
|
Indian Journal of Critical Care Medicine
Medknow Publications on behalf of the Indian Society of Critical Care Medicine
ISSN: 0972-5229 EISSN: 1998-359x
Vol. 12, Num. 1, 2008, pp. 1-9
|
Indian Journal of Critical Care Medicine, Vol. 12, No. 1, January-March, 2008, pp. 1-9
Review Article
Extubation failure in intensive care unit: Predictors and management
Kulkarni AtulP, Agarwal Vandana
Department of Anesthesiology, Critical Care and Pain, Tata Memorial Hospital, Parel, Mumbai, Maharashtra
Correspondence Address:Department of Anesthesiology, Critical Care and Pain, Tata Memorial Hospital, Dr Ernest Borges Road, Parel, Mumbai - 400 012, Maharashtra
kaivalyaak@yahoo.co.in
Code Number: cm08001
Abstract
Extubation failure-need for reintubation within 72 h of extubation, is common in intensive care unit (ICU). It can cause increased morbidity, higher costs, higher ICU and hospital length of stay (LOS) and mortality. Patients with advanced age, high severity of illness at ICU admission and extubation, preexisting chronic respiratory and cardiovascular disorders are at increased risk of extubation failure. Unresolved illness, development and progression of organ failure during the time from extubation to reintubation and reintubation itself have been proposed as reasons for increased morbidity and mortality. Parameters used to predict extubation failure can be categorized into parameters assessing respiratory mechanics, airway patency and protection and cardiovascular reserve. Adequate cough strength, minimal secretions and alertness are necessary for successful extubation. Evidence suggests that early institution of non-invasive ventilation and prophylactic administration of methylprednisolone may prevent reintubation in some patients. The intensivist needs to identify patients at high risk of extubation failure and be prepared to reinstitute ventilation early to prevent adverse outcomes.
Keywords: Extubation, failure of, predictors of, reintubation, weaning
Introduction After resolution of illness, mechanically ventilated patients are liberated from the ventilator, the process being called weaning. It is essential to understand that weaning and extubation though following each other in clinical practice, are two separate processes which pose distinct problems. Extubation failure is defined as inability to sustain spontaneous breathing after removal of the artificial airway; an endotracheal tube or tracheostomy tube; and need for reintubation within a specified time period: either within 24-72 h [1],[2] or up to 7 days. [3],[4] Substantial literature exists about weaning predictors and outcomes; most being inaccurate in predicting extubation outcome. To predict "extubation failure" is essential, as both delayed and failed extubation have detrimental consequences such as prolonged ventilation and ICU stay, need for tracheostomy, increased cost of treatment and mortality. [5],[6],[7] In this review, we discuss causes, outcomes, predictors and management of extubation failure in patients passing spontaneous breathing trial (SBT).
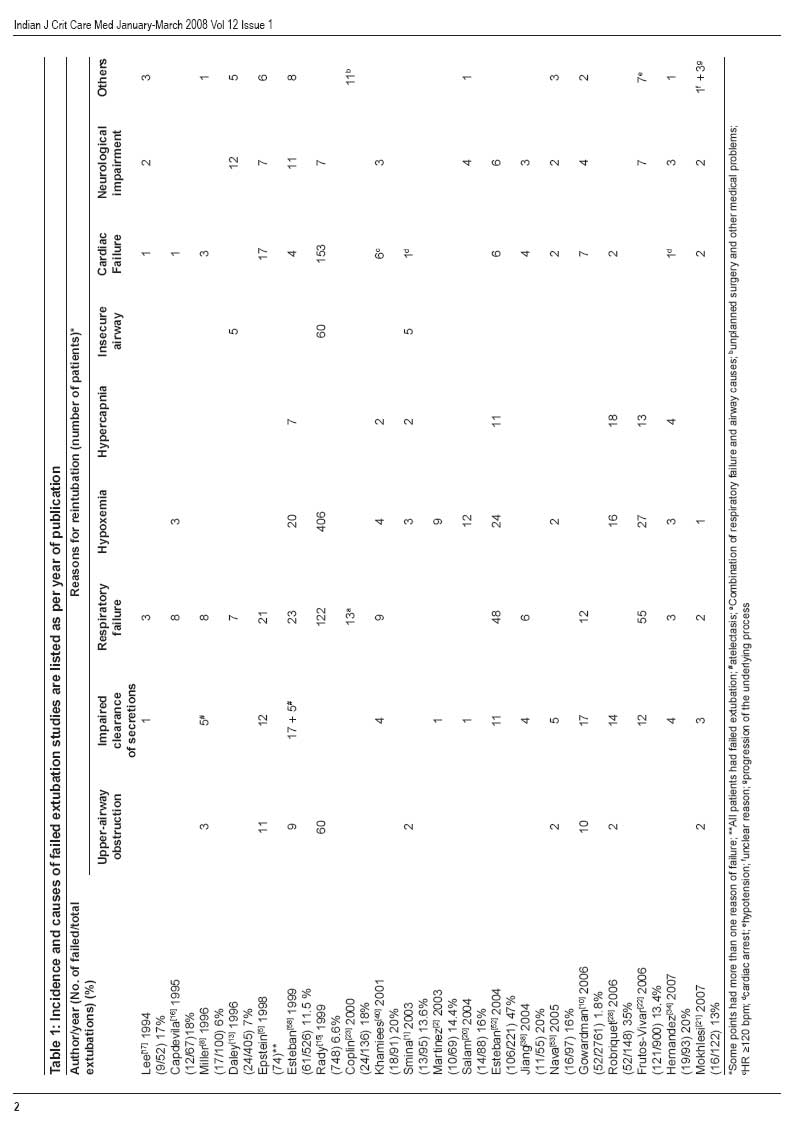
Incidence and Consequences of -Extubation Failure Incidence of extubation failure [Table - 1] varies between 6 and 47%. [3],[8],[9] Epstein [3] and Gowardman [10] found that patients needing reintubation had significantly increased duration of mechanical ventilation as well as ICU and hospital LOS and mortality. The OUTCOMERA study group [11] found a significant increase in the incidence of nosocomial pneumonia with consequent increase in the duration of mechanical ventilation, hospital and ICU LOS, without increased mortality. In a case control study, [7] the incidence of pneumonia was significantly higher (47% vs. 10%) in patients needing reintubation. Dries and colleagues [12] also found an increased incidence of nosocomial pneumonia in patients who failed extubation. The reported [3],[5] mortality rates in patients with extubation failure vary between 30 and 40%.
Extubation Failure and Adverse -Outcomes: Pathophysiology Deconditioned muscles, poor nutrition, upper airway edema due to prolonged translaryngeal intubation, inability to clear secretions, decreased level of consciousness due to persistent effects of sedative and analgesics and critical illness polyneuropathy; all can lead to extubation failure. Several hypotheses attempt to explain increased mortality associated with failed extubation. One hypothesis is that increased mortality after extubation failure may reflect a sicker cohort of patients, [3] with failed extubation acting as an additional marker of severity of illness. This derives from the fact that extubation failure retains a strong independent effect on mortality even after adjusting for confounders such as generalized severity of illness, chronic comorbidities, age and need for acute dialysis. Second hypothesis is that reintubation, an invasive procedure, may itself increase mortality. This may be due to the life-threatening events during reintubation such as cardiac arrest, esophageal intubation, endobronchial intubation, aspiration of gastric contents and cardiac arrhythmias. Torres and colleagues [7] found that patients requiring reintubation were more likely to develop nosocomial pneumonia (47% vs. 10%) with increased mortality. However, if reintubation itself caused mortality, then mortality should not vary for different causes of extubation failure. Esteban and colleagues [4] found a lower mortality for patients reintubated for upper airway obstruction than those reintubated for respiratory failure (7% vs. 30%). This is because reintubation for upper airway obstruction rapidly corrects respiratory dysfunction; whereas organ dysfunction related to other causes of extubation failure may not be readily reversible. Mortality, however, was not different in trauma patients [13] needing reintubation for stridor, inability to clear secretions or deteriorating sensorium. Third hypothesis is that clinical deterioration occurs during spontaneous breathing with development of new organ dysfunction, thereby increasing mortality. This may explain in part the relationship between cause of extubation failure and outcome. This hypothesis is further supported by increase in mortality with increasing duration of time between extubation and reintubation, independent of etiology of extubation failure, mortality for respiratory failure increased four times when reintubation occurred> 12 h after extubation. [5] Another, similar hypothesis presumes a relationship between delay in reintubation and increased mortality. This delay allows a progressive clinical deterioration in the patients′ condition leading to organ dysfunction/failure. Though not confirmed in a recent Australian study, [10] several other studies [5],[9],[14] have reported an increase in mortality with increased time to reintubation beyond 12-24 h.
Risk Factors for Extubation Failure The risk factors for failed extubation vary depending on the population studied. Rady and colleagues [15] reported older age, preexisting left ventricular dysfunction, anemia, large transfusion requirements and renal dysfunction to be the risk factors for extubation failure in cardiac surgical population. Older age, [16] severity of illness on ICU admission, prolonged duration of ventilation before extubation [17] and the use of continuous sedation [18] have been identified as risk factors for extubation failure. Neurologic impairment was found to be an independent risk factor for extubation failure in several studies. [19],[20],[21] Pre-extubation hypercapnoea (PCO 2 ≥ 44 mmHg) due to an imbalance of respiratory load and capacity was an independent risk factor for extubation failure. [21] Frutos-Vivar [22] found that positive fluid balance in preceding 24 h led to extubation failure. Salam and colleagues [20] found that the predictive accuracy for failed extubation increased to 100% when neurologic status was considered along with adequacy of cough peak flows and volume of endotracheal secretions. In brain injured patients, Coplin and colleagues [23] found no correlation between GCS score and reintubation.
Causes of Extubation Failure
[Table - 1] lists the common causes of extubation failure, some being common to a failed spontaneous breathing trial (SBT). Causes related to airway patency and secretion may manifest only after extubation. The most common cause is respiratory failure which manifests with increased work of breathing, accessory muscle use, hypoxia and/or hypercapnea and respiratory acidosis. Another frequent reason is failure to maintain airway patency due to upper airway edema, seen in patients with prolonged translaryngeal intubation and evident as stridor. Excessive secretions, coupled with inadequate muscle strength and glottic incompetence can also cause failed extubation. Neurological impairment, due to primary illness, encephalopathy or residual effect of sedatives can necessitate reintubation. Although the most frequent cause of weaning failure is respiratory system failure, a possible consequence of the transfer from assisted to spontaneous breathing can be acute myocardial ischemia or cardiac dysfunction/failure. [24] The clinical signs presented by patients who fail a weaning trial because they develop acute heart failure (e.g., tachypnoea, tachycardia, anxiety) are often difficult to distinguish from clinical signs resulting from respiratory system failure. The time course of B-type natriuretic peptide serum concentration [25] can help to differentiate between respiratory and cardiac etiology.
Predictors of Failed Extubation A recent metaanalysis [26] found that commonly used predictors such as respiratory mechanics performed moderately when predicting successful SBT and but these predictors did even worse when extubation failure alone was studied. This may be due to the differences in pathophysiology of weaning and extubation failure. While weaning predictors identify the imbalance between respiratory capacity and load, [27] extubation failure can occur due to other causes as well. It may also be that the clinician has assessed these factors intuitively, before conducting SBT. Decisions regarding the timing of extubation are based on assessment of the patient′s capacity to protect the airway, quantity of secretions and cough strength. In this review we discuss predictors of failed extubation in patients who have successfully completed SBT.
Demographic Predictors of Extubation Failure Numerous demographic predictors have been described. Rady and colleagues, [15] in patients undergoing cardiovascular surgery, found that extubation failure was significantly more likely to occur in patients with: old age, preoperative comorbidities, need for preoperative intra-aortic balloon pump and multiple transfusions (>10 units), surgery of thoracic aorta and prolonged cardiopulmonary bypass. They suggested that patients with these factors may be excluded from routine "fast track" extubation protocol. Similar comorbidities may cause extubation failure in other ICU patients. Other demographic predictors are severity of illness at ICU admission (high APACHE II) and prolonged duration of ventilation. [17],[26] A recent trial [28] in COPD patients found that SAPS II > 35 at ICU admission and need for home ventilation predicted extubation failure. Pneumonia as reason for mechanical ventilation with unresolved infection predicted extubation failure. [22]
Predictors Assessing Respiratory -Mechanics
Most parameters of respiratory mechanics are useful only for predicting successful SBT and perform moderately or poorly with extubation prediction. We therefore present a brief discussion of these parameters.
Rapid shallow breathing index (RSBI - f/V T )
Capdevila [16] found significantly lower values of f/V T (50 ± 23 vs. 69 ± 25 breaths/min/l) in successfully extubated patients. Recently a cut off value of RSBI ≥ 57 was described [22] to separate patients who could not be extubated successfully. Epstein, [27] however, found that with f/V T < 100, 14 (of 84) patients failed extubation, 13 due to other organ system problems and suggested that f/V T was not physiologically suited to predict extubation failure. Other studies [2],[20],[29] have also reported inability of f/V T for predicting extubation outcome.
Airway occlusion pressure at 1 s (P 0.1 ) and Ratio of occlusion pressure to maximum inspiratory pressure (MIP) [P 0.1 /MIP]
P 0.1 /MIP is an index of balance between respiratory reserve and demand and reflects neuromuscular drive for breathing and it is unaffected by respiratory compliance or resistance. Capdevila and colleagues [16] reported that patients with low P 0.1 and P 0.1 /MIP failed extubation, Mergoni and colleagues [30] reported excellent prediction of success in weaning using P 0.1 /MIP, while Del Rosario [31] found similar P 0.1 /MIP values in patients with weaning success and failure. In a metaanalysis, [26] P 0.1 /MIP ratio of> 0.3 had a pooled likelihood ratio of 2.3, indicating increased chances of successful extubation. Despite excellent predictive accuracy, the role of P 0.1 /MIP ratio may be limited in most ICUs due to need for a special device.
Minute ventilation recovery time (V E RT)
Minute ventilation recovery time (V E RT) allows physiologic assessment of work imposed after SBT. Thus V E RT may identify patients with better respiratory muscle reserve, capable of sustaining spontaneous breathing following extubation. Martinez and colleagues, [2] after a 2-h SBT, placed patients back on their pre-SBT ventilator settings for up to 25 min and measured various respiratory parameters including minute ventilation (V E ) at three intervals: baseline over preceding 24 h (pre-SBT), post-trial (after SBT) and recovery (return to baseline). Patients were assumed to recover when V E decreased to 110% of the predetermined baseline. V E RT of patients with successful extubation was significantly shorter than those who failed extubation (3.6 ± 2.7 min vs. 9.6 ± 5.8 min, P < 0.011). On multivariate analysis, V E RT was an independent predictor of extubation outcome and correlated with ICU LOS ( P < 0.01). Prolonged V E RT may reflect either a limited respiratory reserve or an unrecognized, underlying disease process. Seymour and colleagues [32] evaluated a more practical method. For pre-SBT V E they collected data in three ways, a 24-h nadir (as in previous study), an 8-h average and the last V E measurement prior to SBT. They also collected data on V E RT with threshold of 100% and 110%. They found that both, the 8-h average V E and immediate pre-SBT value of V E, were in close agreement with the original method. Similarly 100% threshold for V E RT also correlated well with 110% threshold. The same group later demonstrated [33] the utility of the new method in predicting extubation success. Recently Hernandez and colleagues [34] evaluated the utility of close observation of V E during the recovery phase after the SBT. Both V E RT RT50% ∆V E (recovery time needed to reduce V E to half the difference between End-SBT- V E and basal V E ) were significantly lower in successfully extubated patients. They found that a threshold of RT50% ∆V E of seven minutes was useful to discriminate between extubation failures and successes. V E RT and derivatives appear to be promising tools, the drawback being their inability to identify patients with possible upper airway compromise.
Work of breathing (WOB)
Kirton and others [35] found that patients who fail SBT due to increased imposed work of breathing (WOB) secondary to ventilatory apparatus and endotracheal tube, but have normal physiological WOB, can be successfully extubated. The same group later showed [36] that when physiological WOB ≤0.8 J/l, patients can be successfully extubated. Automatic Tube Compensation (ATC), a form of variable pressure support, was shown [37] to improve extubation success by reducing imposed work of breathing. WOB, a promising predictor; remains confined to the research setting due to technical difficulties.
Displacement of liver/spleen
Diaphragm fatigue results in slower movement and reduced excursion. Jiang and colleagues [38] hypothesized that liver and spleen displacement during SBT can be a surrogate of diaphragmatic endurance. In 55 ICU patients, two separate observers measured the displacement of liver and spleen by ultrasonography. Patients were extubated by clinicians blinded to the study results. Patients who were successfully extubated had higher mean values. With a cutoff value of 1.1 cm, the sensitivity and specificity to predict successful extubation was 84.4% and 82.6%. This is a noninvasive test and can be done bedside, but needs expertise.
Parameters Assessing Airway Protection
Cough strength, peak expiratory flow and airway secretions
Adequate cough strength, dependent on the ability of respiratory muscles to generate pressure and flows, is important to clear airway secretions; the so-called "airway competence". This may be compromised due to unresolved pulmonary pathology, weak respiratory muscles and laryngeal dysfunction and compounded by increased resistive work due to airway inflammation and bronchospasm. Secretions may be increased due to irritation by endotracheal tube, non-infectious inflammation, lower or upper respiratory tract infection or aspiration of secretions.
Bach and Saporito [39] found that in tracheostomized patients assisted peak cough flows (PCF) were greater in those who were successfully decannulated. Khamiees and colleagues [40] evaluated the cough strength on command (0 to 5) and amount of endotracheal secretions (none to abundant) in patients passing SBT. Patients were then asked to cough onto a white card through the endotracheal tube. If secretions were propelled onto the card, it was termed a positive white card test (WCT). Patients with weak (grade 0 to 2) coughs and abundant secretions were more likely to fail extubation. Negative WCT also predicted failed extubation. In another study [20] PCF, volume of endotracheal secretions and neurologic status were evaluated after successful SBT. Patients with low PCF failed extubation and a threshold of CPF 60 l/min was a useful discriminator. Impaired neurologic status and secretion volume of> 2.5 ml/h increased the risk of extubation failure. With three risk factors 100% patients failed extubation as against 3% without any risk factors. A recent study [21] found moderate to copious secretions to be an independent predictor of extubation failure. The same group, [1] later found that patients with PEF < 60 l/min were likely to fail extubation and die in the hospital. The peak flows in these studies were much lower than Bach′s study [39] (60 l/min vs. 160 l/min) as intubated patients cannot close their glottis, limiting the pressure and flow generation. Measured cough strength is objective, inexpensive and can be done easily at the bedside and appears to be useful in predicting extubation outcome. However, this test requires patient cooperation. If the patient fails to comprehend instructions, this can lead to erroneous results, reflecting lack of cooperation rather than insufficient muscle strength. Coplin and colleagues [23] evaluated brain injured patients using a semi-quantitative airway care score (ACS) comprising six parts and assigned four points each: spontaneous cough, gag, sputum quantity, sputum viscosity, suctioning frequency and sputum character. ACS did not correlate with either success or failure of extubation. Eighty nine per cent patients with absent or weak gag and 82% patients with weak or absent cough were successfully extubated. However, they found that adequate spontaneous cough and low suctioning frequency were associated with successful extubation. Namen and colleagues [19] also did not find any relationship of presence of cough reflex and cough during suctioning and extubation failure.
Neurological dysfunction
Good mentation is essential for airway protection. The rate of reintubation was highest (33%) in patients with neurologic disease in a trial [41] examining clinical characteristics of patients undergoing weaning. In brain injured patients, [23] 24 of 136 patients required reintubation, but none due to neurological impairment. 80% of patients with GCS ≤ 8 and 91% of patients with GCS ≤ 4 were successfully extubated. There was no correlation between GCS and need for reintubation. 44 (of 117) neurosurgical patients [19] failed extubation and 22 patients needed reintubation. Patients with successful extubation had higher GCS score. A GCS ≥ 8 showed highest predictive accuracy with further improvement with increasing GCS. GCS ≥ 10 has been suggested recently [21] to be a prerequisite for successful extubation.
Parameters Assessing Airway Patency
Cuff leak test
Postextubation laryngeal edema and airway obstruction frequently leads to failed extubation. Adderley and Mullins [42] using "Qualitative cuff leak test" during a croup epidemic, found that 38% patients with absence of leak, required reintubation. The premise is that with endotracheal tube cuff deflated air leak will occur. The amount of leak depends on the degree of laryngeal and airway edema and complete absence of leak indicates very severe edema. Miller and Cole [8] used "Quantitative Cuff leak test" - average cuff leak volume during inspiration and expiration. A cuff leak volume of < 110 ml, predicted a significant risk of postextubation stridor. "Quantitative Cuff leak test" is reproducible and objective. Other studies have used similar [43] or higher [44] threshold values of cuff leak volume. Jaber and colleagues [44] used a cut-off threshold of leak 12% of expired tidal volume; while De Bast and colleagues [45] used leak threshold 15.5% of expired tidal volume. Secretions encrusted on the outer part of the endotracheal tube may reduce cuff leak volume and confound the results. It is also important to understand that though the cuff leak test predicts occurrence of post extubation stridor, it cannot predict the need for reintubation.
Laryngeal ultrasound
Ding and colleagues [46] performed a quantitative cuff leak test and bronchoscopy after a 30-min SBT. Real-time ultrasonography (US) was also done to evaluate the air-leak and the air-column width with the endotracheal cuff inflated and deflated. The air column width during cuff deflation was significantly lower in patients who developed post extubation stridor.
It is a noninvasive, reliable method, but requires skilled expert to perform the procedure.
Parameters Assessing Hemodynamics and Tissue Perfusion Change from assisted to spontaneous breathing during weaning acts as cardiovascular stress test. Patients with normal cardiac reserve increase cardiac output to meet this increased demand while patients with diminished cardiac reserve increase O 2 extraction. [47] Most predictors have been assessed with a view to weaning rather than extubation success. Grasso and colleagues [25] found evidence of acute left ventricular dysfunction in patients who failed weaning. Gastric mucosal CO 2 is a surrogate of intramucosal pH and increase in Gastric - arterial CO 2 difference (∆Pg-aCO 2 ) beyond 10 mmHg indicates inadequate splanchnic blood flow. [48] Uusaro and colleagues [29] evaluated change in ∆Pg-aCO 2 to predict extubation failure in patients with successful SBT. After stress test (spontaneous breathing at 0 pressure support), the ∆Pg-aCO2 was significantly higher in 17 patients (25%) who failed extubation. 30 patients out of 31 with ∆Pg-aCO 2 < 12 mmHg were successfully extubated. ∆Pg-aCO 2 after stress seems to be a very good predictor of likelihood of successful extubation. Patients with positive fluid balance in 24 h preceding extubation were reported [22] to need reintubation more frequently. This may represent persistent vascular permeability due to unresolved illness, however, since hemodynamic data are reported, cardiovascular insufficiency with pulmonary edema cannot be ruled out.
Management of Failed Extubation
A reasonable strategy to prevent failed extubation, if anticipated, can be continued ventilation, treatment of remediable causes of muscle weakness and excessive secretions and daily assessment for readiness to extubate, until predictors become more favorable. Delayed extubation may lead to several complications like pneumonia, increased ICU and hospital LOS, increased cost and mortality. [23] Specific therapies can be used only when the cause for failed extubation is known. If extubation failure is due to cardiac failure, adequate anti-failure with diuretics and vasodilators can be instituted and then extubation attempted. Performing tracheostomy is another option; however, the problem of removing artificial airway still remains and tracheostomy has its own complications. Only two options seem promising in failed extubation, non-invasive ventilation and prophylactic steroids.
Non-invasive ventilation
Non-invasive ventilation (NIV) is used in acute exacerbation of COPD and to prevent intubation and ventilation. It seems logical that NIV may avert reintubation after failed extubation as well. Several studies [49],[50],[51],[52] have evaluated use of NIV, with mixed results. Nava and colleagues [53] found that application of NIV immediately after extubation led to reduced reintubation rates and ICU mortality and reintubation was a strong predictor of mortality. After a prospective trial, Ferrer and colleagues [18] reported NIV to be useful for preventing reintubation and reducing mortality only in patients with hypercapnea during SBT. They suggested that NIV is likely to be useful for patients with COPD and other chronic respiratory disorders, but not in general ICU population, similar to NIV use in acute exacerbation of COPD. [54] NIV seems to be effective when used early in patients with COPD and in those who are hypercapnic during SBT.
Role of steroids
Extubation failure caused by upper airway edema is difficult to assess before extubation. Cuff leak test predicts stridor but not need for reintubation. Prophylactic use of steroids reduced reintubation rate in high risk neonates and children but not in low risk pediatric patients. [55] A Cochrane review, [56] first published in 1999 and reviewed again in 2004, showed no benefit of prophylactic steroids in adults. In a recent double blinded trial, [57] patients planned for extubation received four (20 mg) doses of methylprednisolone starting 12 h before extubation at 4h intervals or placebo. Prophylactic methylprednisolone reduced (from 22 to 3%) incidence of laryngeal edema and rate of reintubation due to (8% vs. 54%) laryngeal edema. After prolonged intubation, patients should undergo a quantitative cuff leak test when ready to be weaned. If positive, they should receive prophylactic methylprednisolone to prevent reintubation.
Conclusion Extubation failure is common in ICU and leads to increased morbidity, costs and mortality. Good mentation, competent airway, minimal secretions, good respiratory muscle strength and adequate cardiovascular reserve are essential for successful extubation. Combination of predictors may predict extubation failure accurately [20] but the results remain to be duplicated. We need to assess therapies to improve respiratory muscle strength, laryngeal competence, neurological status and secretion load and also whether these therapies improve extubation success. Simple, noninvasive predictor of cardiovascular reserve is needed, apart from other predictors. Till such predictors can be validated in general ICU population, one needs to be alert for extubation failure and intervene early to prevent further morbidity.[58]
References
| 1. | Smina M, Salam A, Khamiees M, Gada P, Yawet AA, Manthous CA. Cough peak flows and extubation outcomes. Chest 2003;124:262-8. Back to cited text no. 1 |
| 2. | Martinez A, Seymour C, Nam M. Minute ventilation recovery time: A predictor of extubation outcome. Chest 2003;123;1214-21. Back to cited text no. 2 |
| 3. | Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of mechanical ventilation. Chest 1997;112:186-92. Back to cited text no. 3 |
| 4. | Esteban A, Alνa I, Gordo F, Fernαndez R, Solsona JF, Vallverdú I, et al . Extubation outcome after spontaneous breathing trials with T-tube or pressure support ventilation. Am J Respir Crit Care Med 1997;156:459-65. Back to cited text no. 4 |
| 5. | Epstein SK, Ciubotaru RL. Independent effects of etiology of failure and time to reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med 1998;158:489-93. Back to cited text no. 5 |
| 6. | Seymour CW, Martinez A, Christie JD, Fuchs BD. The outcome of extubation failure in a community hospital intensive care unit: A cohort study. Crit Care 2004;8:R322-7. Back to cited text no. 6 |
| 7. | Torres A, Gatell JM, Aznar E, el Ebiary M, Puig DL, Gonzalez J, et al . Re-intubation increases the risk of nosocomial pneumonia in patients needing mechanical ventilation. Am J Respir Crit Care Med 1995;152:137-41. Back to cited text no. 7 |
| 8. | Miller RL, Cole RP. Association between reduced cuff leak volume and postextubation stridor. Chest 1996;110:1035-40. Back to cited text no. 8 |
| 9. | Esteban A, Frutos F, Tobin MJ, Alia I, Solsona JF, Valverdu I, et al . Comparison of four methods of weaning patients from mechanical ventilation. N Engl J Med 1995;332:345-50. Back to cited text no. 9 |
| 10. | Gowardman JR, Huntington D, Whiting J. The effect of extubation failure on outcome in a multidisciplinary Australian intensive care unit. Crit Care Resusc 2006;8:328-33. Back to cited text no. 10 |
| 11. | de Lassence A, Alberti C, Azoulay E, Le Miere E, Cheval C, Vincent F, et al . Impact of unplanned extubation and reintubation after weaning on nosocomial pneumonia risk in the intensive care unit: A prospective multicenter study. Anesthesiology 2002;97:148-56. Back to cited text no. 11 |
| 12. | Dries DJ, McGonigal MD, Malian MS, Bor BJ, Sullivan C. Protocol-driven ventilator weaning reduces use of mechanical ventilation, rate of early reintubation and ventilator-associated pneumonia. J Trauma 2004;56:943-51. Back to cited text no. 12 |
| 13. | Daley BJ, Garcia-Perez F, Ross SE. Reintubation as an outcome predictor in trauma patients. Chest 1996;110:1577-80. Back to cited text no. 13 |
| 14. | Tanios M, Nevins M, Hendra K, Allan J, Cardinal P, Epstein S. Reexamination of the effect of time to reestablishing ventilatory support on outcome for patients failing extubation. Am J Respir Crit Care Med 2001;163:A689. Back to cited text no. 14 |
| 15. | Rady MY, Ryan T. Perioperative predictors of extubation failure and the effect on clinical outcome after cardiac surgery. Crit Care Med 1999;27:340-7. Back to cited text no. 15 |
| 16. | Capdevila XJ, Perrigault PF, Perey PJ, Roustan JP, d'Athis F. Occlusion pressure and its ratio to maximum inspiratory pressure are useful predictors for successful extubation following T-piece weaning trial. Chest 1995;108:482-9. Back to cited text no. 16 |
| 17. | Lee KH, Hui KP, Chan TB, Tan WC, Lim TK. Rapid shallow breathing (frequency-tidal volume ratio) did not predict extubation outcome. Chest 1994;105:540-3. Back to cited text no. 17 |
| 18. | Ferrer M, Valencia M, Nicolas JM, Bernadich O, Badia JR, Torres A. Early noninvasive ventilation averts extubation failure in patients at risk: A randomized trial. Am J Respir Crit Care Med 2006;173:164-70. Back to cited text no. 18 |
| 19. | Namen AM, Ely EW, Tatter SB, Case LD, Lucia MA, Smith A, et al . Predictors of successful extubation in neurosurgical patients. Am J Respir Crit Care Med 2001;163:658-64. Back to cited text no. 19 |
| 20. | Salam A, Tilluckdharry L, Amoateng-Adjepong Y, Manthous CA. Neurologic status, cough, secretions and extubation outcomes. Intensive Care Med 2004;30:1334-9. Back to cited text no. 20 |
| 21. | Mokhlesi B, Tulaimat A, Gluckman TJ, Wang Y, Evans AT, Corbridge TC. Predicting extubation failure after successful completion of a spontaneous breathing trial. Respir Care 2007;52:1710-7. Back to cited text no. 21 |
| 22. | Frutos-Vivar F, Ferguson ND, Esteban A, Epstein SK, Arabi Y, Apezteguνa C, et al . Risk factors for extubation failure in patients following a successful spontaneous breathing trial. Chest 2006;130:1664-71. Back to cited text no. 22 |
| 23. | Coplin WM, Pierson DJ, Cooley KD, Newell DW, Rubenfeld GD. Implications of extubation delay in brain-injured patients meeting standard weaning criteria. Am J Respir Crit Care Med 2000;161:1530-6. Back to cited text no. 23 |
| 24. | Frazier SK, Brom H, Wiedner J. Prevalence of myocardial ischemia during mechanical ventilation and weaning and its effects on weaning success. Heart Lung 2006;35:363-73. Back to cited text no. 24 |
| 25. | Grasso S, Leone A, De Michele M, Anaclerio R, Cafarelli A, Ancona G, et al . Use of N-terminal pro-brain natriuretic peptide to detect acute cardiac dysfunction during weaning failure in difficult-to-wean patients with chronic obstructive pulmonary disease. Crit Care Med 2007;35:96-105. Back to cited text no. 25 |
| 26. | Meade M, Guyatt G, Cook D, Griffith L, Sinuff T, Kergl C, et al . Predicting success in weaning from mechanical ventilation. Chest 2001;120:400S-24S. Back to cited text no. 26 |
| 27. | Epstein SK. Etiology of extubation failure and the predictive value of the rapid shallow breathing index. Am J Respir Crit Care Med 1995;152:545-9. Back to cited text no. 27 |
| 28. | Robriquet L, Georges H, Leroy O, Devos P, D'escrivan T, Guery B. Predictors of extubation failure in patients with chronic obstructive pulmonary disease. J Crit Care 2006; 21: 185-90. Back to cited text no. 28 |
| 29. | Uusaro A, Chittock DR, Russell JA, Walley KR. Stress test and gastric-arterial PCO2 measurement improve prediction of successful extubation. Crit Care Med 2000;28:2313-9. Back to cited text no. 29 |
| 30. | Mergoni M, Costa A, Primavera S, Salvadori A, Saccani A, Zuccoli P. Assessment of various new predictive parameters of the outcome of mechanical ventilation weaning. Minerva Anestesiol 1996;62:153-64. Back to cited text no. 30 |
| 31. | Del Rosario N, Sassoon CS, Chetty KG, Gruer SE, Mahutte CK. Breathing pattern during acute respiratory failure and recovery. Eur Respir J 1997;10:2560-5. Back to cited text no. 31 |
| 32. | Seymour CW, Christie JD, Gaughan CA, Fuchs BD. Evaluation of a new method for measurement of minute ventilation recovery time. Respir Care 2006;51:133-9. Back to cited text no. 32 |
| 33. | Seymour CW, Hanson CW, Fuchs BD. Minute ventilation recovery time (V E RT) can predict extubation outcome in surgical patients. Am J Respir Crit Care Med 2002;:A687. Back to cited text no. 33 |
| 34. | Hernandez G, Fernandez R, Luzon E, Cuena R, Montejo JC. The early phase of the minute ventilation recovery curve predicts extubation failure better than the minute ventilation recovery time. Chest 2007;131:1315-22. Back to cited text no. 34 |
| 35. | Kirton OC, DeHaven B, Morgan JP, Windsor J, Civetta JM. Elevated imposed work of breathing masquerading as ventilator weaning intolerance. Chest 1995;108:1021-5. Back to cited text no. 35 |
| 36. | DeHaven CB, Kirton OC, Morgan JP, Hart AM, Shatz DV, Civetta JM. Breathing measurement reduces false-negative classification of tachypneic preextubation trial failures. Crit Care Med 1996;24:976-80. Back to cited text no. 36 |
| 37. | Cohen JD, Shapiro M, Grozovski E, Lev S, Fisher H, Singer P. Extubation outcome following a spontaneous breathing trial with automatic tube compensation versus continuous positive airway pressure. Crit Care Med 2006;34:682-6. Back to cited text no. 37 |
| 38. | Jiang JR, Tsai TH, Jerng JS, Yu CJ, Wu HD, Yang PC. Ultrasonographic evaluation of liver/spleen movements and extubation outcome. Chest 2004;126:179-85. Back to cited text no. 38 |
| 39. | Bach JR, Saporito LR. Criteria for extubation and tracheostomy tube removal for patients with ventilatory failure: A different approach to weaning. Chest 1996;110:1566-71. Back to cited text no. 39 |
| 40. | Khamiees M, Raju P, DeGirolamo A, Amoateng-Adjepong Y, Manthous CA. Predictors of extubation outcome in patients who have successfully completed a spontaneous breathing trial. Chest 2001;120:1262-70. Back to cited text no. 40 |
| 41. | Vallverdu I, Calaf N, Subirana M, Net A, Benito S, Mancebo J. Clinical characteristics, respiratory functional parameters and outcome of a 2-hour t-piece trial in patients weaning from mechanical ventilation. Am J Respir Crit Care Med 1999;159:512-8. Back to cited text no. 41 |
| 42. | Adderley RJ, Mullins GC. When to extubate the croup patient: The "leak" test. Can J Anaesth 1987;34:304-6. Back to cited text no. 42 |
| 43. | Kriner EJ, Shafazand S, Colice GL. The endotracheal tube cuff-leak test as a predictor for postextubation stridor. Respir Care 2005;50:1632-8. Back to cited text no. 43 |
| 44. | Jaber S, Chanques G, Matecki S, Ramonatxo M, Vergne C, Souche B, et al . Post-extubation stridor in intensive care unit patients: Risk factors evaluation and importance of the cuff-leak test. Intensive Care Med 2003;29:69-74. Back to cited text no. 44 |
| 45. | De Bast Y, De Backer D, Moraine JJ, Lemaire M, Vandenborght C, Vincent JL. The cuff leak test to predict failure of tracheal extubation for laryngeal edema. Intensive Care Med 2002;28:1267-72. Back to cited text no. 45 |
| 46. | Ding LW, Wang HC, Wu HD, Chang CJ, Yang PC. Laryngeal ultrasound: A useful method in predicting post-extubation stridor: A pilot study. Eur Respir J 2006;27:384-9. Back to cited text no. 46 |
| 47. | De Backer D, El Haddad P, Preiser JC, Vincent JL. Hemodynamic responses to successful weaning from mechanical ventilation after cardiovascular surgery. Intensive Care Med 2000;26:1201-6. Back to cited text no. 47 |
| 48. | Mohsenifar Z, Hay A, Hay J, Lewis MI, Koerner SK. Gastric intramural pH as a predictor of success or failure in weaning patients from mechanical ventilation. Ann Intern Med 1993;119:794-8. Back to cited text no. 48 |
| 49. | Kilger E, Briegel J, Haller M, Frey L, Schelling G, Stoll C, et al . Effects of noninvasive positive pressure ventilatory support in non-COPD patients with acute respiratory insufficiency after early extubation. Intensive Care Med 1999;25:1374-80. Back to cited text no. 49 |
| 50. | Jiang JS, Kao SJ, Wang SN. Effect of early application of biphasic positive airway pressure on the outcome of extubation in ventilator weaning. Respirology 1999;4:161-5. Back to cited text no. 50 |
| 51. | Keenan SP, Powers C, McCormack DG, Block G. Noninvasive positive-pressure ventilation for postextubation respiratory distress: A randomized controlled tria trial. JAMA 2002;287:3238-44. Back to cited text no. 51 |
| 52. | Esteban A, Frutos-Vivar F, Ferguson ND, Arabi Y, Apezteguνa C, Gonzαlez M, et al . Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med 2004;350:2452-60. Back to cited text no. 52 |
| 53. | Nava S, Gregoretti C, Fanfulla F, Squadrone E, Grassi M, Carlucci A, et al . Noninvasive ventilation to prevent respiratory failure after extubation in high-risk patients. Crit Care Med 2005;33:2465-70. Back to cited text no. 53 |
| 54. | Caples SM, Gay PC. Noninvasive positive pressure ventilation in the intensive care unit: A concise review. Crit Care Med 2005;33:2651-8. Back to cited text no. 54 |
| 55. | Lukkassen MA, Markhorst DG. Does dexamethasone reduce the risk of extubation failure in ventilated children. Arch Dis Child 2006;91:791-3. Back to cited text no. 55 |
| 56. | Markovitz BP, Randolph AG. Corticosteroids for the prevention and treatment of post-extubation stridor in neonates, children and adults. Cochrane Database Syst Rev 2000;2:CD001000. Back to cited text no. 56 |
| 57. | Franηois B, Bellissant E, Gissot V, Desachy A, Normand S, Boulain T, et al . 12-h pretreatment with methylprednisolone versus placebo for prevention of postextubation laryngeal oedema: A randomised double-blind trial. Lancet 2007;369:1083-9. Back to cited text no. 57 |
| 58. | Esteban A, Alνa I, Tobin MJ, Gil A, Gordo F, Vallverdú I, et al . Effect of spontaneous breathing trial duration on outcome of attempts to discontinue mechanical ventilation. Am J Respir Crit Care Med 1999;159: 512-8. Back to cited text no. 58 |
Copyright 2008 - Indian Journal of Critical Care Medicine
The following images related to this document are available:
Photo images
[cm08001t1.jpg]
|

{kind=link}