 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
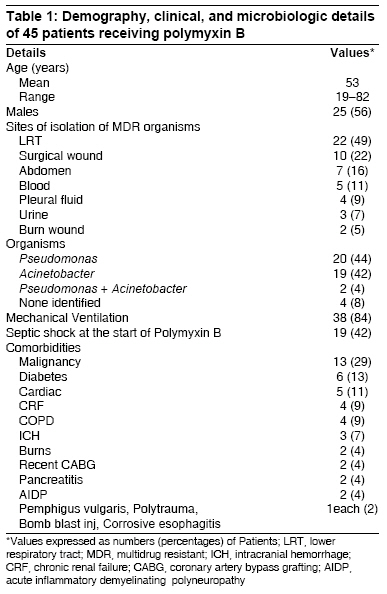
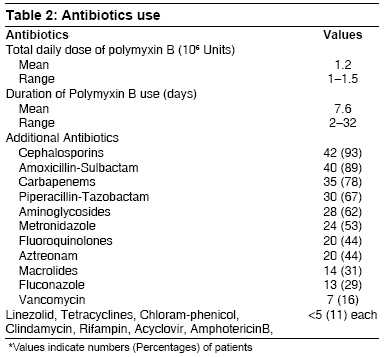
Indian Journal of Critical Care Medicine, Vol. 12, No. 4, October-December, 2008, pp. 153-157 Original Article Safety and efficacy of polymyxin B in multidrug resistant gram-negative severe sepsis and septic shock Ramasubban Suresh, Majumdar Ayanava, Das PurnenduSekhar Department of Critical Care Medicine, Apollo Gleneagles Hospital, Kolkata, W. Bengal Code Number: cm08031 Abstract Background and Aims: The emergence of multidrug resistant strains of Gram-negative bacteria, especially the lactose nonfermenters like Pseudomonas and Acinetobacter, in the intensive care units have prompted renewed worldwide interest in the polymyxins. However, perceived nephrotoxicity has been a major vexation limiting their early and regular use in severe sepsis. This study was conducted to assess the safety and efficacy of polymyxin B in patients with severe sepsis and septic shock.Materials and Methods: Forty-five patients with sepsis admitted in our medical-surgical intensive care units were identified from pharmacy records to have received polymyxin B. We retrospectively reviewed the clinical and microbiologic outcomes as well as occurrence of renal failure temporally related to the use of intravenous polymyxin B. Results: polymyxin B was used in severe sepsis and septic shock with the isolated organism being resistant to other available antimicrobials or clinical deterioration despite carbapenem use. Overall mortality was 52% and among patients who received at least eight days of intravenous polymyxin B, 67% patients with initial septic shock and 62% with severe sepsis survived. The target multidrug resistant organism was cleared in 88% of subjects evaluated by repeat microbiologic testing. Acute renal failure developed in only two patients (4%). Conclusions: Polymyxin B has acceptable effectiveness against nosocomial multidrug resistant Gram-negative sepsis. The associated nephrotoxicity has been found to be significantly lower than previously reported even in patients with background renal impairment and established risk factors of renal failure. Keywords: Acute renal failure, Gram-negative organisms, multidrug resistant, polymyxin B, severe sepsis and septic shock Introduction Multidrug resistant (MDR) Gram-negative bacterial sepsis poses an increasingly daunting challenge in the critical care setting worldwide. [1],[2] Especially the lactose nonfermenters Pseudomonas and Acinetobacter, which are opportunistic niche pathogens affecting primarily the critically ill and the immunocompromised, ubiquitous in the hospital environment and notorious for developing multiresistance to available antibiotics, are making management of sepsis not only difficult but also very expensive even for the industrialized countries. [3],[4],[5] Hence, the worldwide interest in the polymyxins, which have shown consistent efficacy against aerobic Gram-negative bacilli including Pseudomonas and Acinetobacter by their detergent-like cell-membrane-disrupting and antiendotoxin actions, [6],[7] yet their use has been restricted as the last resort in cases of clinical or microbiologic resistance to other available antibiotics, owing to the reports of nephrotoxicity and neurotoxicity. [8],[9] We reviewed our recent experience in the use of intravenous polymyxin B against MDR Gram-negative organisms with particular attention to its nephrotoxicity in the critical care unit in the 350-bed tertiary-level multispecialty Apollo-Gleneagles Hospital situated in Kolkata. Materials and Methods Forty-five patients were identified from pharmacy records who had received more than two doses of intravenous polymyxin B during the period March 2006 and June 2007. The medical records were reviewed retrospectively for demographic details, underlying diseases, presence, severity and source of sepsis, organisms isolated and their antibiotic sensitivity, length of stay in the ICU, dose, frequency and duration of polymyxin B, other antibiotics used, mechanical ventilation and creatinine levels, development of any new rash or neurological problems, and clinical outcomes. The main outcomes of interest included resolution of sepsis, as well as microbiological response to polymyxin B, survival and renal failure temporally linked to the use of polymyxin B. Sepsis was identified by the presence of systemic inflammatory response parameters like temperature, tachycardia, tachypnoea, leucocytosis, and/or leucopenia. Severe sepsis was defined as the presence of organ dysfunction and septic shock as hypotension unresponsive to fluids. [10] Lower respiratory tract secretions were considered pathological if these systemic signs were associated with radiological changes in chest X-ray. Renal failure was defined as acute increase in the serum creatinine level by> 0.5 mg/dL above the baseline over 24 hours. Baseline serum creatinine was defined as the most recent value available at the start of the treatment with polymyxin B. Results As detailed in [Table - 1], the study population comprised 45 critically ill patients with the mean age of the patients being 53 years and 56% being males. Mean duration of stay in the ICU was 38 days (range 6-92 days). Malignancy was the most prevalent underlying comorbidity (29%) followed by diabetes mellitus (13%) and chronic renal failure (9%). Polymyxin B was used in severe sepsis with microbiological or clinical refractoriness to carbapenem antibiotics. Forty-two percent of the subjects were in septic shock and 84% of patients were receiving mechanical ventilation at the time of initiation of polymyxin B. Dose of 15,000 to 25,000 units/kg of ideal body weight in two divided doses per day was used. Total daily dose was reduced by 25% and 50% when the calculated creatinine clearance was 20-50 mL/min and < 20 mL/min, respectively. The mean total daily dose used was 1.2 x 10 6 units and the mean duration 7.6 days. The mean number of days between ICU admission and start of polymyxin was 22 days. All patients received carbapenems, 90% received piperacillin-tazobactam or cefoperazone-sulbactam combination before polymyxin was used. All the patients received other potentially nephrotoxic agents like NSAIDs and diuretics. Fifty-two percent received Amikacin and 16% received Vancomycin [Table - 2]. In our study, the MDR organisms were most commonly isolated from the lower respiratory tract (49%) and surgical wounds (22%). Pseudomonas was isolated in 22 patients and Acinetobacter in 21. Clinical outcomes: Overall mortality was 52% and 40% of patients died or had to be discharged before an eight-day course. Among patients who received at least eight days of intravenous polymyxin B, 67% patients with initial septic shock and 62% with severe sepsis survived and recovered. Acute renal failure developed in only two of the 45 patients treated with polymyxin B (4%). Two patients, a 69-year-old man with esophageal cancer and a 36-year-old lady with vasculitis-induced intracranial bleed developed acute renal failure following treatment with polymyxin B. Acute renal failure developed on day 5 of polymyxin B therapy in the former patient and on day 3 in the later. They died respectively two and nine days after developing acute renal impairment. The mean dose of polymyxin B used was 0.85 x 10 6 units. The mean rise in creatinine level was 0.6 compared to negative 0.1 in patients without renal failure. None of the four patients with background chronic renal impairment developed any acute deterioration after receiving polymyxin B at mean dose of 1.38 x 10 6 units. Microbiologic outcome : Repeat microbiologic culture was obtained in 55% of patients. Thirty-two percent of them cleared the target MDR organism, 56% revealed either a different species or the same organism with sensitivity toward safer broad-spectrum antibiotics. Among patients who failed to clear the target organism, 72% had anatomically uncontrollable surgical site infection and 20% had nosocomial pneumonia. Survival among the patients who received at least eight days of therapy was 67% in the septic shock group and 62% in the nonseptic shock group. Discussion Our study is unique as there is very limited data on the efficacy and safety of polymyxin B in critically ill patients with severe sepsis and septic shock. Polymyxin E, that is, colistin has a large body of evidence, [12],[13],[14],[15],[16],[17],[18] studies involving polymyxin B [19],[20] are limited and our study has the largest number of patients. All patients in our study were critically ill and a majority had severe sepsis and septic shock at time of starting therapy with polymyxin B pointing toward a good efficacy in this group of patients. The relative slow development of safe and new antibiotics [21] has prompted renewed interest in older agents like the polymyxins which were discontinued from clinical practice due to early reports of nephrotoxicity. However, the absence of a unanimous definition of acute renal failure until recently and the significant variation in the incidence of nephrotoxicity shown by Falagas et al, in their review of literature on polymyxins from 1960-2005 [13] call for critical enquiry into the issue. Reported incidence of nephrotoxicity in the earlier literature [22],[23],[24],[25] varied widely between 20-25% and up to 100% of recipients. Recent Western estimates on nephrotoxicity have been much more moderate with 10-14% [19],[20] for polymyxin B and 24% for colistimethate sodium. [13] Sepsis itself has adverse effects on renal function [28] and hence becomes a confounding factor in assessing the nephrotoxicity of polymyxins when therapy is initiated as a last resort in advanced stage of septicemia. Nosocomial sepsis with septic shock has a very high mortality and an acceptable clinical and microbiologic improvement was obtained with polymyxin B in our study. Overall mortality was 52% in our study. Forty-two percent of patients were in septic shock before initiation of polymyxin B. Polymyxin B was started after results of cultures were obtained in most of the patients with sepsis. Late use of polymyxin B might have blunted its efficacy as definite prognostic advantage is derived with early use of appropriate antibiotics in sepsis. [27] Previous studies with polymyxin B have shown mortality between 20-48%. Mortality in respiratory tract infections treated with polymyxin B [19] is about 48%, and in the study published by Ouderkirk et al, [20] the overall mortality was 20%. However, data as to number of patients in shock is not available, so comparative conclusions on efficacy is difficult. Microbiologic response with polymyxin B in our study is also comparable to the efficacy reported in the study by Ouderkirk. Our limitation is the lack of a comparative cohort treated with other antibiotics. The retrospective nature of this study is also a drawback. Hence, as the stigmata of nephrotoxicity associated with the use of polymyxin B is being questioned worldwide, we need to consider it early in severe nosocomial sepsis where MDR organisms are suspected, with careful monitoring of renal function. References
Copyright 2008 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm08031t2.jpg] [cm08031t1.jpg] |
| |||||||||

{kind=link}
{kind=link}