 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
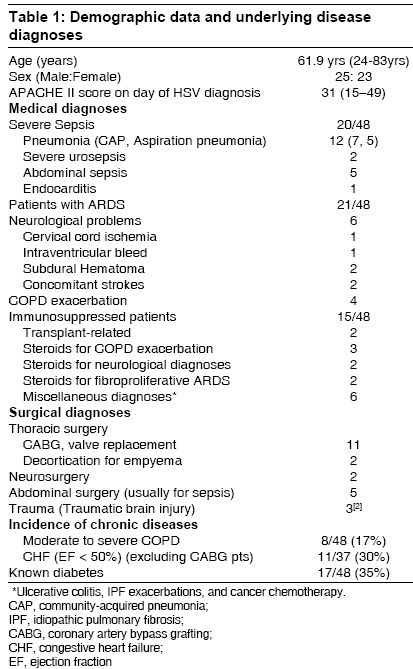
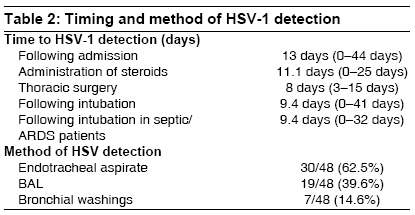
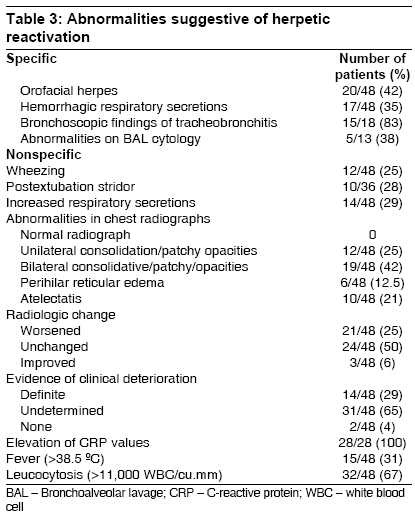
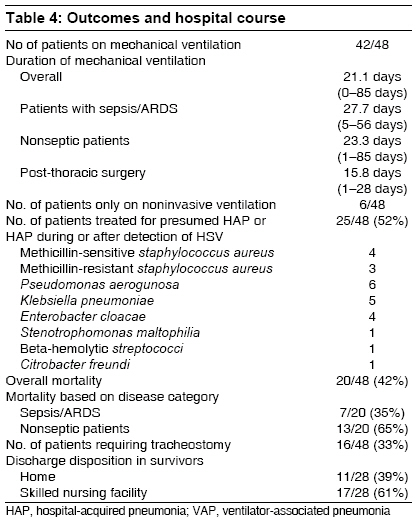
Indian Journal of Critical Care Medicine, Vol. 12, No. 4, October-December, 2008, pp. 145-152 Original Article Clinical course and spectrum of intensive care unit patients reactivating herpes simplex-1 virus: A retrospective analysis Sundar KrishnaM, Ludwig KarlA, Alward WilliamT, Pearce MichaelJ, Bishop ClarkT, Hammond RoyC, Hillyard DavidR, Freestone StevenW, Ozment Anne, Cahill BarbaraC Department of Medicine, Utah Valley Regional Medical Center, Provo;Department of Medicine, University of Utah Medical Center, Salt Lake City, Utah Code Number: cm08030 Abstract Background : Herpes simplex-1 virus (HSV-1) reactivation in the respiratory tract is common in intensive care unit (ICU) patients. However, susceptible ICU populations are poorly defined. Clinical recognition of HSV infection of the respiratory tract is difficult and the impact of such reactivation is not understood.Materials and Methods : A retrospective analysis of HSV-1 positive patients encountered over a 5-year period at a multispecialty ICU was carried out. HSV-1 was identified in respiratory secretions using a qualitative polymerase chain reaction (PCR) technique. Patient charts were reviewed for clinical features that would typify HSV-1 respiratory involvement, and the morbidity and mortality risks found with HSV-1 respiratory involvement. Results : A review of 48 HSV-1 positive ICU patients showed that patients reactivating HSV in the respiratory tract fell into one of the three categories: (1) septic elderly patients with and without ARDS, (2) immunosuppressed patients, especially those receiving high-dose steroids, and (3) post-thoracotomy patients. Abnormalities suggestive of HSV-1 reactivation in the respiratory tract included, haemorrhagic or excessive respiratory secretions, concomitant orofacial herpes (42%), and bronchoscopic abnormalities (hemorrhagic ulcers and mucosal friability) (83%). Twenty eight percent of the HSV-1 infected patients experienced postextubation stridor. HSV-1 reactivation was associated with extended ventilator stays, significant mortality (42%), and ventilator-associated pneumonias (52%). Conclusions : Identification of susceptible populations and definition of clinical features of HSV-1 related respiratory disease can enable diagnosis of HSV-1 infection in ICU patients. Although detection by a PCR technique can rapidly diagnose HSV-1 reactivation, prospective studies are required to clarify HSV disease versus mere shedding, and understand the impact of HSV-1 reactivation in hospitalized patients. Keywords: Herpes simplex-1 virus, pneumonia, viral, ventilator associated Introduction The viruses from the herpes family are characterized by their ability to remain latent within tissues following initial infection and a tendency to reactivate at mucocutaneous sites. [1] Reactivation of herpes simplex-1 virus (HSV-1) in the orofacial region is a common problem; other sites of herpetic infection include the respiratory tract and gastrointestinal tract. [1] HSV-1 reactivation pneumonitis and esophagitis are well recognized in immunosuppressed patients. [2] However, a number of critically ill and hospitalized patients also develop herpetic infection in the respiratory tract that is infrequently recognized. This study was carried out to identify circumstances in which herpetic reactivation occurs in ICU patients, recognize patterns of respiratory disease, and evaluate the clinical impact of such reactivation.Materials and Methods Hospital records from ICU patients who tested positive for HSV-1 in their respiratory secretions between 2003 and 2007 were reviewed. HSV in sputum, endotracheal aspirate, bronchoscopic aspirates, and lavage fluid (BAL) was identified with a polymerase chain reaction (PCR) method using the Nanogen MGB Alert HSV 1, 2 qualitative assay (Nanogen Inc., Wothell, WA, USA). This PCR method has been validated for HSV-1 and HSV-2 detection in a variety of sample types including respiratory secretions. [3] This assay targets a 179-bp region from the glycoprotein D gene and utilizes UTP/UNG contamination control and hybridization probe chemistry allowing for post PCR melting analysis and accommodation of sequence polymorphisms. It also employs a noncompetitive internal control in every sample PCR to monitor for extraction efficiency and potential PCR inhibition. [3] Clinical samples are extracted using the QIAGEN 96-well blood kit, with minor modifications to optimize extraction efficiency. The test was performed in a closed-tube format using a standard-master mix kit (Roche Molecular Biochemicals, Indianapolis, Indiana, USA) and has an analytic sensitivity of approximately 400 HSV genomes per milliliter of clinical fluid [3] . Since this assay does not distinguish between HSV1 and HSV2, further references to HSV detection in respiratory secretions will be meant to imply HSV1 detection. HSV2 infections in the respiratory tract have been reported very rarely in the existing literature. [4] In patients screened for HSV-1 in the respiratory tract, no apriori testing algorithms were used. In fact, no specific recommendations exist for HSV-1 screening except in instances of suspicion of herpetic tracheobronchitis. [5] Previous reports indicate that herpetic tracheobronchitis can be suspected during bronchoscopy when the findings of hemorrhagic mucosal ulcers are encountered. [5] Many patients in this study however lacked the classic bronchoscopic features and manifested a spectrum of clinicoradiologic abnormalities. Among patients with HSV-1 in respiratory secretions, data was reviewed for demographic information, underlying medical diagnoses, time to HSV diagnosis, bronchoscopic findings, concomitant infections, hospital course, and outcome. Attempt was made to identify diseases or interventions that may have predisposed patients to herpetic reactivation. Charts were reviewed for specific mention of orofacial lesions, appearance of respiratory secretions, and chest auscultatory findings. Chest X-ray findings during diagnosis of HSV infection were reviewed by a radiologist (RCH) blinded to clinical information on individual patients. Medical diagnoses were obtained from chart descriptors and review. Particular attention was paid to the reasons for ICU stay during the week prior to HSV positivity in respiratory secretions as many patients had multiple comorbidities and prolonged ICU stays. The diagnoses of acute respiratory distress syndrome (ARDS), severe sepsis, and ventilator-associated pneumonia (VAP), were made based on accepted practice standards [Appendix I]. In a number of patients, bronchoscopy was performed and the description of airway abnormalities and available cytological specimens reviewed. BAL was performed with instillation and aspiration of 2-3 aliquots of 60 cc of normal saline in a wedged lung segment of interest. In patients with suspected nosocomial pneumonia, BAL was sent for Gram stain, quantitative bacterial cultures, and HSV PCR. Approval from Intermountain Health Care institutional review board was obtained for conducting this study. The need for informed consent from patients was waived by the review board due to lack of any patient identifiers. Results All patients with HSV-1 in respiratory secretions diagnosed by qualitative PCR over a five-year period at a tertiary-level multispecialty ICU were analyzed. Between 2003 and 2007, 56% (46/88) of sputum specimens, 31.3% (30/96) of BAL specimens, and 3.3% (7/23) of bronchial washings at the Utah Valley Regional Medical Center yielded HSV by PCR. Of these, 48 HSV-1 positive patients from surgical, medical, and coronary ICUs were identified. All, but two patients were Caucasians. A majority of patients testing positive for HSV were elderly, critically ill, and septic [Table - 1]. Unlike previous reports of an increased association in smokers, [6] only 8/48 patients had a smoking history or documented COPD. After excluding patients undergoing cardiac surgery, 11/37 patients had underlying cardiac illnesses, mostly congestive heart failure. Although 85% of the patients were on insulin infusions for tight blood glucose control during their ICU stay, only 17 patients had preexisting diabetes mellitus. The three most common associations for a positive HSV PCR were critical illness (20 patients), steroid use (13 patients), and thoracotomy for coronary artery bypass grafting (CABG) or valve surgery (11 patients) [Table - 1]. HSV was identified an average of 13 days after hospitalization, and in intubated patients, after nine days of mechanical ventilation [Table - 2]. HSV was detected in respiratory secretions after a mean duration of 11 days of steroid initiation and eight days after thoracotomy [Table - 2]. HSV was most often detected in sputum obtained through endotracheal aspiration (30/48 patients) or from BAL samples (19/48 patients). Testing from multiple respiratory sources was done in seven patients [Table - 2]. [Table - 3] details clinical findings associated with the presence of HSV in respiratory secretions. 20/48 (42%) of the patients developed orofacial herpes. Of the 18 patients who underwent bronchoscopy, 15 (83%) had findings of tracheobronchial ulcers, erythematous mucosa, and mucosal friability. Cytopathological examination of BAL specimens showed characteristic herpetic inclusions in only 38% of the specimens available for review. A number of patients had either hemorrhagic respiratory secretions (17/48) or excessive sputum production (14/48). Wheezing was found in 25% of the patients and 10 patients were noted to have postextubation stridor for which noninvasive ventilation and/or steroids were used. On posthoc review of serial chest radiographs, most patients had either unchanged or worsened chest X-rays on the day of HSV detection. In 29% of patients, definite clinical deterioration was noted during the time of HSV detection; but in the majority, HSV-1 positive patients were significantly ill from underlying morbidities that precluded an accurate assessment of definitive clinical changes. Of the 48 HSV positive patients, 25 developed nosocomial pneumonia (ventilator-associated pneumonia 23, hospital acquired pneumonia 2) [Table - 4]. Causative organisms included both Gram positive and Gram-negative bacteria [Table - 4]. The mortality rate was high in patients with HSV, despite specific treatment of herpes simplex and concomitant infections [Table - 4]. All patients were treated with intravenous acyclovir at a dose of 5 mg/kg given 2-3 times a day based on their renal function. Although a number of patients had evidence of clinical or radiologic deterioration that improved with antiviral therapy, withdrawal of life support in a number of cases made it difficult to compare mortality rates among HSV-positive groups. The duration of mechanical ventilation in HSV-positive patients was much longer than the average length of stay on the ventilator in our institution (9.3 days for ARDS patients in the year 2007). Post-thoracotomy patients with HSV-1 isolated from respiratory secretions had longer ventilator days as compared to our institutional average (time to first extubation < 10 hours in 2007). Thirty three percent of HSV-1 positive patients required tracheostomy and 61% required placement in a skilled nursing facility following hospital discharge [Table - 4]. Discussion In humans, HSV-1 infection is characterized by latent infection in the sensory ganglia of cranial nerves with reactivation under conditions of stress. [1] Stressors that lead to reactivation range from local trauma (dental procedures, sunburn, trigeminal nerve root decompression, etc.) to systemic immunosuppression that especially affects the T-cell immunity (organ or marrow transplantation, HIV infection). [1] Following oropharyngeal reactivation, seeding of the virus into the respiratory and gastrointestinal tract can occur and the potential for herpetic tracheobronchitis and esophagitis exists. However, secondary infections in the respiratory and gastrointestinal tract are reported very infrequently in immunocompetent patients, and visceral disease is not commonly recognized in immunocompetent patients with orofacial herpes. In the last few decades, a number of reports have highlighted the occurrence of herpetic visceral infections, especially herpetic bronchopneumonitis in relatively nonimmunosuppressed populations. Pulmonary HSV infections were initially recognized in patients with burns [7],[8] and allogeneic transplants. [2] A seminal study by Tuxen et al, showed that patients with ARDS who tested positive for HSV showed both an increase in duration of ventilatory support and late mortality. [9] Further studies have shown HSV reactivation in patients undergoing thoracotomy [10],[11] and in patients with critical illness. [12],[13] Critically ill populations that reactivate HSV not only include medically ill septic patients but also surgical and trauma patients. [14],[15] One of these studies in critically ill patients established that HSV infection encountered in the ICU occurs due to reactivation of latent virus residing in sensory cranial nerve ganglia rather than from new infection acquired nosocomially. [13] This finding of HSV reactivation in critically ill patients has been explored to understand its impact on outcomes in bigger studies, however, a mortality effect has not been clearly demonstrable. [16],[17] The use of highly sensitive PCR technique has also revolutionized the diagnosis of viral infections, especially HSV1 infections. PCR increases the detection rate of HSV-1 by 44% when compared to the cumbersome culture technique. [18] In addition, PCR is inexpensive and results can be obtained quickly. [3],[18] The identification of HSV1 by PCR in the lung, however, may denote lower respiratory tract infection or contamination from oropharyngeal or orofacial herpetic reactivation. Quantitative BAL PCR has been recommended to distinguish herpetic bronchopneumonitis from upper airway contamination; [16],[19] however, viral loads that accurately discriminate between contamination and infection are not defined. The full spectrum of HSV infection of the lower respiratory tract remains to be established. Although initial studies emphasized tracheobronchitis as the main manifestation of herpetic infection, [5],[8] a spectrum of abnormalities have been described, ranging from asymptomatic shedding from viral activation in the ninth and tenth cranial nerves, [20] pneumonia, [2],[8],[11],[15] tracheal stenosis, [21] and an effect on lung capillary permeability. [22] This study aimed to identify ICU populations susceptible to herpetic reactivation, to define patterns of HSV respiratory disease, and to understand the impact of HSV disease on hospital course and coinfections. Susceptible populations for HSV infection Apart from surgical trauma due to thoracotomy, steroid therapy appears to be an important trigger for herpetic reactivation. [13],[16] Although many patients received empiric stress-dose steroids for management of septic shock, most with HSV reactivation had received higher steroid doses (>0.5 mg/kg/day of prednisone) given for reasons other than adrenal dysfunction. Given the number of hospitalized patients who receive significant doses of steroids for a variety of problems, reports of serious herpetic disease are rare. [25],[26] Patterns of HSV infection Role of cytological diagnosis Impact of HSV infection Study limitations Conclusion Identification of HSV in respiratory secretions has been vastly improved by the increased availability of PCR that can detect HSV1 in all types of respiratory specimens. The convenience and rapidity of the PCR technique allows early detection in susceptible populations - critically ill, septic patients with lung injury who often require prolonged mechanical ventilation. Steroid use and post-thoracotomy patients may be particularly at risk. Even though detection of HSV has been improved, the separation of mere shedding from disease is clinically challenging. Future studies are required to determine the extent of testing that is required to differentiate bronchial shedding or contamination from upper respiratory tract reactivation versus true herpetic bronchopneumonitis.Acknowledgments Dr Nathan Dean, Dr Terry Clemmer[32]References
Copyright 2008 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm08030t2.jpg] [cm08030t1.jpg] [cm08030t4.jpg] [cm08030t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}