 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
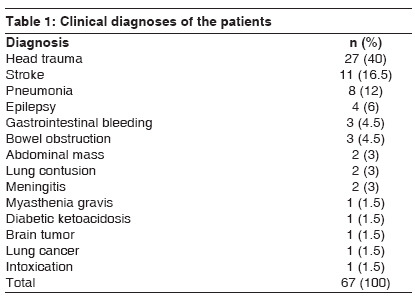
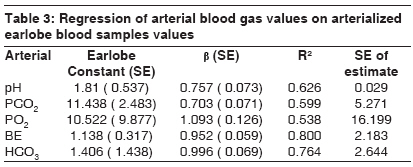
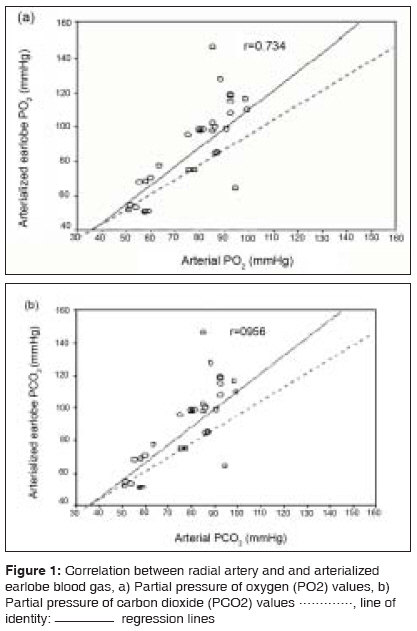
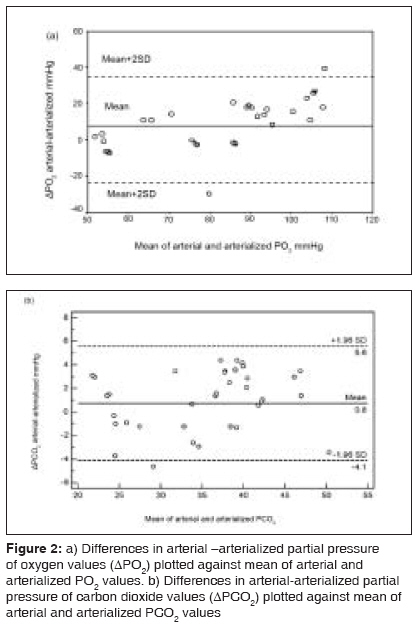
Indian Journal of Critical Care Medicine, Vol. 12, No. 3, July-September, 2008, pp. 96-101 Research Article Prediction of arterial blood gas values from arterialized earlobe blood gas values in patients treated with mechanical ventilation Honarmand Azim, Safavi Mohammadreza Department of Anaesthesiology and Intensive Care, Isfahan University of Medical Sciences, Isfahan Code Number: cm08021 Abstract Background/Objective: Arterial blood gas (ABG) analysis is useful in evaluation of the clinical condition of critically ill patients; however, arterial puncture or insertion of an arterial catheter may sometimes be difficult and cause many complications. Arterialized ear lobe blood samples have been described as adequate to gauge gas exchange in acute and chronically ill pediatric patients.Purpose: This study evaluates whether pH, partial pressure of oxygen (PO 2 ), partial pressure of carbon dioxide (PCO 2 ), base excess (BE), and bicarbonate (HCO 3 ) values of arterialized earlobe blood samples could accurately predict their arterial blood gas analogs for adult patients treated by mechanical ventilation in an intensive care unit (ICU). Setting: A prospective descriptive study Methods: Sixty-seven patients who were admitted to ICU and treated with mechanical ventilation were included in this study. Blood samples were drawn simultaneously from the radial artery and arterialized earlobe of each patient. Results: Regression equations and mean percentage-difference equations were derived to predict arterial pH, PCO 2 , PO 2 , BE, and HCO 3 -values from their earlobe analogs. pH, PCO 2 , BE, and HCO 3 all significantly correlated in ABG and earlobe values. In spite of a highly significant correlation, the limits of agreement between the two methods were wide for PO 2 . Regression equations for prediction of pH, PCO 2 , BE, and HCO3- values were: arterial pH (pHa) = 1.81+ 0.76 x earlobe pH (pHe) [r = 0.791, P < 0.001]; PaCO 2 = 1.224+ 1.058 x earlobePCO 2 (PeCO 2 ) [r = 0.956, P < 0.001]; arterial BE (BEa) = 1.14+ 0.95 x earlobe BE (BEe) [r= 0.894, P < 0.001], and arterial HCO 3 - (HCO 3 -a) = 1.41+ earlobe HCO 3 (HCO 3 -e) [r = 0.874, P < 0.001]. The predicted ABG values from the mean percentage-difference equations were derived as follows: pHa = pHe × 1.001; PaCO 2 = PeCO 2 × 0.33; BEa = BEe × 0.57; and HCO 3 -a = HCO 3 -e × 1.06. Conclusions: Arterialized earlobe blood gas can accurately predict the ABG values of pH, PCO 2 , BE, and HCO 3 - for patients who do not require regular continuous blood pressure measurements and close monitoring of arterial PO 2 measurements. Keywords: Arterialized earlobe blood gas, critically illness, mechanical ventilation Introduction Measurement of arterial blood gas tensions is routinely used to assess gas exchange in patients with acute and chronic respiratory disorders. Arterial blood gas (ABG) sampling represents the gold standard method for acquiring patients′ acid-base status. The most common complications associated with arterial puncture are pain, arterial injury, aneurysm formation, hemorrhage, and thrombosis with distal ischaemia. The risks increase with repeated arterial punctures, especially with insertion of a catheter when performed by inexperienced individuals. [1] Additionally, this procedure carries a small but appreciable risk of needle stick injury to health care workers, with the consequent risk of transmission of blood borne viruses such as hepatitis C and human immunodeficiency virus (HIV). [2] In the 1960s, it was proposed that blood gas values could be measured using arterialized earlobe blood samples. [3] Arterialized ear lobe blood gas samplings are easier to obtain and a less invasive way of evaluating acid-base status in intensive care unit. It avoids the risks of arterial punctures. It is based on the assumption that provided sufficient vasodilatation can be achieved locally by means of topical application of a vaso-active cream on the earlobe, the arterialized earlobe oxygen tension resembles the arterial oxygen tension due to convergence of arterial and venous oxygen tension. [4] Techniques for sampling arterialized capillary blood from the finger pulp and the earlobe were first described over two decades ago but, although close agreement between arterial values and earlobe samples has been demonstrated in normal subjects, this technique is not in common usage. The main reasons for this appear to be lack of knowledge of its existence and uncertainty over its accuracy. [5] Initial [3],[6],[7] or more recent [5] studies have concluded that the earlobe method might be accurate enough to replace arterial blood samples for clinical purposes. This opinion is based mainly on positive and strong correlations that have been found between the two methods. However, most investigators have sought correlation using simple regression analysis instead of the method of BLAND and ALTMAN. [8] This approach has probably rendered the conclusion of most studies flawed by statistical bias. In fact, two recent studies using BLAND and ALTMAN [8] analysis have stated that arterialized earlobe PO 2 often underestimates arterial PO 2 , therefore making this method unsuitable for clinical assessment. [9],[10] Several studies have shown good correlation between capillary blood, venous blood, and arterial blood gas values in pediatric intensive care units. [11],[12],[13] However, arterialized earlobe oxygen tension often underestimates arterial oxygen tension [4] and is not fully validated in adult patients with acute respiratory failure receiving mechanical ventilation. The purpose of this study was to investigate the correlation between simultaneous arterial blood gas and arterialized earlobe blood samples and to establish whether pH, partial pressure of oxygen (PO 2 ), partial pressure of carbon dioxide (PCO 2 ), base excess (BE), and bicarbonate (HCO 3 -) values of arterialized earlobe blood samples could accurately predict their arterial blood gas analogs for patients with acute respiratory failure treated by mechanical ventilation in an intensive care unit (ICU).Materials and Methods Sixty seven patients with acute respiratory failure who were admitted to a multidisciplinary adult intensive care unit between May 2005 and August 2005 receiving mechanical ventilation, were enrolled in this prospective descriptive study. The study protocol was approved by the local institutional ethics committee, and written informed consent was obtained from each patient or his or her family. Patients with hypotension (systolic blood pressure less than or equal to 90 mm Hg), hypertension (systolic pressure above 140 with a diastolic pressure above 90), hypothermia (axillary temperature < 36°C), and hyperthermia (axillary temperature> 38°C), severe sepsis, multiorgan failure, or chronic lung disease were excluded from the study. No patient was in cardiovascular shock. Blood samples were drawn simultaneously from the radial artery and the arterialized earlobe of each patient in a sitting position. Blood gases were obtained if the patient needed blood gases for clinical decisions. All patients were receiving mechanical ventilation for 48h or more with a fraction of inspired oxygen (FiO 2 ) of 0.5 or less and positive end-expiratory pressure of 5 cm H 2 O. Arterial samples Earlobe samples Statistical methods Results Sixty-seven consecutive adult patients were studied. Blood samples were drawn simultaneously from arterialized earlobe and radial artery. Admission diagnoses included head trauma, abdominal mass, gastrointestinal bleeding, lung contusion, bowel obstruction, myasthenia gravis, epilepsy, pneumonia, meningitis, diabetic ketoacidosis, stroke, brain tumor, lung cancer, and intoxication [Table - 1]. The mean (SD) age of the patients was 47.57 (19.51). Fifty (74.6%) were males and 17 (25.4%) were females. No complication in the drawing of blood samples was observed with either method. pH, PCO2, BE, and HCO3 were all significantly correlated in ABG and earlobe samples [Table - 2] and [Table - 3]. The range of arterial PO2 values was 6.8-19.5 kPa (51.1-146.5mmHg), mean 11.3 kPa (84.77mmHg). The range and mean of arterial PCO 2 values was 3.01-6.5 kPa (22.6-48.6 mmHg) and 4.7 kPa (35.08 mmHg) respectively. The relationships between arterial and earlobe samples for PO 2 and PCO2 are shown in [Figure 1a] and [Figure 1b]. The correlation coefficients were 0.734 (P< 0.0001) and 0.956 (P< 0.0001) respectively. Despite this highly significant correlation, regression lines were slightly different from lines of identity, particularly for PO 2 . In [Figure 2a] and [Figure 2b], differences between the two methods (arterial - arterialized values) were plotted against means of arterial and arterialized PO 2 PO 2 or PCO 2 . The mean (bias) ±SD and the range of the differences, as well as the 95% confidence intervals for the lower and upper limit of agreement were reported in [Table - 4]. Arterialized earlobe PO 2 was lower than arterial PO 2 in most cases, and the difference increased as the arterial PO 2 increased. These results show that the limits of agreement for PO 2 were wide, reveal a lack of agreement between the two methods. For PCO 2 , on the other hand, the mean difference between the two methods was close to zero, and the limits of agreement were narrower. Regression equations for prediction of pH, PCO 2 ,, BE, and HCO 3 - values were: arterial pH (pHa) = 1.81+ 0.76 x earlobe pH (pHe) [r = 0.791, P < 0.001]; PCO 2 , = 1.224+ 1.06 x earlobe PCO 2 , (PeCO 2 ) [r = 0.956, P < 0.001]; arterial BE (BEa) = 1.14+ 0.95 x earlobe BE (BEe) [r= 0.894, P < 0.001], and arterial HCO 3 - (HCO 3 -a) = 1.41+ earlobe HCO 3 (HCO 3 -e) [r = 0.874, P < 0.001]. The predicted ABG values from the mean percentage-difference equations were derived as follows: pHa = pHe x 1.001; PCO 2 , = PeCO 2 x 0.33; BEa = BEe x 0.57; and HCO 3 -a = HCO 3 -e x 1.06.Discussion Acid-base analysis is essential for management of patients in ICU, yielding valuable information about a variety of disease processes. [1],[12],[14] Non-invasive methods, such as pulse oximetry, transcutaneous monitoring of oxygen and carbon dioxide, and end tidal carbon dioxide have been proven to be useful, [1] but they do not give information about pH, PO 2 , BE and bicarbonate. Arterial blood gases are frequently determined in the ICU. This is, however, an invasive way of monitoring blood gas and there are complications, mostly local hematoma related to arterial puncture. The procedure itself is technically difficult and painful. Arterial lines are usually placed in unstable patients in the ICU who need close monitoring of PO2. When an arterial line is not in place, arterial or venous blood gas (VBG) values continue to be obtained and used for clinical monitoring and management decisions. Earlobe blood gas sampling is a less invasive way of evaluating acid-base status in a well perfused patient. If a blood gas value determined by earlobe samples could be used to show patients′ acid-base status and guide their management with the same accuracy as arterial sampling, this would be preferable because of ease of blood sample collection. For many years, clinicians have been looking for alternatives to ABG sampling in both children and adults, and studies have investigated ABG, VBG, and capillary (CBG) blood gas samples and the correlation between the values. [15],[16],[17] Numerous studies published many years ago concluded that the method using arterialized earlobe blood for PO 2 and PCO 2 analysis was accurate enough to replace arterial blood samples for clinical purposes. [3],[6],[7],[18],[19],[20] However, the validity of this method has been discussed in two studies, [9],[10] showing with the analysis of BLAND and ALTMAN, [8] PO 2 was usually lower in earlobe than in arterial blood, and that the limits of agreement were wide between the two methods. Studies comparing ABG and CBG, ABG and VBG samples in diabetic ketoacidosis, and ABG-CBG blood gases values in stable pediatric intensive care unit patients have shown good correlation among ABG, VBG, and CBG samples. [13] However, there have been no studies comparing simultaneously obtained ABG and earlobe samplings in stable adult ICU patients treated by mechanical ventilation. We studied sixty-seven simultaneously obtained arterial blood gas and arterialized earlobe blood samples of patients and showed pH, PCO 2 , BE, HCO 3 were all correlated in arterial and earlobe blood gases in normotensive and normothermic patients. Although there was a significant correlation for PO 2 in these patients, it was lower. Sauty et al, compared arterial and arterialized earlobe blood samples in 115 consecutive adult patients and concluded that, in adult patients, arterialized earlobe blood PO 2 is not a reliable mirror of arterial PO 2 . [9] The main cause of underestimation of arterial PO 2 in earlobe samples is insufficient arterialization of blood, corresponding to a certain venous admixture. The effect of a given venous admixture in earlobe blood depends on the arterio-venous PO 2 difference: the larger the arterio-venous PO 2 difference, the wider the discrepancy between earlobe and arterial PO 2 . This is one likely reason for the unreliable PO 2 values measured in arterialized earlobe blood in patients breathing 100% oxygen. [19],[21],[22] Because the arterio-venous PO 2 difference is large in subjects with normal arterial PO 2 , a small venous admixture in earlobe blood will result in a greater discrepancy between earlobe and arterial PO 2 . Our data supports this observation. It must be emphasized that in our study, there was no patient with severe sepsis, multiorgan failure, cardiovascular shock, or chronic lung disease because inclusion of these patients might have caused poorer correlation between ear and arterial PO 2 values due to venous admixture. Indeed, [Figure 2a] shows that arterial PO 2 , when in the normal range, was often markedly underestimated by the earlobe sample. Interestingly and despite fewer normal PO 2 values, the study of PITKIN et al, [5] also showed a trend towards increased difference between arterial and arterialized PO 2 with increasing mean PO 2 values. Accordingly, and as reported by the same authors, we observed a better agreement between the two methods for arterial PO 2 values lower than 8.0 kPa (60 mmHg), where the effect of venous admixture is smaller. On the other hand, there was a good agreement between earlobe and arterial values of PCO 2 , as previously reported. [5] This reflects the insignificant effect of venous admixture, due to the comparatively smaller arterio-venous PCO 2 difference. The usefulness of each method should be weighed according to its advantages and inconveniences. The advocated advantages of the earlobe method are that it is safe and can be performed by non-medical staff. [23] However, as the collection of an earlobe blood sample must be fully aseptic, [6] the method requires trained personnel. Although complications of arterial punctures have been described, [24] complications of radial arterial punctures are extremely low and in our experience none were observed in the present experiment. In conclusion, we showed a good correlation in pH, PCO 2 , BE, and HCO 3 between simultaneous samples of arterialized earlobe and arterial blood in normotensive and normothermic patients receiving mechanical ventilation. So, earlobe blood gas measurements may be useful alternatives to arterial blood gas samples for critically ill patients who do not require regular continuous blood pressure measurements and close monitoring of arterial PO 2 measurements. We do not recommend arterialized earlobe blood samples for determining PO 2 of arterial blood gas samples. References
Copyright 2008 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm08021t4.jpg] [cm08021t1.jpg] [cm08021f1.jpg] [cm08021f2.jpg] [cm08021t3.jpg] [cm08021t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}