other RNA viruses, such as poliovirus, hepatitis, influenza and HIV, there would be considerable public health implications. In individuals infected with hepatitis (B or C), selenium also appears to be protective against the progression of the condition to liver cancer. [73],[74] Baum et al ., reported that the likelihood of death was increased about 20 times in selenium-deficient HIV patients compared with those with adequate selenium levels and that a low plasma selenium concentration is a more significant mortality risk than a low helper-T-cell count. [75]
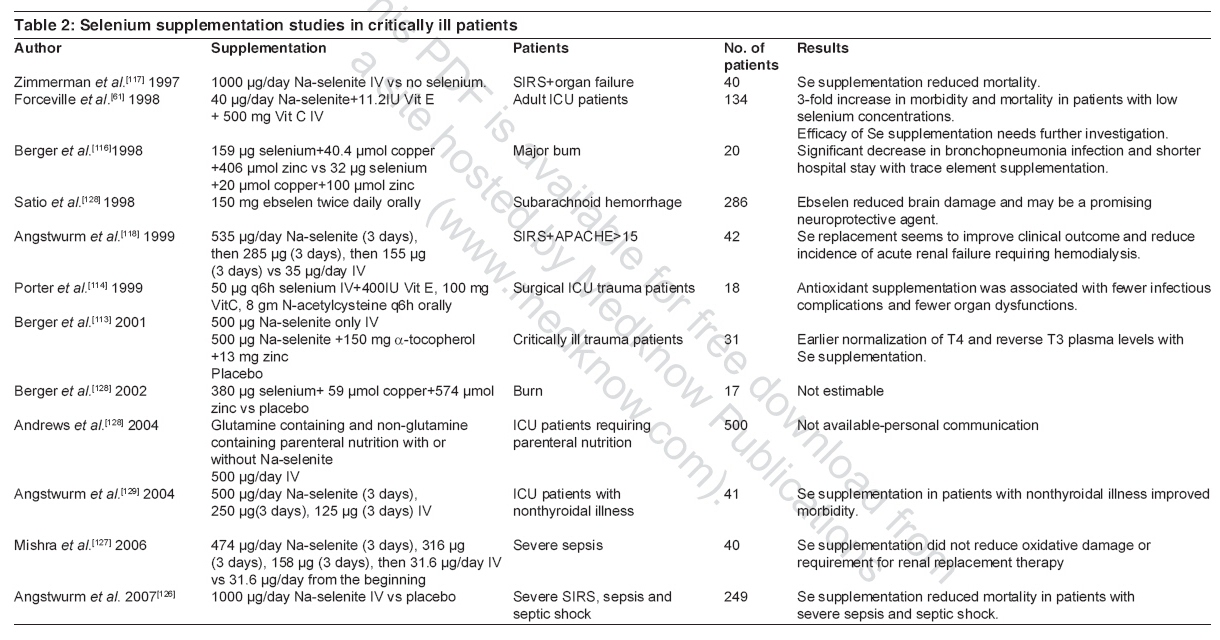
Table 2.
Selenium deficiency has also been shown to be associated with several forms of cardiovascular disease. [76] Selenium deficiency has been associated with a higher incidence of myocardial infarction and increased mortality rates from cardiovascular disease. [76] In men with coronary artery disease, platelet agreeability is inversely related to selenium status. [76],[77] Epidemiologic studies have, however, shown conflicting results. [76],[78],[79],[80] The disparity between these studies may be explained, in part, by the status of other antioxidants such as vitamin E, which may compensate for the deficiency in selenium in protecting against atherosclerosis. [81] The protective role of selenium in cardiovascular disease may be mediated by counteraction of lipid oxidation by GPx and reduction in platelet aggregation. [82]
Selenium behaves both as an antioxidant and an anti-inflammatory agent. This is because selenium in its antioxidant role, notably as GPx, can: i. reduce hydrogen peroxide, lipid and phospholipid hydroperoxides, thereby damping the propagation of free radicals and reactive oxygen species (ROS); ii. reduce hydroperoxide intermediates in the cyclo-oxygenase and lipoxygenase pathways, diminishing the production of inflammatory prostaglandins and leukotrienes; and iii. modulate the respiratory burst, by removal of hydrogen peroxide and reducing superoxide production. [68] Any condition associated with increased oxidative stress or inflammation might be expected to be influenced by selenium levels, which may be the case in rheumatoid arthritis, [83],[84] pancreatitis, [85] and asthma. [86],[87] Selenium has insulin-mimetic properties in vitro and in vivo , [88] probably by stimulating the tyrosine kinase involved in the distal signaling of the insulin signaling cascade. [89] When administered to streptozotocin-diabetic rats, selenium restores glycemic control and modifies the activity of a range of enzymes involved in hepatic glycolysis and gluconeogenesis. These changes are not linked to changes in insulin levels. [90],[91],[92],[93] A combination of selenium and iodine deficiency exacerbates hypothyroidism and may manifest itself as myxedema. [94] There is a higher incidence of thyroid tumors correlated with low levels of selenium. [95] Finally, patients with Alzheimer′s disease have lower brain selenium levels compared with controls [96] and a low selenium status has been associated with a significantly increased incidence of negative mood states, such as depression and anxiety. [97] Role of selenium in critical illness
In critical illness, ROS can be produced due to mitochondrial dysfunction [98] and impairment of the oxygen radical scavenger system of the body and a resulting increase in oxidant stress has been implicated in the evolution and maintenance of tissue injury in critically ill patients with multi-organ failure. [99],[100] In addition, selenium deficiency may activate some pro-inflammatory genes because selenium inhibits many transcription factors, such as activator protein (AP)-1 or nuclear factor-kappa B (NF-κB), involved in the transcription of various inflammatory mediators (e.g. tumor necrosis factor [TNF]-alpha). [101] Selenium also plays an important role in regulating the arachidonic acid cascade by controlling the concentration of lipid peroxides, [102] as well as the biosynthesis of thromboxane A2 and pro-inflammatory lipoxygenase products. [103],[104] Selenium deficiency may increase the thromboxane A2/prostacyclin ratio, thereby increasing vasoconstriction and blood coagulation. [105]
In a study of critically ill patients, plasma selenium concentrations remained low for > 2 weeks in patients with systemic inflammatory immune syndrome (SIRS) despite selenium supplementation. [61] However, there was a slight increase in plasma selenium concentrations in surviving SIRS patients, whereas plasma selenium concentrations decreased in non-surviving patients. [61] In patients after major trauma, Berger et al ., [105] showed that mean selenium levels were strongly decreased upon admission, reverting progressively to normal ranges after the first week following admission. The more severe the trauma, SIRS or sepsis, the larger the depletion of antioxidants appears to be. [106],[107] The decrease in plasma selenium levels in critically ill patients is multi-factorial: initiation of the acute phase response, [24],[108] hemodilution by resuscitation fluids and incompletely replaced biological fluid losses which contain large quantities of trace elements (mainly blood losses), are the main contributors. These described observations are not mere epiphenomena as low endogenous stores of antioxidants are associated with an increase in free radical generation, augmentation of the systemic inflammatory response, subsequent cell injury, increased morbidity and even higher mortality in the critically ill. [109],[110] Forceville et al ., [61] reported that plasma selenium measured on ICU admission, correlated inversely with APACHE II or SAPS II scores. Patients with SIRS had lower selenium concentrations than those without SIRS; selenium concentration was low in all patients with severe sepsis and septic shock and in those patients with ischemia-reperfusion from aortic cross-clamping. Low selenium values were associated with an increase in secondary complications and higher mortality rates. [61] The negative correlation between plasma selenium concentrations and mortality has been shown by several studies. In a large longitudinal French study [111] in an elderly population, the baseline plasma selenium was higher in individuals who were alive at the end of the 9-year follow up period than in those who died. After adjustment for various potential confounding factors, the association between lower plasma selenium levels and mortality remained significant. Forceville et al ., [61] reported that the frequencies of ventilator-associated pneumonia and organ system failure and the mortality rate were three times higher in patients with low plasma selenium concentrations at the time of admission to the ICU than for other patients. We [112] recently reported that plasma selenium levels were less than the standard values for healthy subjects in 92% of critically ill patients admitted to a surgical ICU. There was a consistent decrease in plasma selenium concentrations during the ICU stay in all patients. Interestingly, there was a tight relation between plasma selenium and all components of organ dysfunction/failure as assessed by the maximum sequential organ failure assessment (SOFA) score during the ICU stay. Plasma selenium concentrations were inversely correlated with serum C-reactive protein (CRP), procalcitonin (PCT) and interleukin (IL)-6. Previous studies have shown not only an association between low selenium concentrations and early mortality but also unfavorable long term outcomes.Selenium Supplementation in the Critically Ill As selenium deficiency is commonly associated with critical illness and with poor outcome, the notion of selenium supplementation in such patients is appealing. Supplementation with selenium has been shown to improve antioxidant capacity, as demonstrated by increased GPx activity. [113] Several randomized controlled studies have investigated the possible effect of selenium supplementation on outcome. [113],[114],[115],[116],[117],[118] However, most of these studies were performed on relatively small patient populations presenting with trauma, burns, sepsis or acute pancreatitis and thus are underpowered to detect a treatment effect on clinically important outcomes. [119] The current recommended dietary intake of selenium in humans is between 55 and 75 µg per day. [120] These amounts are based on the selenium intake that maximally induces the activity of GPx in plasma and erythrocytes. Low molecular weight selenium compounds [121] are important for the beneficial effect of selenium. [122],[123],[124] This might suggest that higher doses of selenium supplementation than the currently recommended 55-75 mg per day should be used. [125] However, the narrow therapeutic window of selenium should be taken in account - selenocompounds are toxic and their therapeutic index is rather small. [1] Angstwurm et al ., [118] demonstrated a reduction in the incidence of acute renal failure in patients suffering from SIRS who received supplemental selenium, even if their creatinine concentration was elevated at admission. Selenium supplementation has been associated with earlier normalization of thyroid profile in surgical ICU patients, [114] significant reduction in bronchpneumonia events and shorter hospital stays in burn patients, [116] and reduced mortality in septic patients [126] and patients with acute pancreatic necrosis. [115] However, the mortality benefit was not reproducible in another study [127] and another study could not find a significant effect regarding resolution of organ dysfunction, duration of intensive care unit (ICU) stay, incidence of mechanical ventilation, need for hemodialysis or vassopressor therapy or the incidence of acute respiratory distress syndrome (ARDS). [126] In a meta-analysis of randomized controlled studies (n=7) in 186 patients, selenium supplementation (alone or in combination with other antioxidants) was associated with a trend towards a lower mortality ( P =0.09), while non-selenium antioxidants were found to have no effect on mortality. Studies using high doses of selenium (500-1000 µg/day) [113],[115],[117],[118] were associated with a trend towards a lower mortality ( P =0.1), whereas studies using lower selenium doses (< 500 µg/day) [114],[116] showed no effect on mortality. No effect was observed on infectious complications, suggesting that the mortality effect was mediated by some other mechanisms, perhaps related to improved organ function. In a recent prospective, randomized placebo controlled, multi-center trial by Angstwurm and colleagues, 249 patients with severe SIRS, sepsis and septic shock were randomized to receive selenium or placebo. Patients in the study group received 1000 µg sodium selenite for 14 days. The primary end point of 28-day mortality was significantly reduced to 42.4% in the treatment group compared to 56.7% in the placebo group. In predefined subgroup analyses, the mortality rate was significantly reduced in patients with septic shock with disseminated intravascular coagulopathy as well as in the most critically ill patients with APACHE III scores > 102 or more than three organ dysfunctions. [126] Selenium supplementation in critical illness and other disease states is promising; however, large randomized multi-center studies are needed to confirm the beneficial effects of selenium supplementation in critically ill patients[129].
References
| 1. | Gromer S, Eubel JK, Lee BL, Jacob J. Human selenoproteins at a glance. Cell Mol Life Sci 2005;62:2414-37. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Subcommittee on Selenium National Research Council. Selenium in Nutrition. National Academy Press: Washington, DC; 1983. Back to cited text no. 2 |
| 3. | Hendrickson WA. Determination of macromolecular structures from anomalous diffraction of synchrotron radiation. Science 1991;254:51-8. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Hendrickson WA, Horton JR, LeMaster DM. Selenomethionyl proteins produced for analysis by multiwavelength anomalous diffraction (MAD): A vehicle for direct determination of three-dimensional structure. EMBO J 1990;9:1665-72. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Neve J. New approaches to assess selenium status and requirement. Nutr Rev 2000;58:363-9. Back to cited text no. 5 |
| 6. | Thomson CD. Assessment of requirements for selenium and adequacy of selenium status: A review. Eur J Clin Nutr 2004;58:391-402. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Bjelakovic G, Nikolova D, Simonetti RG, Gluud C. Antioxidant supplements for prevention of gastrointestinal cancers: A systematic review and meta-analysis. Lancet 2004;364:1219-28. Back to cited text no. 7 [PUBMED] [FULLTEXT] |
| 8. | Combs GF Jr. Selenium in global food systems. Br J Nutr 2001;85:517-47. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Gassmann T. Der Nachweis des Selens im Knochen-und Zahngewebe. Hoppe-Seyler's Z Physiol Chem 1916;97:307-10. Back to cited text no. 9 |
| 10. | Maxon AL. Alkali disease or selenium poisoning. So Dak Agric Exp Sta Tech Bull 1937;311:1-91. Back to cited text no. 10 |
| 11. | Tscherkes LA, Volgarev MN, Aptekar SG. Selenium-caused tumours. Acta Unio Int Contra Cancrum 1963;19:632-3. Back to cited text no. 11 |
| 12. | Birringer M, Pilawa S, Flohe L. Trends in selenium biochemistry. Nat Prod Rep 2002;19:693-718. Back to cited text no. 12 |
| 13. | Oldfield JE. A brief history of selenium research: From alkali disease to prostate cancer. J Anim Sci Online supplement 2002;11:1. Back to cited text no. 13 |
| 14. | Patterson EL, Milstrey R, Stokstad EL. Effect of selenium in preventing exudative diathesis in chicks. Proc Soc Exp Biol Med 1957;95:617-20. Back to cited text no. 14 |
| 15. | Turner DC, Stadtman TC. Purification of protein components of the clostridial glycine reductase system and characterization of protein A as a selenoprotein. Arch Biochem Biophys 1973;154:366-81. Back to cited text no. 15 |
| 16. | Gunzler WA, Steffens GJ, Grossmann A, Kim SM, Otting F, Wendel A, et al . The amino-acid sequence of bovine glutathione peroxidase. Hoppe Seylers Z Physiol Chem 1984;365:195-212. Back to cited text no. 16 |
| 17. | Bock A, Forchhammer K, Heider J, Leinfelder W, Sawers G, Veprek B, et al . Selenocysteine: The 21 st amino acid. Mol Microbiol 1991;5:515-20. Back to cited text no. 17 |
| 18. | Zhang Y, Fomenko DE, Gladyshev VN. The microbial selenoproteome of the Sargasso Sea. Genome Biol 2005;6:R37. Back to cited text no. 18 |
| 19. | Flohe L, Gunzler WA, Schock HH. Glutathione peroxidase: A selenoenzyme. FEBS Lett 1973;32:132-4. Back to cited text no. 19 |
| 20. | Hall L, Williams K, Perry AC, Frayne J, Jury JA. The majority of human glutathione peroxidase type 5 (GPX5) transcripts are incorrectly spliced: Implications for the role of GPX5 in the male reproductive tract. Biochem J 1998;333:5-9. Back to cited text no. 20 |
| 21. | Vernet P, Rigaudiere N, Ghyselinck N, Dufaure JP, Drevet JR. In vitro expression of a mouse tissue specific glutathione-peroxidase-like protein lacking the selenocysteine can protect stably transfected mammalian cells against oxidative damage. Biochem Cell Biol 1996;74:125-31. Back to cited text no. 21 |
| 22. | Brigelius-Flohe R. Tissue-specific functions of individual glutathione peroxidases. Free Radic Biol Med 1999;27:951-65. Back to cited text no. 22 |
| 23. | Aumann KD, Bedorf N, Brigelius-Flohe R, Schomburg D, Flohe L. Glutathione peroxidase revisited--simulation of the catalytic cycle by computer-assisted molecular modeling. Biomed Environ Sci 1997;10:136-55. Back to cited text no. 23 |
| 24. | Singh A, Smoak BL, Patterson KY, LeMay LG, Veillon C, Deuster PA. Biochemical indices of selected trace minerals in men: Effect of stress. Am J Clin Nutr 1991;53:126-31. Back to cited text no. 24 |
| 25. | Mueller S, Riedel HD, Stremmel W. Direct evidence for catalase as the predominant H2O2 -removing enzyme in human erythrocytes. Blood 1997;90:4973-8. Back to cited text no. 25 |
| 26. | Hamanishi T, Furuta H, Kato H, Doi A, Tamai M, Shimomura H, et al . Functional variants in the glutathione peroxidase-1 (GPx-1) gene are associated with increased intima-media thickness of carotid arteries and risk of macrovascular diseases in Japanese type 2 diabetic patients. Diabetes 2004;53:2455-60 Back to cited text no. 26 |
| 27. | Wingler K, Brigelius-Flohe R. Gastrointestinal glutathione peroxidase. Biofactors 1999;10:245-9. Back to cited text no. 27 |
| 28. | Brigelius-Flohe R, Muller C, Menard J, Florian S, Schmehl K, Wingler K. Functions of GI-GPx: Lessons from selenium-dependent expression and intracellular localization. Biofactors 2001;14:101-6. Back to cited text no. 28 |
| 29. | Wingler K, Bocher M, Flohe L, Kollmus H, Brigelius-Flohe R. mRNA stability and selenocysteine insertion sequence efficiency rank gastrointestinal glutathione peroxidase high in the hierarchy of selenoproteins. Eur J Biochem 1999;259:149-57. Back to cited text no. 29 |
| 30. | Florian S, Wingler K, Schmehl K, Jacobasch G, Kreuzer OJ, Meyerhof W, et al . Cellular and subcellular localization of gastrointestinal glutathione peroxidase in normal and malignant human intestinal tissue. Free Radic Res 2001;35:655-63. Back to cited text no. 30 |
| 31. | Tham DM, Whitin JC, Kim KK, Zhu SX, Cohen HJ. Expression of extracellular glutathione peroxidase in human and mouse gastrointestinal tract. Am J Physiol 1998;275:G1463-71. Back to cited text no. 31 |
| 32. | Bierl C, Voetsch B, Jin RC, Handy DE, Loscalzo J. Determinants of human plasma glutathione peroxidase (GPx-3) expression. J Biol Chem 2004;279:26839-45. Back to cited text no. 32 |
| 33. | Ursini F, Maiorino M, Valente M, Ferri L, Gregolin C. Purification from pig liver of a protein which protects liposomes and biomembranes from peroxidative degradation and exhibits glutathione peroxidase activity on phosphatidylcholine hydroperoxides. Biochim Biophys Acta 1982;710:197-211. Back to cited text no. 33 |
| 34. | Ursini F, Maiorino M, Gregolin C. The selenoenzyme phospholipid hydroperoxide glutathione peroxidase. Biochim Biophys Acta 1985;839:62-70. Back to cited text no. 34 |
| 35. | Brigelius-Flohe R, Friedrichs B, Maurer S, Schultz M, Streicher R. Interleukin-1-induced nuclear factor kappa B activation is inhibited by overexpression of phospholipid hydroperoxide glutathione peroxidase in a human endothelial cell line. Biochem J 1997;328:199-203. Back to cited text no. 35 |
| 36. | Ursini F, Heim S, Kiess M, Maiorino M, Roveri A, Wissing J, et al . Dual function of the selenoprotein PHGPx during sperm maturation. Science 1999;285:1393-6. Back to cited text no. 36 |
| 37. | Mostert V. Selenoprotein P: Properties, functions and regulation. Arch Biochem Biophys 2000;376:433-8. Back to cited text no. 37 |
| 38. | Gomez B, Jr, Tappel AL. Selenoprotein P receptor from rat. Biochim Biophys Acta 1989;979:20-6. Back to cited text no. 38 |
| 39. | Schweizer U, Streckfuss F, Pelt P, Carlson BA, Hatfield DL, Kohrle J, et al . Hepatically derived selenoprotein P is a key factor for kidney but not for brain selenium supply. Biochem J 2005;386:221-6. Back to cited text no. 39 |
| 40. | Persson-Moschos M, Huang W, Srikumar TS, Akesson B, Lindeberg S. Selenoprotein P in serum as a biochemical marker of selenium status. Analyst 1995;120:833-6. Back to cited text no. 40 |
| 41. | Motsenbocker MA, Tappel AL. A selenocysteine-containing selenium-transport protein in rat plasma. Biochim Biophys Acta 1982;719:147-53. Back to cited text no. 41 |
| 42. | Saito Y, Takahashi K. Characterization of selenoprotein P as a selenium supply protein. Eur J Biochem 2002;269:5746-51. Back to cited text no. 42 |
| 43. | Saito Y, Sato N, Hirashima M, Takebe G, Nagasawa S, Takahashi K. Domain structure of bi-functional selenoprotein P. Biochem J 2004;381:841-6. Back to cited text no. 43 |
| 44. | Gromer S, Urig S, Becker K. The thioredoxin system--from science to clinic. Med Res Rev 2004;24:40-89. Back to cited text no. 44 |
| 45. | Anestal K, Arner ES. Rapid induction of cell death by selenium-compromised thioredoxin reductase 1 but not by the fully active enzyme containing selenocysteine. J Biol Chem 2003;278:15966-72. Back to cited text no. 45 |
| 46. | Dickson RC, Tomlinson RH. Selenium in blood and human tissues. Clin Chim Acta 1967;16:311-21. Back to cited text no. 46 |
| 47. | Reilly C. Selenium in food and health. Blackie Academic and Professional: London; 1996. Back to cited text no. 47 |
| 48. | Bates CJ, Thane CW, Prentice A, Delves HT. Selenium status and its correlates in a British national diet and nutrition survey: People aged 65 years and over. J Trace Elem Med Biol 2002;16:1-8. Back to cited text no. 48 |
| 49. | Kafai MR, Ganji V. Sex, age, geographical location, smoking and alcohol consumption influence serum selenium concentrations in the USA: Third National Health and Nutrition Examination Survey, 1988-1994. J Trace Elem Med Biol 2003;17:13-8. Back to cited text no. 49 |
| 50. | Rayman MP, Rayman MP. The argument for increasing selenium intake. Proc Nutr Soc 2002;61:203-15. Back to cited text no. 50 |
| 51. | Campbell D, Bunker VW, Thomas AJ, Clayton BE. Selenium and vitamin E status of healthy and institutionalized elderly subjects: Analysis of plasma, erythrocytes and platelets. Br J Nutr 1989;62:221-7. Back to cited text no. 51 |
| 52. | Barany E, Bergdahl IA, Bratteby LE, Lundh T, Samuelson G, Schutz A, et al . Relationships between trace element concentrations in human blood and serum. Toxicol Lett 2002;134:177-84. Back to cited text no. 52 |
| 53. | Reyes H, Baez ME, Gonzalez MC, Hernandez I, Palma J, Ribalta J, et al . Selenium, zinc and copper plasma levels in intrahepatic cholestasis of pregnancy, in normal pregnancies and in healthy individuals, in Chile. J Hepatol 2000;32:542-9. Back to cited text no. 53 |
| 54. | Cumming FJ, Fardy JJ, Woodward DR. Selenium and human lactation in Australia: Milk and blood selenium levels in lactating women and selenium intakes of their breast-fed infants. Acta Paediatr 1992;81:292-5. Back to cited text no. 54 |
| 55. | Lyons GH, Judson GJ, Stangoulis JC, Palmer LT, Jones JA, Graham RD. Trends in selenium status of South Australians. Med J Aust 2004;180:383-6. Back to cited text no. 55 |
| 56. | Kiremidjian-Schumacher L, Roy M, Wishe HI, Cohen MW, Stotzky G. Supplementation with selenium and human immune cell functions. II. Effect on cytotoxic lymphocytes and natural killer cells. Biol Trace Elem Res 1994;41:115-27. Back to cited text no. 56 |
| 57. | Mertz W. The essential trace elements. Science 1981;213:1332-8 Back to cited text no. 57 |
| 58. | Solomon N. Trace ιlιments. In : Rombeau JL, Caldwell MD, editors. Clinical nutrition: parenteral nutrition. WB Saunders: Philadelphia; 1993. p. 150-84. Back to cited text no. 58 |
| 59. | Leung FY. Trace elements in parenteral micronutrition. Clin Biochem 1995;28:561-6. Back to cited text no. 59 |
| 60. | Okada A, Takagi Y, Nezu R, Sando K, Shenkin A. Trace element metabolism in parenteral and enteral nutrition. Nutrition 1995;11:106-13. Back to cited text no. 60 |
| 61. | Forceville X, Vitoux D, Gauzit R, Combes A, Lahilaire P, Chappuis P. Selenium, systemic immune response syndrome, sepsis and outcome in critically ill patients. Crit Care Med 1998;26:1536-44. Back to cited text no. 61 |
| 62. | Ge K, Xue A, Bai J, Wang S. Keshan disease-an endemic cardiomyopathy in China. Virchows Arch A Pathol Anat Histopathol 1983;401:1-15. Back to cited text no. 62 |
| 63. | Peng X, Lingxia Z, Schrauzer GN, Xiong G. Selenium, boron and germanium deficiency in the etiology of Kashin-Beck disease. Biol Trace Elem Res 2000;77:193-7. Back to cited text no. 63 |
| 64. | Ge K, Yang G. The epidemiology of selenium deficiency in the etiological study of endemic diseases in China. Am J Clin Nutr 1993;57:259S-63S. Back to cited text no. 64 |
| 65. | Moreno-Reyes R, Suetens C, Mathieu F, Begaux F, Zhu D, Rivera MT, et al . Kashin-Beck osteoarthropathy in rural Tibet in relation to selenium and iodine status. N Engl J Med 1998;339:1112-20. Back to cited text no. 65 |
| 66. | Barrington JW, Taylor M, Smith S, Bowen-Simpkins P. Selenium and recurrent miscarriage. J Obstet Gynaecol 1997;17:199-200. Back to cited text no. 66 |
| 67. | Scott R, MacPherson A, Yates RW, Hussain B, Dixon J. The effect of oral selenium supplementation on human sperm motility. Br J Urol 1998;82:76-80. Back to cited text no. 67 |
| 68. | Spallholz JE, Boylan LM, Larsen HS. Advances in understanding selenium's role in the immune system. Ann N Y Acad Sci 1990;587:123-39. Back to cited text no. 68 |
| 69. | Guimaraes MJ, Peterson D, Vicari A, Cocks BG, Copeland NG, Gilbert DJ, et al . Identification of a novel selD homolog from eukaryotes, bacteria and archaea: Is there an autoregulatory mechanism in selenocysteine metabolism? Proc Natl Acad Sci U S A 1996;93:15086-91. Back to cited text no. 69 |
| 70. | Taylor EW. Selenium and cellular immunity. Evidence that selenoproteins may be encoded in the +1 reading frame overlapping the human CD4, CD8 and HLA-DR genes. Biol Trace Elem Res 1995;49:85-95. Back to cited text no. 70 |
| 71. | Kupka R, Msamanga GI, Spiegelman D, Morris S, Mugusi F, Hunter DJ, et al . Selenium status is associated with accelerated HIV disease progression among HIV-1-infected pregnant women in Tanzania. J Nutr 2004;134:2556-60. Back to cited text no. 71 |
| 72. | Beck MA, Shi Q, Morris VC, Levander OA. Rapid genomic evolution of a non-virulent coxsackievirus B3 in selenium-deficient mice results in selection of identical virulent isolates. Nat Med 1995;1:433-6. Back to cited text no. 72 |
| 73. | Yu SY, Zhu YJ, Li WG. Protective role of selenium against hepatitis B virus and primary liver cancer in Qidong. Biol Trace Elem Res 1997;56:117-24. Back to cited text no. 73 |
| 74. | Yu MW, Horng IS, Hsu KH, Chiang YC, Liaw YF, Chen CJ. Plasma selenium levels and risk of hepatocellular carcinoma among men with chronic hepatitis virus infection. Am J Epidemiol 1999;150:367-74. Back to cited text no. 74 |
| 75. | Baum MK, Shor-Posner G, Lai S, Zhang G, Lai H, Fletcher MA, et al . High risk of HIV-related mortality is associated with selenium deficiency. J Acquir Immune Defic Syndr Hum Retrovirol 1997;15:370-4. Back to cited text no. 75 |
| 76. | Neve J. Selenium as a risk factor for cardiovascular diseases. J Cardiovasc Risk 1996;3:42-7. Back to cited text no. 76 |
| 77. | Salonen JT, Salonen R, Seppanen K, Kantola M, Parviainen M, Alfthan G, et al . Relationship of serum selenium and antioxidants to plasma lipoproteins, platelet agreeability and prevalent ischaemic heart disease in Eastern Finnish men. Atherosclerosis 1988;70:155-60. Back to cited text no. 77 |
| 78. | Wei WQ, Abnet CC, Qiao YL, Dawsey SM, Dong ZW, Sun XD, et al . Prospective study of serum selenium concentrations and esophageal and gastric cardia cancer, heart disease, stroke and total death. Am J Clin Nutr 2004;79:80-5. Back to cited text no. 78 |
| 79. | Yoshizawa K, Ascherio A, Morris JS, Stampfer MJ, Giovannucci E, Baskett CK, et al . Prospective study of selenium levels in toenails and risk of coronary heart disease in men. Am J Epidemiol 2003;158:852-60. Back to cited text no. 79 |
| 80. | Salonen JT, Alfthan G, Huttunen JK, Pikkarainen J, Puska P. Association between cardiovascular death and myocardial infarction and serum selenium in a matched-pair longitudinal study. Lancet 1982;2:175-9. Back to cited text no. 80 |
| 81. | Kardinaal AF, Kok FJ, Kohlmeier L, Martin-Moreno JM, Ringstad J, Gomez-Aracena J, et al . Association between toenail selenium and risk of acute myocardial infarction in European men. The EURAMIC Study. European Antioxidant Myocardial Infarction and Breast Cancer. Am J Epidemiol 1997;145:373-9. Back to cited text no. 81 |
| 82. | Neve J. Physiological and nutritional importance of selenium. Experientia 1991;47:187-93. Back to cited text no. 82 |
| 83. | Knekt P, Heliovaara M, Aho K, Alfthan G, Marniemi J, Aromaa A. Serum selenium, serum alpha-tocopherol and the risk of rheumatoid arthritis. Epidemiology 2000;11:402-5. Back to cited text no. 83 |
| 84. | Peretz A, Neve J, Duchateau J, Famaey JP. Adjuvant treatment of recent onset rheumatoid arthritis by selenium supplementation: Preliminary observations. Br J Rheumatol 1992;31:281-2. Back to cited text no. 84 |
| 85. | Kuklinski B, Schweder R. Acute pancreatitis, a free radical disease: Reducing the lethality with sodium selenite and other antioxidants. J Nutr Environ Med 1996;6:393-4. Back to cited text no. 85 |
| 86. | Shaw R, Woodman K, Crane J, Moyes C, Kennedy J, Pearce N. Risk factors for asthma symptoms in Kawerau children. N Z Med J 1994;107:387-91. Back to cited text no. 86 |
| 87. | Hasselmark L, Malmgren R, Zetterstrom O, Unge G. Selenium supplementation in intrinsic asthma. Allergy 1993;48:30-6. Back to cited text no. 87 |
| 88. | Beckett GJ, Arthur JR. Selenium and endocrine systems. J Endocrinol 2005;184:455-65. Back to cited text no. 88 |
| 89. | McKenzie RC, Arthur JR, Beckett GJ. Selenium and the regulation of cell signaling, growth and survival: Molecular and mechanistic aspects. Antioxid Redox Signal 2002;4:339-51. Back to cited text no. 89 |
| 90. | McNeill JH, Delgatty HL, Battell ML. Insulin like effects of sodium selenate in streptozocin-induced diabetic rats. Diabetes 1991;40:1675-8. Back to cited text no. 90 |
| 91. | Ghosh R, Mukherjee B, Chatterjee M. A novel effect of selenium on streptozotocin-induced diabetic mice. Diabetes Res 1994;25:165-71. Back to cited text no. 91 |
| 92. | Becker DJ, Reul B, Ozcelikay AT, Buchet JP, Henquin JC, Brichard SM. Oral selenate improves glucose homeostasis and partly reverses abnormal expression of liver glycolytic and gluconeogenic enzymes in diabetic rats. Diabetologia 1996;39:3-11. Back to cited text no. 92 |
| 93. | Mukherjee B, Anbazhagan S, Roy A, Ghosh R, Chatterjee M. Novel implications of the potential role of selenium on antioxidant status in streptozotocin-induced diabetic mice. Biomed Pharmacother 1998;52:89-95. Back to cited text no. 93 |
| 94. | Vanderpas JB, Contempre B, Duale NL, Goossens W, Bebe N, Thorpe R, et al . Iodine and selenium deficiency associated with cretinism in northern Zaire. Am J Clin Nutr 1990;52:1087-93. Back to cited text no. 94 |
| 95. | Glattre E, Thomassen Y, Thoresen SO, Haldorsen T, Lund-Larsen PG, Theodorsen L, et al . Prediagnostic serum selenium in a case-control study of thyroid cancer. Int J Epidemiol 1989;18:45-9. Back to cited text no. 95 |
| 96. | Hawkes WC, Hornbostel L. Effects of dietary selenium on mood in healthy men living in a metabolic research unit. Biol Psychiatry 1996;39:121-8. Back to cited text no. 96 |
| 97. | Benton D, Cook R. The impact of selenium supplementation on mood. Biol Psychiatry 1991;29:1092-8. Back to cited text no. 97 |
| 98. | Brealey D, Brand M, Hargreaves I, Heales S, Land J, Smolenski R, et al . Association between mitochondrial dysfunction and severity and outcome of septic shock. Lancet 2002;360:219-23. Back to cited text no. 98 |
| 99. | Freeman BA, Crapo JD. Biology of disease: Free radicals and tissue injury. Lab Invest 1982;47:412-26. Back to cited text no. 99 |
| 100. | Takeda K, Shimada Y, Amano M, Sakai T, Okada T, Yoshiya I. Plasma lipid peroxides and alpha-tocopherol in critically ill patients. Crit Care Med 1984;12:957-9. Back to cited text no. 100 |
| 101. | Handel ML, Watts CK, deFazio A, Day RO, Sutherland RL. Inhibition of AP-1 binding and transcription by gold and selenium involving conserved cysteine residues in Jun and Fos. Proc Natl Acad Sci U S A 1995;92:4497-501. Back to cited text no. 101 |
| 102. | Eisenmann CJ, Miller RK. The effect of selenium compounds (selenite, selenate, ebselen) on the production of thromboxane and prostacyclin by the human term placenta in vitro. Toxicol Appl Pharmacol 1995;135:18-24. Back to cited text no. 102 |
| 103. | Perona G, Schiavon R, Guidi GC, Veneri D, Minuz P. Selenium dependent glutathione peroxidase: A physiological regulatory system for platelet function. Thromb Haemost 1990;64:312-8. Back to cited text no. 103 |
| 104. | Natarajan V. Oxidants and signal transduction in vascular endothelium. J Lab Clin Med 1995;125:26-37. Back to cited text no. 104 |
| 105. | Berger MM, Cavadini C, Chiolero R, Dirren H. Copper, selenium and zinc status and balances after major trauma. J Trauma 1996;40:103-9. Back to cited text no. 105 |
| 106. | Alonso de Vega JM, Diaz J, Serrano E, Carbonell LF. Oxidative stress in critically ill patients with systemic inflammatory response syndrome. Crit Care Med 2002;30:1782-6. Back to cited text no. 106 |
| 107. | Motoyama T, Okamoto K, Kukita I, Hamaguchi M, Kinoshita Y, Ogawa H. Possible role of increased oxidant stress in multiple organ failure after systemic inflammatory response syndrome. Crit Care Med 2003;31:1048-52. Back to cited text no. 107 |
| 108. | Young AB, Ott LG, Beard D, Dempsey RJ, Tibbs PA, McClain CJ. The acute-phase response of the brain-injured patient. J Neurosurg 1988;69:375-80. Back to cited text no. 108 |
| 109. | Metnitz PG, Bartens C, Fischer M, Fridrich P, Steltzer H, Druml W. Antioxidant status in patients with acute respiratory distress syndrome. Intensive Care Med 1999;25:180-5. Back to cited text no. 109 |
| 110. | Goode HF, Cowley HC, Walker BE, Howdle PD, Webster NR. Decreased antioxidant status and increased lipid peroxidation in patients with septic shock and secondary organ dysfunction. Crit Care Med 1995;23:646-51. Back to cited text no. 110 |
| 111. | Akbaraly NT, Arnaud J, Hininger-Favier I, Gourlet V, Roussel AM, Berr C. Selenium and mortality in the elderly: Results from the EVA study. Clin Chem 2005;51:2117-23. Back to cited text no. 111 |
| 112. | Sakr Y, Reinhart K, Bloos F, Marx G, Russwurm S, Bauer M, et al . Time course and relationship between plasma selenium concentrations, systemic inflammatory response, sepsis and multiorgan failure. Br J Anaesth 2007;98:775-84. Back to cited text no. 112 |
| 113. | Berger MM, Reymond MJ, Shenkin A, Rey F, Wardle C, Cayeux C, et al . Influence of selenium supplements on the post-traumatic alterations of the thyroid axis: A placebo-controlled trial. Intensive Care Med 2001;27:91-100. Back to cited text no. 113 |
| 114. | Porter JM, Ivatury RR, Azimuddin K, Swami R. Antioxidant therapy in the prevention of organ dysfunction syndrome and infectious complications after trauma: Early results of a prospective randomized study. Am Surg 1999;65:478-83. Back to cited text no. 114 |
| 115. | Kuklinski B, Buchner M, Schweder R, Nagel R. Acute pancreatitis--a free radical disease. Decrease in fatality with sodium selenite (Na2SeO3) therapy. Z Gesamte Inn Med 1991;46:145-9. Back to cited text no. 115 |
| 116. | Berger MM, Spertini F, Shenkin A, Wardle C, Wiesner L, Schindler C, et al . Trace element supplementation modulates pulmonary infection rates after major burns: a double-blind, placebo-controlled trial. Am J Clin Nutr 1998;68:365-71. Back to cited text no. 116 |
| 117. | Zimmermann T, Albrecht S, Kuhne H, Vogelsang U, Grutzmann R, Kopprasch S. Selenium administration in patients with sepsis syndrome. A prospective randomized study. Med Klin (Munich) 1997;92:3-4. Back to cited text no. 117 |
| 118. | Angstwurm MW, Schottdorf J, Schopohl J, Gaertner R. Selenium replacement in patients with severe systemic inflammatory response syndrome improves clinical outcome. Crit Care Med 1999;27:1807-13. Back to cited text no. 118 |
| 119. | Heyland DK, Dhaliwal R, Suchner U, Berger MM. Antioxidant nutrients: A systematic review of trace elements and vitamins in the critically ill patient. Intensive Care Med 2005;31:327-37. Back to cited text no. 119 |
| 120. | Rayman MP. The importance of selenium to human health. Lancet 2000;356:233-41. Back to cited text no. 120 |
| 121. | Ip C, Thompson HJ, Zhu Z, Ganther HE. In vitro and in vivo studies of methylseleninic acid: Evidence that a monomethylated selenium metabolite is critical for cancer chemoprevention. Cancer Res 2000;60:2882-6. Back to cited text no. 121 |
| 122. | Combs GF Jr. Chemopreventive mechanisms of selenium. Med Klin (Munich) 1999;94:18-24. Back to cited text no. 122 |
| 123. | Davis CD, Uthus EO. Dietary folate and selenium affect dimethylhydrazine-induced aberrant crypt formation, global DNA methylation and one-carbon metabolism in rats. J Nutr 2003;133:2907-14. Back to cited text no. 123 |
| 124. | Davis CD, Uthus EO, Finley JW. Dietary selenium and arsenic affect DNA methylation in vitro in Caco-2 cells and in vivo in rat liver and colon. J Nutr 2000;130:2903-9. Back to cited text no. 124 |
| 125. | Food and Nutrition Board Institute of Medicine. Selenium. In : Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium and Carotenoids. A Report of the Panel on Dietary Antioxidants and Related Compounds. National Academy Press: Washington, DC; 2000. Back to cited text no. 125 |
| 126. | Angstwurm MW, Engelmann L, Zimmermann T, Lehmann C, Spes CH, Abel P, et al . Selenium in Intensive Care (SIC): Results of a prospective randomized, placebo-controlled, multiple-center study in patients with severe systemic inflammatory response syndrome, sepsis and septic shock. Crit Care Med 2007;35:118-26 Back to cited text no. 126 |
| 127. | Mishra V, Baines M, Perry SE, McLaughlin PJ, Carson J, Wenstone R, et al . Effect of selenium supplementation on biochemical markers and outcome in critically ill patients. Clin Nutr 2007;26:41-50. Back to cited text no. 127 |
| 128. | Avenell A, Noble DW, Barr J, Engelhardt T. Selenium supplementation for critically ill adults. Cochrane Database Syst Rev 2004;CD003703. Back to cited text no. 128 |
| 129. | Angstwurm MW, Schopohl J, Gaertner R. Selenium substitution has no direct effect on thyroid hormone metabolism in critically ill patients. Eur J Endocrinol 2004;151:47-54. Back to cited text no. 129 |
Copyright 2007 - Indian Journal of Critical Care Medicine
The following images related to this document are available:
Photo images
[cm07024t1.jpg]
[cm07024f1.jpg]
[cm07024t2.jpg]
|

{kind=link}