 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
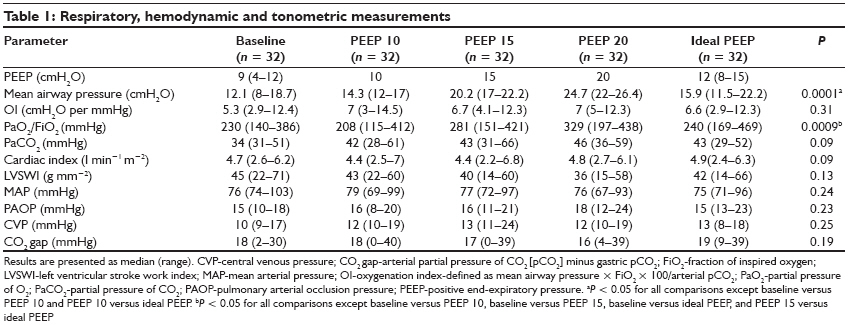
Indian Journal of Critical Care Medicine, Vol. 13, No. 1, January-March, 2009, pp. 12-16 Research Article Changes of splanchnic perfusion after applying positive end expiratory pressure in patients with acute respiratory distress syndrome Sarkar Suman, Bhattacharya Prithwis, Kumar Indrajit, Mandal KrutiSundar Department of Anesthesiology, Intensive Care Unit, IMS Banaras Hindu University, Varanasi-221 105, Uttar Pradesh Code Number: cm09003 Abstract Background: Positive end-expiratory pressure (PEEP) improves oxygenation and can prevent ventilator- induced lung injury in patients with acute respiratory distress syndrome (ARDS). Nevertheless, PEEP can also induce detrimental effects by its influence on the cardiovascular system. The purpose of this study was to assess the effects of PEEP on gastric mucosal perfusion while applying a protective ventilatory strategy in patients with ARDS.Materials and Methods: Thirty-two patients were included in the study. A pressure-volume curve was traced and ideal PEEP, defined as lower inflection point + 2cmH 2 O, was determined. Gastric tonometry was measured continuously (Tonocap). After baseline measurements, 10, 15 and 20cmH 2 O PEEP and ideal PEEP were applied for 30 min each. By the end of each period, hemodynamics, CO 2 gap (gastric minus arterial partial pressures), and ventilatory measurements were taken. Results: PEEP had no effect on CO 2 gap (median [range], baseline: 18 [2-30] mmHg; PEEP 10: 18 [0-40] mmHg; PEEP 15: 17 [0-39] mmHg; PEEP 20: 16 [4-39] mmHg; ideal PEEP: 19 [9-39] mmHg; P = 0.19). Cardiac index also remained unchanged (baseline: 4.7 [2.6-6.2] l min−1 m−2 ; PEEP 10: 4.4 [2.5-7] l min−1 m−2 ; PEEP 15: 4.4 [2.2-6.8] l min−1 m−2 ; PEEP 20: 4.8 [2.4-6.3] l min−1 m−2 ; ideal PEEP: 4.9 [2.4-6.3] l min−1 m−2 ; P = 0.09). Conclusion: PEEP of 10-20 cmH 2 O does not affect splanchnic perfusion and is hemodynamically well tolerated in most patients with ARDS, including those receiving inotropic supports. Keywords: Acute respiratory distress syndrome, gastric mucosal perfusion, positive end-expiratory pressure, tonometry Introduction Many recent studies have shown that mechanical ventilation (MV) in patients with acute respiratory distress syndrome (ARDS), using low tidal volumes and high levels of positive end-expiratory pressure (PEEP) reduces the mortality rate and this ventilatory strategy is now accepted as standard practice in patients with ARDS. [1],[2] Although PEEP improves arterial oxygenation, it has adverse hemodynamic effects. PEEP reduces the venous return to the heart and the left ventricular end diastolic volume by pushing the inter ventricular septum towards the left, and thus reduces the cardiac output. These effects are proportional to the PEEP level. Regional perfusion can also be affected by PEEP, independently of cardiac output changes. The splanchnic perfusion is particularly sensitive, and any reduction can compromise its barrier function, promote bacterial translocation, and contribute to the development of multiple organ failure. [3] In experimental models, PEEP has markedly decreased mesenteric and portal blood flow, despite only moderate reductions in cardiac output. [4],[5],[6],[7],[8] Similar results have been reported in patients without lung injury. [9],[10] These effects are usually dose related, becoming more pronounced with PEEP levels around 20 cmH 2 O. Kiefer reported that PEEP did not significantly alter splanchnic circulation in six patients with acute lung injury. [11] Nevertheless, caution should be exercised in extending these results to clinical practice, because only hemodynamically stable patients without adrenergic drugs were studied, and PEEP levels never exceeded 14 cmH 2 O. [12] Our aim was to evaluate the effects of PEEP levels up to 20 cmH 2 O on gastric mucosal perfusion and systemic hemodynamics in mechanically ventilated patients with ARDS on hemodynamic support. Materials and Methods Patients Adult, mechanically ventilated patients were considered eligible for the study if they met the following criteria for ARDS during the 24 hours that preceded the study: a0 cute onset of respiratory failure; diffuse bilateral infiltrates in the chest radiograph involving more than three-fourths of both lung fields; a ratio of partial pressure of O 2 (PaO 2 ) to fraction of inspired oxygen (FiO 2 ) of less than 200 mmHg; and a pulmonary arterial occlusion pressure less than 18 mmHg and no cardiac failure. Hemodynamic monitoring included an arterial line and a pulmonary artery catheter. Patients could be on vasopressor or inotropic support (Dopamine 5-20 microgram/kg/min with or without Noradrenaline 10- 20 micrograms /min dose), but had to be hemodynamically stable (with a mean arterial blood pressure of more than 60mm of Hg, pulse rate should be less than 100/min and more than 50 per minute) for at least 5 hours before starting the protocol. Patients were excluded if they had any of the following conditions: Pregnancy, pre-existing respiratory dysfunction, cardiac index of less than 2.5 l min−1 m−2 , or were receiving enteral nutrition. Interventions PEEP levels of 10, 15, 20 cmH 2 O, and ideal PEEP, with tidal volumes of 6 ml kg−1 , were applied in four consecutive 30 min periods, respectively. Respiratory rate was modified to maintain end tidal CO 2 within ±10mmHg of basal. All patients were receiving a constant infusion of 6% hetastarch before the beginning of the study (40-60 ml h−1 ). Cardiac output was optimized before and during the trial by determining the respiratory variation of systolic arterial pressure. [14] Whenever the variation was more than 10% a 100 ml bolus of 6% hetastarch was infused and the volume status was reassessed. No changes in vasopressor or inotropic support were allowed during the study. If hypotension (mean arterial pressure < 60 mmHg) persisted for more than 2 min, the protocol was stopped. Measurements Statistical analysis Results Thirty-two patients with ARDS were enrolled. They had a median (range) age of 47 years, (25 were male and seven were female, and two of the female patients were in postpartum state, four patients had previous history of diabetes) and an Acute Physiology and Chronic Health Evaluation II score of 20 at admission to the intensive care unit. On the day of the study they had a median Sepsis-related Organ Failure Assessment (SOFA) [15] score of 10. All patients fulfilled criteria for ARDS, as defined by the inclusion criteria, during the 24 hours before the study and they had been on mechanical ventilation for 32 (12-72) hours. They were being ventilated with a median PEEP level of 9 (4-12) cmH 2 O, had a PaO 2 /FiO 2 ratio of 230 (140-386) mmHg and their respiratory system compliance was 45 (27-60)ml per cmH 2 O. Twenty-eight patients had sepsis (eight pneumonia and 20 extra pulmonary sepsis), and four had severe head and thoracic injury. Of the septic patients, 24 were in septic shock. No changes in cardiac index or in CO 2 gap were found at any of the study periods [Table - 1]. Oxygenation index, mean arterial pressure, pulmonary mean arterial pressure, pulmonary artery occlusion pressure, central venous pressure and left ventricular stroke work index also remained stable through the study. Only mean airway pressure and PaO 2 /FiO 2 ratio differed between periods, as expected. Twenty patients required a 100ml bolus of hetastarch during the trial; in no patient was it necessary to repeat it. At baseline, 12 patients had already a CO 2 gap of more than 20 mmHg. After starting the protocol with 10 cmH 2 O PEEP, 24 patients decreased their CO 2 gap and eight increased it. When PEEP was increased from 15 to 20 cmH 2 O, 12 patients increased their CO 2 gap, 12 decreased it and in four patients it remained unchanged. Twenty-four of the 32 patients studied, survived (75%). The median length of stay in the intensive care unit was 18 days and the median duration of mechanical ventilation was 11 (5-34) days. Discussion Similar studies have been done previously, but the number of cases studied were very few; we have done this study with a relatively large number of patients and our results show that high PEEP levels (up to 20 cmH 2 O) do not compromise gastric mucosal perfusion, as assessed by tonometry, and do not affect systemic hemodynamics in most patients with ARDS. This is consistent with the findings of two other studies on the effects of PEEP on splanchnic perfusion in patients with ARDS. However, in contrast to our study, neither of those studies included patients in septic shock or on adrenergic support. [11],[16] Shock and cardiovascular dysfunction are frequently associated with ARDS. This is an important issue, because hemodynamic safety concerns could preclude the use of high or optimal PEEP levels in that setting, even if necessary. A major finding of our study is that PEEP levels up to 20 cmH 2 O can be well tolerated, even in patients with ARDS and septic shock. Nevertheless, our trial was relatively short and we cannot exclude the possibility that keeping high PEEP levels for a longer period might result in increased fluid requirements, which could be deleterious in the longer term. Experimental and clinical research has demonstrated that in mechanically ventilated subjects without lung injury, PEEP decreases venous return and, secondarily, cardiac output. [17],[18],[19] In addition, Trager and colleagues showed that in patients with acute respiratory failure associated with septic shock, high PEEP levels induced a decrease in cardiac output. [20] In contrast, we found no decrease in cardiac output in our patients tested with increasing PEEP levels when fluid administration was optimized according to the respiratory variation in systolic arterial pressure. A similar result was reported by Kiefer et al . and by Akinci et al . [11],[16] Possible explanations for these contradictory results are a higher rate of fluid administration and the use of lower tidal volumes in the latter studies. Although we did not determine the upper inflection point of the pressure-volume curve, we think that by keeping tidal volume at 6 ml kg−1 any overdistension of the lungs was minimized. Lung volumes are a critical component of the hemodynamic effects of ventilation. [21] Thus, it seems that it is possible to preserve cardiac output in patients with ARDS, despite the use of high PEEP levels, by optimizing fluid administration and limiting tidal volumes. Gastric mucosal perfusion, as assessed by CO 2 gap, also remained unchanged during the PEEP trial. This is consistent with the results reported by Kiefer and Akinci in similar studies. In all these studies cardiac output remained unchanged. [11],[16] In contrast, Trager reported, in a series of septic shock patients with acute respiratory failure, that an increase in PEEP from 5 to 15 cmH 2 O induced a decrease in cardiac output associated with a decrease in hepatic vein O 2 saturation and in hepatic glucose production. [20] It therefore seems that by avoiding a decrease in cardiac output, splanchnic perfusion can be preserved in a majority of patients. One major limitation of our study is the small number of patients studied. Thus, a type II error cannot be excluded. We did not perform any a priori power analysis because we had no estimation of the possible magnitude of the effects that PEEP could have on gastric tonometry. Another limitation is the rather moderate severity of ARDS in our study. Although all patients fulfilled the criteria for ARDS during the 24 hours that preceded the study, at inclusion their PaO 2 /FiO 2 ratio and their respiratory system compliance were only moderately decreased. Two recent papers provide an explanation for this observation. [22],[23] They show in patients diagnosed with ARDS that after a few hours of treatment with PEEP or a high FiO 2 , more than half of the patients present a PaO 2 /FiO 2 ratio of more than 200 mmHg. In addition, the respiratory system compliance increased by more than 10 ml per cmH 2 O after 6 hours of treatment with PEEP. [23] At inclusion our patients had already been ventilated with a median PEEP level of 9 cmH 2 O for more than 12 hours, which could have explained the rather improved respiratory performance at baseline. In any event, this improvement demonstrated a less severe ARDS. It is possible that more severely compromised patients might present a lower tolerance to high PEEP levels. Another limitation is that tonometry was the sole method used to assess gastric mucosal perfusion. Nevertheless, Elizalde et al . showed that gastric mucosal blood flow, measured by laser Doppler flowmetry and by reflectance spectrophotometry, is well correlated with gastric intramucosal acidosis in mechanically ventilated patients. [24] Conclusions Our study supports the findings of previous studies suggesting that high PEEP levels do not affect splanchnic perfusion and are hemodynamically well tolerated in most patients with ARDS. Furthermore, our study shows that gastric mucosal perfusion can be well preserved while high PEEP levels are applied even in patients presenting cardiovascular dysfunction and receiving vasopressor support, which is a frequent occurrence in critical care. Future studies should assess the effects of PEEP on splanchnic perfusion in a longer term.References
Copyright 2009 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm09003t1.jpg] |
| |||||||||

{kind=link}