 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
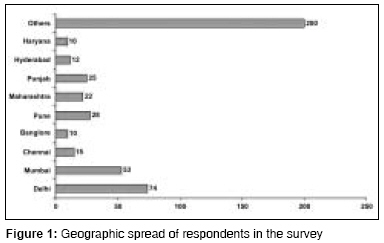
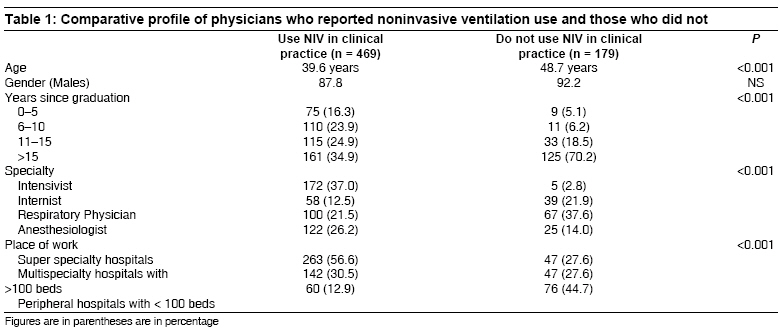
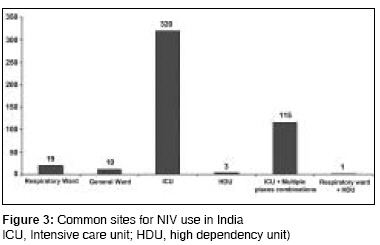
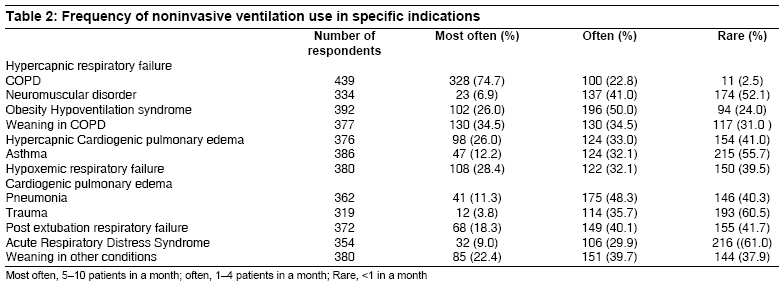
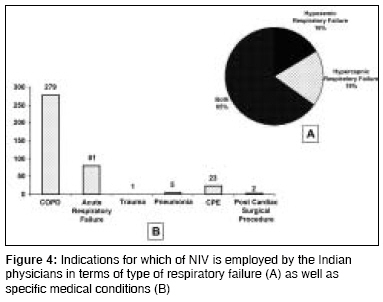
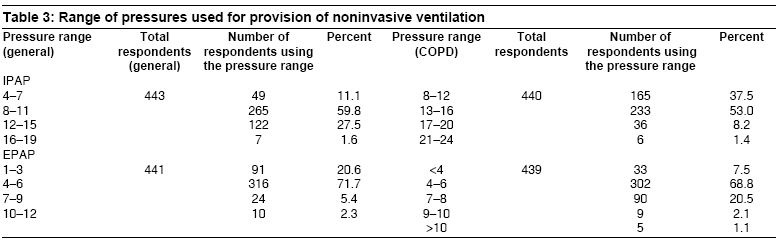
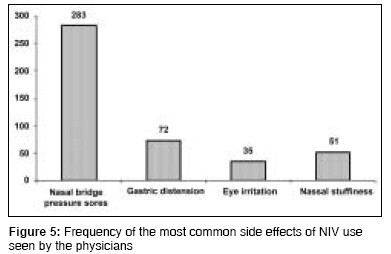
Indian Journal of Critical Care Medicine, Vol. 12, No. 4, October-December, 2008, pp. 163-169 Original Article Noninvasive ventilation: A survey of practice patterns of its use in India Chawla Rajesh, Sidhu US, Kumar Vijai, Nagarkar Shruti, Brochard Laurent Department of Pulmonary, Critical Care and Sleep Medicine, Indraprastha Apollo Hospitals, New Delhi Code Number: cm08033 Abstract Background and Aims : To understand the practice patterns of noninvasive ventilation (NIV) use by Indian physicians.Subjects and Methods : Around three thousand physicians from all over India were mailed a questionnaire that could capture the practice patterns of NIV use. Results : Completed responses were received from 648 physicians (21.6%). Majority ( n = 469, 72.4%, age 40 ± 9 years, M:F 409:60) use NIV in their clinical practice. NIV was most exclusively being used in the ICU setting (68.4%) and the commonest indication for its use was chronic obstructive pulmonary disease (COPD) (71.4%). A significant number did not report use of a conventional ventilator for NIV support (62%). Oronasal mask was the overwhelming favorite among the sampled physicians (68.2%). In most of the cases, the treating physician initiated NIV (60.8%) and a baseline blood gas analysis was performed in only 71.1% of the cases (315/443). Nasal bridge pressure sores was the commonest complication (64.2%). Conclusions : NIV is being widely used in clinical practice in India for various indications. COPD is the most common indication for its deployment. There seems to be a marked variability in the patterns relating to actual deployment of NIV, including the site of initiation, protocols for initiation followed, and monitoring of patients. Keywords: Noninvasive ventilation, questionnaire-based study, survey Introduction Noninvasive ventilation (NIV) is a useful therapy for management of selected patients with respiratory failure. [1],[2],[3],[4] Significant variability in the practice patterns of NIV use has been observed across the world. [5],[6],[7] However, NIV is of particular interest for a country like India for several reasons. India is a large country in which the healthcare system is facing major cost limitations. NIV has the potential to be a much cheaper option than conventional mechanical ventilation by reducing complications and length of hospital stay, and in some cases, by avoiding ICU admission when delivered outside the ICU. It can also be delivered by relatively simple equipments, reducing this part of the costs. Lastly, although there is lack of formal data, the diseases well treated by NIV, such as acute exacerbation of chronic obstructive pulmonary disease (COPD) and acute cardiogenic pulmonary edema have a high incidence in India and represent huge number of cases. The use of NIV may, however, be limited by different reasons including physician′s training. It is therefore relevant to assess the current practice patterns of NIV use by the Indian physicians.Materials and Methods Instrument Subjects Questionnaires were mailed along with a self-addressed envelope, to all the members on the addresses available in the directories over the next two months. The responses were awaited for next six months before E-mail reminders were sent to physicians whose E-mail ID′s were available in the directories. At the end of a total eight months after mailing all the questionnaires, data were entered into a Microsoft excel worksheet and analysis conducted. Statistical analysis Results Responses were received from 648 physicians (response rate: 21.6%). All respondents, however, did not reply to all the questions and the number of replies varied for each question. A majority of respondents comprised of Intensivists (63.2%). Geographically, almost all the regions of the country were represented in the survey sample with Delhi (n = 74, 16.5%) and Mumbai (n = 53, 11.8%) being the top two in terms of number of respondents ([Figure - 1], Electronic Supplementary Material). Use and nonuse of NIV Indications for NIV Equipment for provision of NIV Provision of NIV and blood gas analysis Complications of NIV An overwhelming majority of physicians felt that guidelines regarding use of NIV would be useful (94%), only 31.6% of the respondents were aware about the existence of any guidelines. The awareness was highest among the Intensivists (37.7%) followed by Anaesthesiologists (34.5%). Discussion The present study aimed to evaluate the practice patterns of NIV use among physicians from India. To the best of our knowledge, this is the first study of its kind in India although similar work has been carried out in the West. [8],[9] The survey utilized a simple instrument that was developed indigenously. The questionnaire was kept simple, short, and concise with objective responses to maximize the response rate. Although frequently observed in this kind of survey, the response rate to the survey was low, which was probably influenced by the survey methodology that was employed. Though almost 3000 questionnaires were mailed, it cannot be ascertained with certainty how many physicians actually received the same as many members do not update their change of addresses in the society directories. Given this scenario, the true response rate (given a different denominator of physicians who actually received the questionnaire) of the current study would be higher. Moreover, the average response rate in physician postal surveys has been determined to be just more than 50%. [10],[11] It must be acknowledged though that a selection bias favoring the physicians who use NIV to respond may tend to occur. It is therefore difficult to extrapolate the specific figure of proportion of physicians using NIV to the whole of country. The overall profile of the group of physicians that did not use NIV in their clinical practice was understandably different from those that did use NIV. It is likely that older physicians who work in peripheral hospitals and do not have subspecialty training, would be the group more likely to persist with traditional management approaches. Interestingly, the association between fewer years in clinical practice and NIV use was also found in the Ontario survey. [9] One of the key findings of the study was the finding of marked underutilization of NIV outside ICU. Whereas NIV continues to be largely used in an intensive care setting, it is being increasingly deployed in general wards as well. The study by Plant and coworkers [12] where equivocal results were demonstrated with use on NIV in general wards has been largely responsible for this development. However, the same does not seem to be the case in the present survey and this is one area where awareness levels need to go up. This is especially important for resources-limited settings such as those in India where a perennial shortage of intensive care beds exists. The indications for the use of NIV remained largely similar and did not differ by the place of use, hospital setup, physician specialty, or the number of years of use of NIV. The earlier two surveys also found COPD as the commonest indication for provision of NIV support. [8],[9] This is pretty much on expected lines, given the weight of the evidence supporting the role of NIV in management of patients with exacerbation of COPD. However, very few respondents reported use of NIV for cardiogenic pulmonary edema and awareness regarding the use of NIV in this setting should also go up. It was intriguing to note that despite broad consistencies in the indications for which NIV is used, significant heterogeneity was the norm when it came to the delivery techniques. Use of conventional ICU ventilators for provision of NIV was noted more frequently with Internists as a specialty and with those who were using NIV for lesser number of years. It appears that some of the more experienced and subspecialist operators are reluctant to use conventional ventilators for provision of NIV. Unless the same is the result of unavailability of conventional ventilators in the setup, one would wish that physicians attempt to maximize the utilization of available resources in the setup. As per the current guidelines, most of the settings where NIV is used, backup conventional ventilators would be available, [13],[14] and so was the case in the current survey where an overwhelming majority of physicians reported availability of backup conventional ventilators (92.2%). However, when it came to carrying out blood gas analysis before initiation of NIV, almost 30% did not report following this protocol and would go by their clinical judgment while initiating a patient on NIV. Moreover, 15% of physicians were actually using NIV in absence of availability of blood gas analysis in their setups. Although, we did not compare the outcomes of the patients that are managed in this fashion with those managed as per the standard protocols, these findings do lend credence to the feasibility of such an approach. These possibilities need to be explored in future studies, especially in resources-limited settings. It is well known that many of the healthcare setups in the peripheries of the country cannot offer anything more than oxygen therapy in terms of respiratory support to the patients. It may also be possible in many of these centers to procure a NIV but are probably discouraged because of the norm that NIV should be used only in monitored settings and with availability of backup conventional ventilators. However, in a setup where no other means of providing assisted ventilation is available, patients could be offered NIV as a stand-alone modality of assisted ventilation. Whereas this may not be done when a referral of the patient to a higher level of care is possible, it can certainly help to improve outcomes when no other option is available. It was also noted that majority of times NIV was initiated by the physicians themselves. However, in many settings it is possible that physicians may not be available all the times and during such times the "window of opportunity" of initiating NIV in a timely fashion must not be missed. It is therefore worthwhile to train more nursing and paramedical staff in use of NIV. It is concluded that a majority of participating physicians across different specialties, backgrounds, and from different healthcare setups use NIV in their clinical practice. The indications for which NIV is utilized were also similar across the study cohort. However, significant heterogeneity was seen in terms of training received and the delivery methods employed by the physicians from different specialties. Acknowledgment The authors express their gratitude toward the Indian Society of Critical Care Medicine (Delhi Chapter) for providing financial support for stationary items and postage. Authors also thank Dr Amit Banga, MD, FCCP for providing critical inputs during statistical analysis and preparation of manuscript.References
Copyright 2008 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm08033f3.jpg] [cm08033t3.jpg] [cm08033t1.jpg] [cm08033f5.jpg] [cm08033f1.jpg] [cm08033t2.jpg] [cm08033f4.jpg] [cm08033f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}