 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
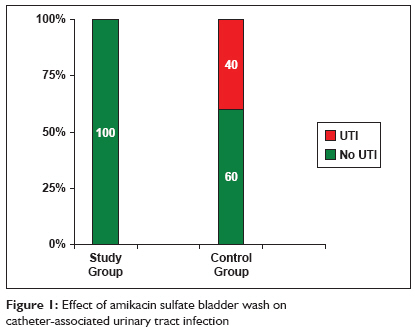
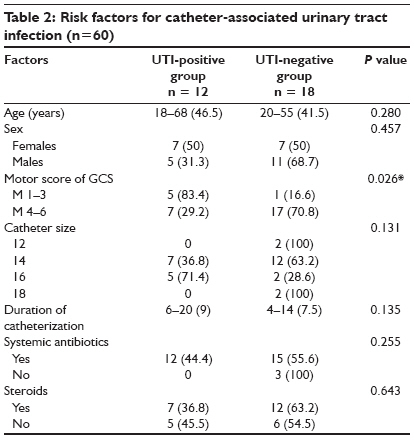
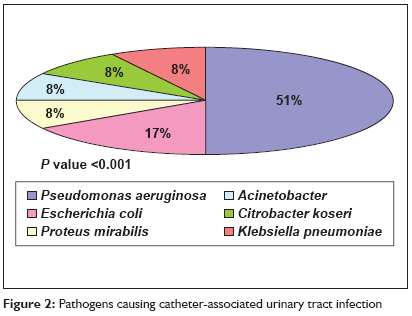
Indian Journal of Critical Care Medicine, Vol. 13, No. 1, January-March, 2009, pp. 17-20 Research Article A comparative study to assess the effect of amikacin sulfate bladder wash on catheter-associated urinary tract infection in neurosurgical patients Zacharias Sumi, Dwarakanath Srinivas, Agarwal Meena, Sharma BhavaniShankar Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi Code Number: cm09004 Abstract Background: The indwelling urinary catheter is an essential part of modern medical care. Unfortunately, when poorly managed, the indwelling catheter may present a hazard to the very patients it is designed to protect. Catheter-associated urinary tract infection (CAUTI) is the most common nosocomial infection in hospitals and nursing homes.Aims and Objectives: The primary objective was to study the effect of amikacin sulfate bladder wash on CAUTI in neurosurgical patients. The other objectives were to study the various organisms causing CAUTI and their antibiotic sensitivity and resistance pattern. Materials and Methods: This was a prospective randomized controlled study performed on 60 patients who met the inclusion criteria at the neurosurgical intensive care of the All India Institute of Medical Sciences between June and December 2006. The patients were randomized into two groups - one was the trial group which received amikacin bladder wash, while the other was the control group that did not receive any bladder wash. Results: Forty percent of the subjects in the control group developed CAUTI, while none of the subjects in study group developed CAUTI. (Fisher's exact test, P value < 0.001) Pseudomonas aeruginosa (51%) was the commonest pathogen. Conclusions: Amikacin sulfate bladder wash was effective in preventing CAUTI. It can thus decrease the antibiotic usage thereby preventing the emergence of antibiotic resistance. Keywords: Amikacin bladder irrigation, bladder wash, catherer-associated urinary tract infection Introduction The indwelling urinary catheter is an essential part of modern medical care and a variety of different indwelling urinary catheters can be used for various purposes. Each year, urinary catheters are inserted in more than five million patients in acute-care hospitals and extended-care facilities. [1] Unfortunately, when poorly managed, the indwelling catheter may present a hazard to the very patients it is designed to protect. Catheter-associated urinary tract infection (CAUTI) is the most common nosocomial infection in hospitals and nursing homes, comprising> 40% of all institutionally acquired infections. [2],[3],[4],[5],[6] Interventions such as topical meatal antimicrobials, disinfectants added to the urinary drainage bag, and antimicrobials coatings for catheters have not been shown to decrease the incidence of UTI. [7] An effective measure to prevent the CAUTI has not yet been developed. The most common organisms responsible for CAUTI are Escherichia coli , Candida spp., Klebsiella pneumoniae , Streptococcus agalactiae , Enterococcus faecalis , and Pseudomonas aeruginosa . Amikacin has proven to be the most effective antibiotic in preventing the growth of all these species. [8] Previous studies have shown that using individualized regimens for bladder washouts minimizes the infection rate and catheter blockage, thus reducing the need for frequent recatheterization. [9] Since there is no significant systemic absorption of antibiotics used for bladder irrigation, [10] prophylactic bladder irrigations are considered to be safe. We performed an extensive review of literature which did not reveal any study done on the effectiveness of amikacin sulfate bladder wash. Materials and Methods This study was performed on a total of 60 catheterized patients who were admitted to the Neurosurgery Department of AIIMS, New Delhi, during June-December 2006 and met the inclusion criteria [Appendix 1]. The subject data sheet and procedure of amikacin sulfate bladder wash was developed under the guidance of a guide (Author 3) and co-guides (Authors 2 and 4), and was further validated by six experts from the Departments of Neurosurgery, Microbiology, and Nursing, AIIMS. Informed written consent was taken from the patients or patients′ relatives after providing appropriate information to the concerned. Confidentiality of the data was ensured. They were randomized after catheterization to either of the two groups - study and the control groups. Then urine samples were sent within 24 hours for culture and sensitivity (C/S), in case of positive C/S, patients were excluded from the study [Appendix 2]. Study group received amikacin sulfate bladder wash twice daily under strict aseptic precautions and the control group did not receive bladder wash [Appendix 3]. Urine C/S was performed on days 3, 7, and then weekly till the removal of catheter or discharge. Both groups received standard catheter care including perineal care; the only difference was the bladder wash. The researcher (Author 1) performed the bladder wash on all patients to eliminate bias. CAUTI was diagnosed when it met the respective criteria [Appendix 4]. Statistical methods The study was conducted following the approval of ethics committee of All India Institute of Medical Sciences (AIIMS). Results Demographic profile of patients Incidence of catheter-associated urinary tract infection and predisposing factors Organism and sensitivity profile Discussion The present study is the first of its kind in which the effect of amikacin bladder wash has been analyzed. Efficiency of bladder irrigation using various different solutions have been studied in the past in an attempt to reduce the incidence of CAUTI, majority of the investigators found it to be a time consuming and costly procedure that did not have an impact on CAUTI. [11],[12],[13],[14],[15] In contrast, the present study revealed that amikacin bladder wash is effective in preventing CAUTI. In previous studies, the incidence of CAUTI ranged from 11.0-73.3%. [16],[17] In the present study, incidence of CAUTI was 40% since those who were catheterized for less than three days were excluded in the study. This inclusion criterion might be the chief reason for a higher incidence of CAUTI in the present study. CAUTI increases the burden of the patient in terms of increased morbidity and mortality, prolonged hospital stay, and cost of the tests and medicines. [17],[18],[19] Tambyah et al. , [20] found that CAUTI had been responsible for an additional of USD589 per CAUTI in diagnostic tests and in medications. The present study reveals that amikacin sulfate bladder wash is effective in preventing CAUTI. As a vial of amikacin sulfate (500 mg) costs INR58 (approximately USD1.4), this is very cost effective especially in a developing country like ours. Puri et al. , [21] in their study said that the risk was significantly higher for females, elderly patients, critically ill patients, and those on prolonged catheterization. The present study showed only severity of the disease (low motor score of GCS) as a statistically significant risk factor. This might be since a lower GCS corresponds to the severity of tissue injury, where there is hypermetabolism and increased protein catabolism, which eventually leads to decreased immunity that makes the person more susceptible to infections. However, the present study did not show any influence of sex, age, catheter size, duration of catheterization, and systemic use of antibiotics and steroids. This might be because of the small sample size and inclusion of long-term catheterized patients only. Pathogenic organisms responsible for CAUTI and their antibiotic sensitivity pattern vary with time. In a study, Jha et al. , [22] found that most common organisms responsible for CAUTI were E. coli (49%), S. aureus (23%), Proteus spp. (3.6%), Klebsiella (9.71%), Pseudomonas (0.8%), and Citrobacter (2.8%). Whereas in the present study, Pseudomonas (51%), E. coli (17%), Proteus spp., Citrobacter , Klebsiella , and Acinetobacter (8% each) were the most common. Similarly, antibiotic resistance pattern also varied. In their study, Taneja et al. , [23] found the highest frequency of antibiotic resistance was for ciprofloxacin (68.6%) followed by netilmicin (60.7%), ceftazidime (58.8%), imipenem (43.7%), amikacin (43.1%), and piperacillin (39.2%). In the present study, the pattern of antibiotic resistance was ceftazidime (100%), netilmicin (83%), imipenem (75%), ciprofloxacin (75%), and meropenem (60%). In this study, we have shown that amikacin sulfate bladder wash is very effective in preventing CAUTI. Thus it can be included in the routine catheter care, especially if catheterization is needed for more than five days. It is easy to implement and cost effective. The main limitation of this study was the small sample size and the fact that the main researcher was not blinded to the study. Conclusions There is a varying pattern of antibiotic sensitivity and resistance in different institutions. The most important thing to note is the fact that the bacteria have started developing resistance to higher antibiotics. This is very important since the indiscriminate use of antibiotics can lead to resistance, thus potentially endangering the life of a patient. This increasing resistance calls for immediate measures to use methods other than oral or parenteral antibiotics in CAUTI. We believe that this study is important because if used can decrease the development of CAUTI.References
Copyright 2009 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm09004f1.jpg] [cm09004t1.jpg] [cm09004t2.jpg] [cm09004f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}