 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Critical Care Medicine, Vol. 15, No. 2, April-June, 2011, pp. 88-95 Research Article Hot climate and perioperative outcome in elderly patients Parshotam Lal Gautam, Sunit Kathuria, Sunita Chhabra Department of Anaesthesiology, Dayanand Medical College and Hospital, Ludhiana, Punjab, India Correspondence Address: Parshotam Lal Gautam, 61, Ashok Vihar, Rishi Nagar, Ludhiana - 141 001, Punjab, India, parshotamg@yahoo.com Code Number: cm11023 DOI: 10.4103/0972-5229.83013 Abstract Background: It is well known that heat wave is a major cause of weather related mortality in extreme of ages. While auditing our hospital mortality record, we found higher surgical mortality in the months of summer season which inspired us to look into the impact of hot climate in elderly surgical patients.Materials and Methods: An observational prospective cohort study was undertaken to study the impact of hot climate on elderly (age > 60 yrs) surgical patients over one year when outside temperature was more than 20 o C. 98 elderly patients requiring general anaesthesia for surgery were enrolled. Patients were grouped on the basis of peak outdoor temperature with a cut off value of 30 o C. Group I- when peak outdoor temperature ranged between 20-30 o C (comfortable zone) and Group II - when peak outdoor temperature ranged above 30 o C. To reduce the bias, inclusion and exclusion criterion were defined. Meteorological factors, patient characteristics, surgical risk factors and other related data were noted. Data was analyzed using student's't' and z-test for statistical significance. Results: There were statistically significant complications and prolonged hospital stay in group II as compared to I (13.21±6.44 Vs 9.81±3.54 days, P value =0.01) on univariate analysis. High risk patients had more complications in hot weather. Stepwise multivariate regression analysis showed higher adverse impact of poor physical and cardiac status than hot climate. Conclusion: Hot and humid weather adversely affect the perioperative outcome in elderly surgical patients. Patients with poor reserves are at greater perioperative risk during hot and humid climate. Keywords: Elderly, hot climate, perioperative outcome Introduction It is widely recognized that extreme climatic conditions constitute a major public health hazard. Epidemiological surveys and reports on heat wave have shown that the elderly population is particularly at a high risk of developing complications and heat-related mortality. [1],[2],[3],[4],[5] Heat-related illness may range from trivial heat injury to life-threatening emergencies. As there is gradual global warming, the threat of intermittent heat wave on human life is increasing day by day. At the same time, we have to accept the fact that despite preventive measures by the national and international organizations to stop progression of unfavorable climatic change, the hot climatic trend may be delayed but cannot be stopped. It is expected that these heat waves may increase in frequency, severity and duration to a discernible extent. This hot climate threat is going to be a concern of all health care specialties. While auditing our hospital mortality record of the last couple of years in the surgical population, we found high peaks of mortality in July and August [Figure - 1], which correspond to the summer months, with very high humidity levels in this region, which inspired us to look into the heat-related surgical morbidity prospectively. Although a lot of epidemiological studies have been carried out in hot climatic conditions for various aspects, very little has been studied in the surgical patients. Secondly, most of these surveys are either from western regions or from well-developed countries with good living conditions. Thirdly, temperature variations, other meterological factors and patient characteristics are different in India. It is well known that cardiac output increases to compensate for increased blood flow to skin. As most of the earlier work is done in the developed and western population, their results cannot be extrapolated to developing countries like India, where many are exposed to constant hot and humid weather because of poor living conditions and facilities. As our hospital record witnessed peaks of surgical deaths in the summer season, we planned this prospective cohort study to determine the impact of hot climatic conditions in elderly surgical patients over 1 year. Materials and Methods After approval from the institutional ethics committee and written informed consent from patients, an observational prospective cohort study was undertaken to study the impact of hot climate on elderly (age >60 years) surgical patients over a period of 1 year. All patients reporting to the surgical suite were screened for eligibility to the study. Patients were included in the study irrespective of their characteristic, American Society of Anesthesiologists (ASA) physical status, cardiac status and nature of surgery once the ambient temperature crossed 20°C. We considered peak ambient temperature at the time of admission as our reference point. To minimize the bias due to medical problems and adaptation of body in the hospital air conditioned environment, the exclusion criterion were designed as follows:
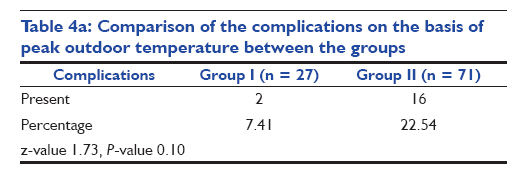
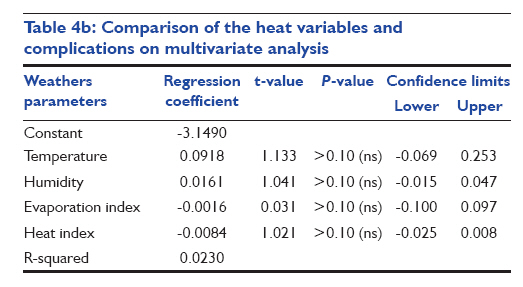
Ninety-eight elderly patients requiring general anesthesia for surgery were enrolled in this study. Subjects were grouped on the basis of peak ambient temperature with a cut-off value of 30 o C. We took 20-30 o C as a control as, in this range, the human body is comfortable. Group I - when peak ambient temperature ranged between 20 and 30 o C. Group II - when peak ambient temperature ranged above 30 o C. Peak ambient temperature, relative humidity and evaporation index were noted daily from Meteorological Department, Punjab Agricultural University, Ludhiana, Punjab, India. Heat index was derived from the above-noted value with the formula given below. [6] Humidex or heat index are the commonly used indices to study the effect of temperature and relative humidity. Heat index (HI) or apparent temperature (AI) = -42.379 + 2.04901523 (Tf) + 10.14333127 (RH) - 0.22475541 (Tf) (RH) - (6.83783 x 10 -3 ) (Tf 2 ) - ((5.481717 x 10 -2 ) (RH 2 ) + ((1.22874 x 10 -3 ) (Tf 2 ) (RH) + ((8.5282 x 10 -4 ) (Tf) (RH 2 )) - ((1.99 x 10 -6 ) (Tf 2 ) (RH 2 ) Tf = Temperature in Fahrenheit RH = Relative humidity All patients included in the study were assessed pre-operatively. The pre-operative evaluation included complete history, general physical examination, clinical signs of heat dysfunction, patient′s urine output and daily approximate fluid intake. Patient′s risk stratification was carried out on the basis of ASA physical status, Detsky scoring [7] and Shoemaker risk criteria [8] to test the impact of bias due to different patient clinical profiles. Detsky scoring and Shoemaker risk criteria were used to assess the cardiovascular and surgical risk, respectively. Nature, type of surgery (emergency/elective), pre-operative vitals and reports of routine investigations were also recorded. Intra- and post-operative data related to surgical risk factors, duration of anesthesia, vitals record and complications were noted. Vitals were recorded every half an hour intra-operatively and then every hour for the first 2 h, every 2-hourly for the next 24 h and then daily during the post-operative hospital stay. Perioperative complications such as hypotension, tachycardia/bradycardia, dysarrhythmias, myocardial infarction, respiratory distress, oliguria, anuria, acute renal failure, liver dysfunction or multiple organ dysfunction syndrome, etc., if any, were recorded with the time of episode. Hypotension was defined when the systolic blood pressure was <90 mmHg, tachycardia when heart rate was >100/min, bradycardia when heart rate was <60/min, myocardial ischemia as evident from chest pain and ST depression on EKG/monitor. Respiratory distress was defined as a respiratory rate >35/min or <6/min, use of accessory muscles, PaO 2 <60 mmHg on room air and PaCo 2 >40 mmHg or <35 mmHg in ABG (if performed). Oliguria was defined as urine output <400 ml/24 h and anuria as urine output <100 ml/24 h. The PACU stay, ICU stay and hospital stay were noted. All patients showing signs of post-operative ischemia or unexplained hypotension were subjected to troponin-T investigation to rule out MI. Post-operatively, patients were also observed for signs of septicemia (as evident from fever, increased WBC count or culture report). Outcome of patients was evaluated and compared in the form of incidence of complications and hospital stay. All these observations were noted in the proforma and analyzed using Student′s "t"-test and z-test for statistical significance. Stepwise multivariate regression analysis was used to determine the impact of risk variables on morbidity. Results It was difficult to plan a prospective study in view of the mixed patient profile because of different socioeconomic status, type of surgery and other surgical risk factors. Being a pioneer study, a convenient sample of all patients coming to the hospital for surgery under general anesthesia and who fulfill the criteria for enrollment was taken over a period of 1 year. We enrolled 98 patients when the peak ambient temperature was above 20°C. Patents were grouped into two groups with a cut-off value of 30°C keeping in mind comfort (control group) and non-comfort heat zone (study group). This resulted in a small sample size of the control group. Heat variables have a significant difference between the two groups. Relative humidity was higher in group I as compared with group II, with a low evaporation index in group I as compared with group II, counteracting some effects of higher temperature. The heat index was high in both the groups, but the difference was statistically significant. There were 27 patients in group I and 71 patients in group II. Age, physical status and risk profiles and type of surgeries of patients were comparable [Table - 1] and [Table - 2], [Figure - 2]. Average age among groups I and II were 66.81 ± 5.74 and 68.08 ± 6.34, respectively. Most of the patients belonged to ASA I-III. Group I had more ASA I patients (37%) as compared with group II (9.8%) and group II had more ASA II patients (45%) than group I (26%). However, patient distribution among groups as per the risk stratification for ASA III, ASA IV, Detsky score and Shoemaker′s rRisk criteria were comparable. All heat variables: ambient temperature, evaporation index and heat index, had a high statistically significant difference between the two groups [Table - 3] and [Figure - 3]. Temperature and heat index had a highly significant difference between the two groups (P = 0.001). Relative humidity was high among both groups I and II (96.48 ± 2.76 and 82.03 ± 14.40, P = 0.01). Evaporation index was higher in group II as compared with group I (P = 0.001), counteracting the effect of high temperature and relative humidity. As relative humidity remained in a higher range in both groups, heat index also remained high in both the groups; group I (103.29 ± 18.58) and group II (166.79 ± 18.25). However, the difference was wide and statistically significant. There were more complications in group II as compared with group I [Table - 4a & b]. Further, there was more complication in the high-risk patients in group II. There were more complications related to the cardiorespiratory system. Complications had a similar positive corelationship with all heat variables except evaporation index, which had a t-value of 0.031 as compared with temperature (1.133), humidity (1.041) and heat index (1.021) [Table - 5]. On multivariate analysis, the impact of heat variables was less than that of ASA physical status, Detsky score and Shoemaker′s risk criteria [Table - 6] a, [Figure - 4] and [Figure - 5]. Patients had a prolonged hospital stay of 13.21 ± 6.44 in group II as compared with group I (9.81 ± 3.54 days) [Table - 7] and [Figure - 6]. Discussion Global warming is emerging as a threat to the survival of human beings in the coming future. There are a number of epidemiological surveys to address the heat wave [8,9] and heat wave-related morbidity and mortality. [1],[2],[3],[4],[5],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21],[22],[23] In a study by Nakai S et al., the authors observed that heat-related deaths were more prone to occur during the day, with peak daily temperatures of >38 o C, and the incidence of these deaths showed an exponential dependence on the number of hot days. Furthermore, most deaths were reported either in children (<4 years) or in the elderly (>70 years). [1],[2] In the last decade, numerous epidemiological studies related to heat wave appeared in the literature from Italy, [1],[11] USA, [2],[13],[14],[15],[16],[17],[18],[19] Japan, [3] France, [5] Belgium [9] and many other countries. There were similar deaths tolls in reports, raising an alarming concern for global warming and related heath issues. Among the hot climatic elements or parameters that affect the human body, the more important are temperature, humidity, wind, evaporation and sunshine. Acting together, these elements influence the body′s comfort and well being. [20],[21],[22] In addition to environmental heat, body heat is gained from cellular metabolism and the mechanical work of the skeletal muscle. Maintenance of body temperature is very complex. For maintaining a body temperature of 37°C, the overall heat load must be dissipated. Evaporation is a primary way of heat loss when the environmental temperature is higher than that of the body. During humid climate, this process is restricted, resulting in uneasiness and discomfort. Lungs and skin account for 600 ml of water loss/day. Continuous active evaporation without adequate water intake poses a risk of dehydration and heat-related illness. Hypovoluemia interferes with thermoregulatory adaptation by decreasing the cutaneous blood flow and sweat rate. The body adapts by various physiological responses. It has been found that most of the acclimatization occurs in first week. The body adapts by various physiological responses. Active sympathetic cutaneous vasodilatation increases the blood flow in the skin up to 8 L/min. An elevated blood temperature also causes tachycardia and tachypnoea, augmenting heat loss through lungs and skin. If the body is given sufficient time, it will gradually become adapted to living and working in a hot environment. [20] This cohort was planned with the hypothesis that if any surgery is carried out in the period prior to adaptation, it may have more complications. We found that patients had statistically significant complications when the peak ambient temperature was higher (group II; 38.2 ± 2.96°C) as compared with the comfortable temperature zone (group I; 28.41 ± 1.63°C). 22.54% patients in group II had complications while in group I, only 7.41% patients had complications (P < 0.10). In group II, two patients had three acute respiratory distress syndrome, two acute renal failure, one myocardial infarction and two multiple organ failure syndrome. Hospital stay was also prolonged statistically when the peak outdoor temperature was higher (P = 0.01). The overall outcome was better in group I than in group II. High-risk patients with poor cardiorespiratory reserve are at a greater risk of complications. Inglis et al. also found seasonal variations in cardiac failure patients in the Australian population in the summer season. [23] Semenza documented a higher incidence of acute renal failure during heat wave. [24] Patients in group II have prolonged hospital stay, but it is difficult to comment whether prolonged stay resulted in more complications or complications resulted in prolonged stay. Infections were not monitored strictly. As chronic dehydration is common in hot weather, particularly in sick patients, it may increase the risk of infection due to gut ischemia. [5] Secondly, type of the surgery and surgical risk factors can bias the results. However, in our study, the nature and type of surgery were similar between the two groups. We found that patients with poor ASA physical status had more complications in group II. We also found that patients with a higher Detsky score or poor Shoemaker′s risk had more complications when the ambient temperature was high. On stepwise multivariate regression analysis, it was found that poor ASA status, Detsky score and Shoemaker′s risk had a greater impact on morbidity as compared with hot weather. Probably, it was the poor cardiorespiratory reserve of the patients that failed to cope with the added adverse weather stress. A comparison among heat variables showed similar effects. We also compared various heat variables in relation to morbidity. There was no statistical difference in the tools used. However, their "t" values were of order as follows: temperature = 1.33, relative humidity = 1.041, evaporation index = 0.031 and heat index = 1.021. There is only one prospective study carried out on intensive care patients evaluating the effect of ambient temperature on core body temperature, and the authors found hyperthermia in these patients. [22] Most of the data and literature available are either from western countries or from well-developed south eastern countries. The impact of hot weather on the Indian population may be different from that of the population of the western and well-developed countries. They probably may be more adapted and genetically different also. Secondly, as change in temperature in this part of the country is often gradual over many days, these subjects might have adapted to some extent also. During the summer months, spells of hot weather occasionally occur over certain parts of India. These spells are often seen to move from one region to another. In places where the normal temperature itself is high and rise in temperature is slow, people become adapted to that temperature. Considering environmental and subject differences, it is important to review our local environmental values and impacts. But, there are very few studies from India or Pakistan. These authors found climate and its variations different from the western and other worlds as well. Considering these aspects, the India Meteorological Department (IMD) has defined heat wave differently in two categories. The first category includes places where the normal maximum temperature is greater than 40°C. In such regions, if the day temperature exceeds by 3-4°C above the normal, it is said to be affected by a heat wave. Similarly, when the day temperature is 5°C or more than the normal, severe heat wave conditions persist. The second category considers the regions where the normal maximum is 40°C or less. In these areas, if the day temperature is 5-6°C above the normal, then the place is said to be affected by a moderate heat wave. A severe heat wave condition exists when the day temperature exceeds the normal maximum temperature over the place by 6°C. A recent study by Sinha Ray et al. has shown that the average annual loss of human life due to heat wave over India is 153. [25] In a report from the IMD, it has been observed that the most affected states were where the normal temperature was greater than 40°C. [25] These authors have also noted that loss of human lives were more in regions with poor socioeconomic conditions of the people than in a state with better living conditions. [25],[26] They also mentioned that the impact of heat waves over Bihar, Punjab and parts of Maharashtra was more as it may create more water scarcity and adversely affect agriculture. These authors also correlated heat wave mortality with El-Nino events. Secondly, living conditions, regional metrological factors, socioeconomic status and genetic predisposition of patients are all different. However, statistical significance has poor strength as the sample size was too small for intragroup comparison. Secondly, there were regional factors also that probably interfered in interpreting the observations. Our patients were mainly from the northern part of India, particularly Punjab state, which is an agricultural state with few industrial cities. Our patients were a mix-up of farmers and industrial laborers. They work for long hours in fields and factories without an air conditioned facility. Although both these population subsets work in similar hot and humid conditions, providing a suitable observational ground for study, these patients differ in a number of other aspects. Industrial pollution has its own detrimental effect. At times, the compounding effect of a high level of industrial smoke and high Humidex has resulted in respiratory distress in stable chest patients in this city. More so, the living conditions are also different. Many are exposed to poor living conditions because of poor socioeconomic status. Their nutritional standards are different with variable body immune defense. Being a pioneer work, there are limitations in our study, the major one being poor power because of the small sample size in group I. Other bias factors such as different types of surgeries, ASA status variations, polluted weather, academic cycle, type of emergency, infections, etc. need to be adjusted to minimize bias. We did not include the vulnerable group categorically, except the age group. There is enough literature analysis on heat vulnerability factors. [4],[26] Heat vulnerability varies spatially, on local, regional, national and international scales. Even within the same city, in addition to the regional difference in heat vulnerability, a higher vulnerability had been seen within the downtown areas of all cities compared with the suburban areas, regardless of the city′s overall vulnerability. Conclusions Hot and humid weather adversely affects the outcome in terms of prolonged hospital stay and complication rate in elderly surgical patients. Patients with poor cardiorespiratory indices had a higher adverse impact of weather. Impact of poor physical status was higher than poor climate. There is need to explore the impact of hot and humid weather in the vulnerable group of patients such as laborers working in fields coming for emergency surgery. Different heat variables have a similar effect on patient outcome. Future directions Keeping in mind the study design limitations and sample size, this ground breaking idea needs further corroboration with a large sample size in suitable high-risk patients to reduce the bias of hidden variables. We need to consider the affects of confounding factors such as air pollutants, socioeconomic status, living conditions, job profiles, rate of change of weather, etc. to study the impact of heat-related morbidity. We need to focus on multiple regions individually also as geographical and racial differences affect the results. As hot weather affects farmers and industrial laborers because of prolonged sun exposure in the harvesting season and hot humid polluted environment, respectively, this study may be more focused on this vulnerable subgroup to study the discernible impact. We also hypothesize that stabilization of patients in an air conditioned environment for 48 h in a hot climate prior to surgery may reduce the complication rate and improve the surgical outcome, especially in patients with poor reserve. This study opens a new area for exploration in an era of global warming. Acknowledgment The authors would like to thank Mr. Ashok Chopra, Chief Record Officer, Dayanand Medical College and Hospital, Ludhiana, Punjab for providing hospital record. The authors would also like to thank Dr. Prabhot Kaur, Agrometeorologist, Punjab Agricultural University, Ludhiana, Punjab for providing meteorological data. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11023f5.jpg] [cm11023f1.jpg] [cm11023t6.jpg] [cm11023t2.jpg] [cm11023t7.jpg] [cm11023t4a.jpg] [cm11023t4b.jpg] [cm11023t1.jpg] [cm11023f6.jpg] [cm11023f2.jpg] [cm11023t5.jpg] [cm11023f4.jpg] [cm11023t3.jpg] [cm11023f3.jpg] |
| |||||||||

![[Figure - 1]](/showimage?cm/photo/cm11023f1.jpg){kind=link}
![[Table - 1]](/showimage?cm/photo/cm11023t1.jpg){kind=link}
![[Table - 2]](/showimage?cm/photo/cm11023t2.jpg){kind=link}
![[Figure - 2]](/showimage?cm/photo/cm11023f2.jpg){kind=link}
![[Table - 3]](/showimage?cm/photo/cm11023t3.jpg){kind=link}
![[Figure - 3]](/showimage?cm/photo/cm11023f3.jpg){kind=link}
{kind=link}
{kind=link}
![[Table - 5]](/showimage?cm/photo/cm11023t5.jpg){kind=link}
![[Table - 6]](/showimage?cm/photo/cm11023t6.jpg){kind=link}
![[Figure - 4]](/showimage?cm/photo/cm11023f4.jpg){kind=link}
![[Figure - 5]](/showimage?cm/photo/cm11023f5.jpg){kind=link}
![[Table - 7]](/showimage?cm/photo/cm11023t7.jpg){kind=link}
![[Figure - 6]](/showimage?cm/photo/cm11023f6.jpg){kind=link}