 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
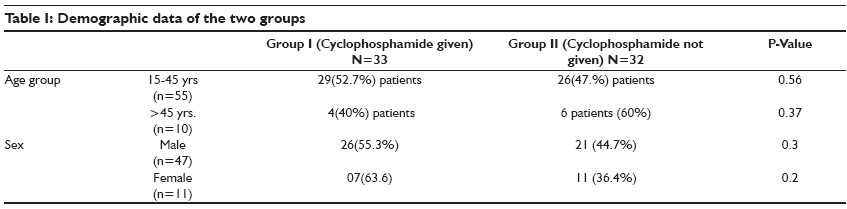
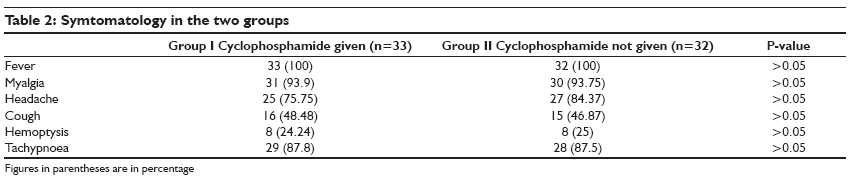
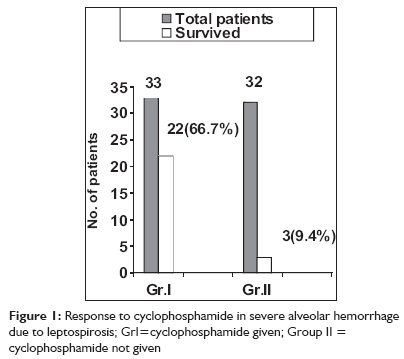
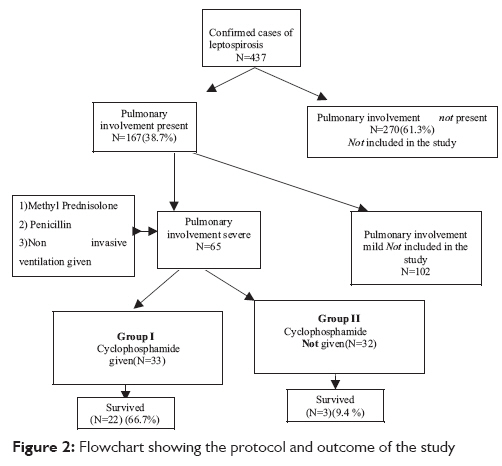
Indian Journal of Critical Care Medicine, Vol. 13, No. 2, April-June, 2009, pp. 79-84 Research Article Cyclophosphamide in pulmonary alveolar hemorrhage due to leptospirosis Trivedi SamirV, Vasava AshwinH, Patel TinkalC, Bhatia LovleenC Department of Medicine, Government Medical College, Surat Code Number: cm09018 PMID: 19881188 Abstract Background and Aims : Severe pulmonary involvement in leptospirosis carries high mortality rates. It is the most common cause of death due to leptospirosis in many parts of India and the world. Exacerbated immune response of the host plays an important role in its pathogenesis. Hence, immunosuppressive drugs could be useful in its treatment. Glucocorticosteroids have been found to be useful in several studies. Cyclophosphamide, an immunosuppressive agent, has been found to be useful in a majority of pulmonary alveolar hemorrhages due to non leptospiral causes. This study was carried out to study the effects of cyclophosphamide in patients with leptospiral pulmonary alveolar hemorrhage.Method: A total of 65 patients with confirmed leptospirosis with severe pulmonary involvement admitted to a tertiary care center in south Gujarat were included in the study. All of the patients were treated with injection crystalline penicillin, methyl prednisolone pulse therapy, and non invasive mechanical ventilation. A total of 33 patients were given parenteral cyclophosphamide 60 mg/kg body weight stat on diagnosis. Their outcomes were compared with the remaining 32 patients who had not been given this drug. Survival was considered the main outcome indicator. Results: Out of the 33 patients treated with cyclophosphamide, 22 (66.7%) survived, while in the control group out of 32 patients, three (9.4%) survived. On statistical analysis, the odds ratio was 19.33 (4.22-102.13) and the P-value was < 0.001. Leucopenia (78.78%) and alopecia (18.75%) were the main side effects noted. No mortality was noted due to these side effects. Conclusion: Cyclophosphamide improves survival in cases of severe pulmonary alveolar hemorrhage due to leptospirosis. Statistically, the improvement is highly significant. Keywords: Cyclophosphamide, leptospirosis, pulmonary alveolar hemorrhage Introduction Pulmonary involvement in leptospirosis has been reported from all over the world. [1] In India, it has also been documented from all the places where leptospirosis cases occur. In fact, it is the most common cause of death due to leptospirosis in several parts of India. [2],[3] The basic pathology in pulmonary involvement is alveolar hemorrhage. [4] Immune causes are responsible for the majority of non leptospiral pulmonary alveolar hemorrhages. [5] Vasculitis is one of the more important of these immune causes. They are all treated with prednisolone and cyclophosphamide. [5] Immune mechanisms have been implicated in the pathogenesis of alveolar hemorrhage due to leptospirosis as well. [1] Leptospirosis is an infectious vasculitis. [6] There are reports of the successful use of glucocorticosteroids in leptospiral alveolar hemorrhage. [7],[8],[9],[10],[11] But, there are reports that cases of leptospirosis are becoming more severe all over the world. [1] In Gujarat, we have noted an increase in the severity of leptospirosis with decreasing response to glucocorticosteroids. (This aspect is elaborated further in the Discussion section.) Immune mechanisms have been implicated for the increasing severity of leptospirosis. Cyclophosphamide has been an integral part of the treatment regimen used to treat non leptospiral causes of pulmonary hemorrhage. [5] Hence, we decided to evaluate its role in pulmonary alveolar hemorrhage due to leptospirosis. Results of the study are presented in this paper. Materials and Methods Patient selection At the outset , approval by the Human Research Ethics Committee of the college was obtained. The study was carried out at a tertiary care center in south Gujarat where severe leptospirosis patients from three districts are referred. The study was carried out between July 2007 and October 2007. This is the peak season for leptospirosis in south Gujarat because of the monsoon season. Suspected patients were subjected to serological tests for leptospirosis and polymerase chain reaction (PCR). The serological tests included dipstick tests for lepto antibodies, IgM enzyme linked immunosorbent essay (ELISA), and microscopic agglutination test (MAT). The World Health Organization (WHO) International Leptospirosis Society (ILS) guidelines were followed for the diagnosis of leptospirosis. [12] Besides a clinical examination, certain investigations were carried out in patients with confirmed leptospirosis. They included complete blood counts, renal function tests, hepatic function tests, and arterial blood gas analysis. Tests for the diagnosis of hepatitis B and C, dengue (IgM), and malaria (peripheral smear and rapid test) were also carried out. A chest X-ray, electrocardiogram (ECG), and abdominal ultrasound were also done. The presence of respiratory symptoms or signs (breathlessness, tachypnoea, cough, or hemoptysis) and/or a chest X-ray showing infiltrates, was considered as pulmonary involvement. An acute lung injury (ALI) score, developed by Murray et al., was used to determine the severity of pulmonary involvement. [13] Patients having an ALI score ≥2.5 were considered to have severe pulmonary involvement and were included in the study. Other causes of opacities in the lungs, like tuberculosis, pneumonia, etc. were ruled out by appropriate clinical and laboratory methods. Out of 437 confirmed cases of leptospirosis, 167 (38.7%) had pulmonary involvement. A total of 65 had an ALI score ≥ 2.5 and were included in the study. Treatment protocol All patients were given the following treatment: (1) Inj. Crystalline penicillin 2 x 10 6 units intravenously 6 hourly, (2) Inj. Methyl prednisolone 1 gram intravenously daily for 3 days, followed by oral prednisolone 1 mg per kg of body weight for 7 days, (3) Non invasive mechanical ventilation) was used where necessary. There are studies to indicate that non invasive ventilation is an affordable alternative to treat patients with severe acute lung injury. [9],[14] Blood component therapy was given as and when indicated. Out of the first 32 patients who had been given this treatment, only three survived. In view of the poor outcome in the initial 32 patients, and considering the fact that immune mechanisms are important in its pathogenesis, the next 33 patients were given a trial of cyclophosphamide. They were all given injection cyclophosphamide 60 mg/kg body weight intravenously immediately upon the diagnosis of severe pulmonary hemorrhage. Mesna (2-MercaptoEthane Sulfonate sodium) was also given to prevent hemorrhagic cystitis. Monitoring and outcome Chest X-rays were taken at regular intervals. Blood total counts were taken daily for 21 days. Platelet counts, liver function tests, and renal function tests were performed at regular intervals. All patients who survived were observed in the hospital for 21 days or until the total counts returned to normal, whichever was longer. Survival was taken as the outcome indicator. Statistical analysis Survival rates were compared between the two groups: Group I - patients who were given cyclophosphamide and Group II - patients who were not given cyclophosphamide. Odds ratio and p-value were calculated to assess the statistical significance of the study. In view of the life-threatening nature of the disease, a randomized trial was not possible. Results A total of 33 patients were enrolled for treatment with cyclophosphamide (Group I). Of these patients, 26 were males. The mean age of the patients was 33 years old. The youngest patient was 17 years old and the oldest patient was 60 years old. The group of patients who had not been given cyclophosphamide had similar demographic characteristics [Table - 1]. All were farm laborers by occupation working in either paddy or sugarcane fields which are water logged. [Table - 2] shows the symptomatology of the two groups. Fever, myalgias, and headache were the most common symptoms. Although all the patients had pulmonary hemorrhage, cough and hemoptysis were present in only a small percentage of patients. As a matter of fact, tachypnoea was the best clinical indicator of pulmonary involvement. [Table - 3] shows organ involvements in the two groups. Eleven patients were given platelet transfusions in the treated group while 14 patients were given platelet transfusions in the control group. None of the patients required dialysis. As already mentioned, all patients in both the groups required non invasive ventilation, BiPAP, with positive end expiratory pressure {PEEP}. In the patients who survived, the median duration for which mechanical ventilation was required was 122 hours in Group I and 128 hours in Group II. The mean duration was 124.8 hours SD ± 30.31 and 123.3 hours SD ± 9.8 in Groups I and II, respectively. Leucopenia and alopecia were the main side effects noted. A total of 26 patients (78.78%) developed leucopenia. The lowest total white blood cell (WBC) count noted was 400. The median duration after which maximum leucopenia was noted was 10 days while the mean duration was 10.05 SD + 0.99. All patients were given colony stimulating factor and broad spectrum antibiotics. The median time taken for the total WBC count to return to normal was 17 days while the mean was 17.33 SD ± 0.84. Three patients developed a secondary infection. Two of them developed pneumonia while one patient developed a urinary tract infection. All of them had complete recovery. None of the patients died due to leucopenia or any other side effects. Six (18.75%) patients developed alopecia. None of the patients developed hemorrhagic cystitis, obviously due to the simultaneous administration of Mesna (2-MercaptoEthane Sulfonate sodium). Platelet counts improved in patients who survived. The average duration for the clearance of opacities from the lungs was seven days. In the group of patients who had been given cyclophosphamide, 22 out of 33 patients survived (66.7%) while in Group II three out of 32 patients survived (9.4%) [Figure - 1] and [Figure - 2]. Statistical analysis The odds ratio was 19.33 (4.22-102.1) indicating that survival was 19.33 times more among those who were given cyclophosphamide as compared with those who were not treated with the drug. The P-value was < 0.001 indicating that the association between survival and treatment with cyclophosphamide was statistically highly significant. Discussion There was a male predominance in this study. This is explained by the fact that all the patients are farm laborers and there are more males in this profession. Predominance of younger patients can also be explained in the same way. Mainly, two mechanisms have been proposed for the pathogenesis of lung injury in leptospirosis: a toxin mediated mechanism and/or exacerbated immune responses of the host. [1] There is evidence to suggest that immune mechanisms play a key role in the pathogenesis of pulmonary alveolar hemorrhage due to leptospirosis. Some of the more important mechanisms are as follows:
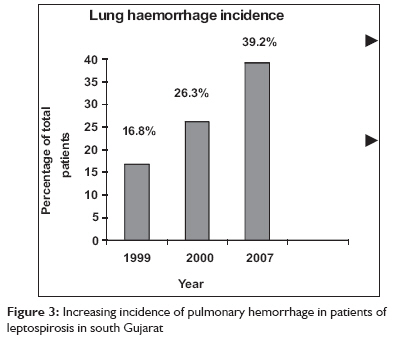
The changing pattern of leptospirosis has been observed by us in south Gujarat as well. We reported 16.8% and 26.3% incidences of pulmonary involvement in studies carried out in 1999 and 2000, respectively. [8],[2] The present incidence of 38.7% in 2007 is much higher, indicating an increasing involvement of the lungs [Figure - 3]. More alarming than the increasing incidence of pulmonary involvement is the increasing severity of the disease. We had found glucocorticosteroids to be quite effective in our study conducted in 1999. [8] But in the present study, the response to glucocorticosteroids was very poor. The explanation put forward by Abdulkader, et al. is applicable to our observations as well. South Gujarat has been witnessing leptospirosis since 1997. [2] In the initial years, we received patients who were infected for the first time, hence the disease was mild. But as the disease became endemic, patients started to have reinfection. The second infection is more severe in a manner similar to dengue. [24] As leptospirosis is an infection, antibiotics have been used for a long time as treatment. In the Cochrane database review, Guidugli, et al. looked at the role of antibiotics in the treatment of leptospirosis. [25] The review of trials found there was not enough evidence to show the benefit or safety of antibiotics for leptospirosis. There is no evidence of resistance to the traditionally used antibiotics such as penicillin. [1] Thus, changing the antibiotics or increasing their dosages will not help in decreasing the mortality rates. Thus, we have gathered the following evidence so far:
Abdulkader et al. have carried out a serological study to suggest an exacerbated immune response of the host as an important mechanism of pathogenesis. We have postulated that the same is operative in South Gujarat but serological studies should be carried out to validate our hypothesis. We conclude that cyclophosphamide therapy is very useful in the treatment of pulmonary alveolar hemorrhage due to leptospirosis. It provides a new tool for the treatment of this dreaded disease. At the same time, it also provides added supportive evidence for the hypothesis that immune mechanisms play a pivotal role in the pathogenesis of this disease. Acknowledgements The authors wish to thank Dr. Abhay Kavishwar, Associate professor, Community Medicine Department, Government Medical College, Surat for the help rendered in carrying out statistical analysis. References
Copyright 2009 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm09018f1.jpg] [cm09018f3.jpg] [cm09018t2.jpg] [cm09018t3.jpg] [cm09018t1.jpg] [cm09018f2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}