 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
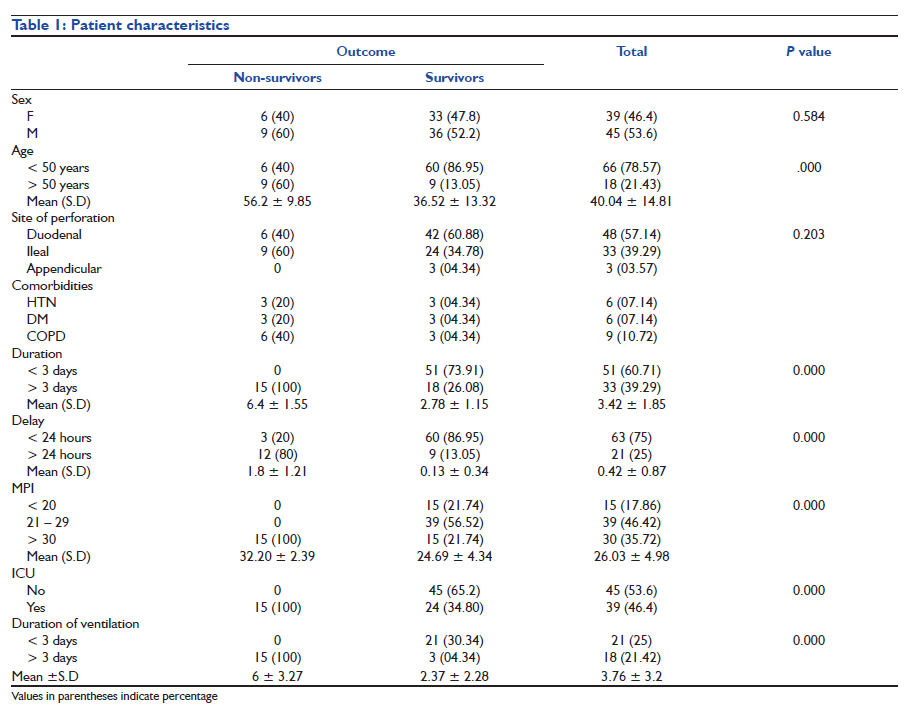
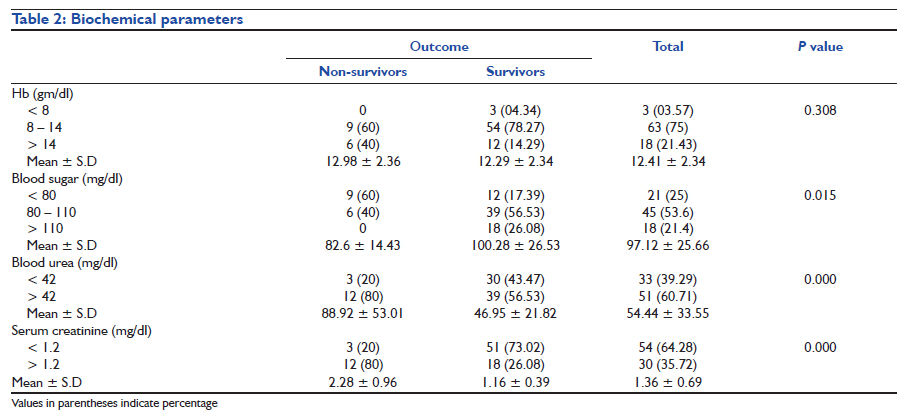
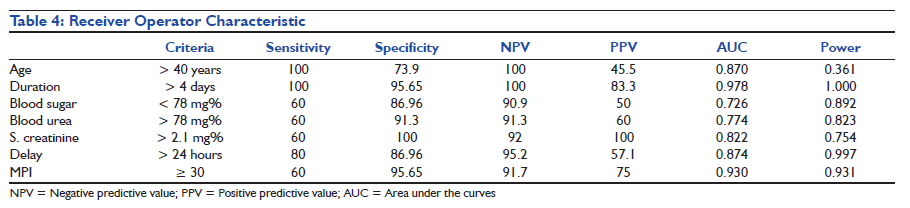
Indian Journal of Critical Care Medicine, Vol. 15, No. 3, July-September, 2011, pp. 157-163 Research Article Preoperative predictors of mortality in adult patients with perforation peritonitis Ranju Singh1, Nishant Kumar2, Abhijit Bhattacharya3, Homay Vajifdar1 1 Department of Anesthesiology and Critical Care, Lady Hardinge Medical College and Shrimati Sucheta Kriplani Hospital, New Delhi, India Code Number: cm11040 DOI: 10.4103/0972-5229.84897 Abstract Introduction: There is paucity of data from India regarding the etiology, prognostic indicators, morbidity, and mortality patterns of perforation peritonitis. The objective of our study was to evaluate the predictors of mortality, preoperatively, for risk stratification of the patients and institution of an early goal-directed therapy. Keywords: Blood sugar, blood urea, delay, duration of peritonitis, Mannheim peritonitis index, perforation peritonitis, mortality, pH, serum creatinine, serum lactate levels, standard base excess Introduction Peritonitis due to perforation of the gastrointestinal tract is one of the most common surgical emergencies all over the world. [1] There is paucity of data from India regarding its etiology, prognostic indicators, morbidity, and mortality patterns. [2] Despite advances in surgical techniques, antimicrobial therapy, and intensive care support, management of peritonitis continues to be highly demanding, difficult, and complex. [3] A majority of the patients present late, with septicemia, [4] thus increasing the incidence of morbidity and mortality and complicating the task of the anesthesiologists to provide optimal perioperative care in these patients. Early prognostic evaluation of abdominal sepsis is desirable to select high-risk patients for more aggressive therapeutic procedures and to provide objective classification of the severity of the disease, [5] as also to choose the optimal perioperative anesthetic management strategies. There is an indication that patients with peptic ulcer perforation are septic upon admission, and thus might benefit from a perioperative care protocol with early source control and early goal-directed therapy according to The Surviving Sepsis Campaign. [6] Various factors have been used previously to reflect the severity of sepsis, as markers of mortality. The most commonly associated are age, [3],[6],[7],[8],[9],[10],[11] serum lactate levels, [12],[13],[14] acidosis (pH), [6],[15] base excess, [16],[17] and multiple organ failure. [5],[6],[10],[18],[19],[20],[21],[22] Similarly, various scoring indices such as the Acute Physiology and Chronic Health Evaluation (APACHE) score, [18],[22],[23] the Simplified Acute Physiology Score (SAPS), [18] the Boey Score, [23],[24],[25] the Multi Organ Failure (MOF) Score, [18],[22] and the Mannheim Peritonitis Index (MPI) [5],[18],[19],[20],[21],[25] have been introduced to stratify the risk in such patients. However, apart from MOF Score and the MPI, none is specific for peritonitis alone. Moreover, while these indices are tedious and difficult to implement, the others incorporate the intraoperative and postoperative statuses as well. The objective of our study was to evaluate pre operative predictors of mortality in patients presenting with perforation peritonitis for surgical management in the emergency department. Materials and Method After approval from the Institutional Ethics Committee, 84 patients presenting with perforation peritonitis, in the age group of 14 - 70 years, of either sex, scheduled for an emergency laparotomy, were studied prospectively from January 2007 to March 2009. The diagnosis was clinical, based on guarding, rigidity, and tenderness on palpation of the abdomen and confirmed radiologically, by the presence of gas under the diaphragm, on an X-ray film. Informed consent was taken from each patient. All patients with perforation peritonitis who were managed conservatively, were excluded. Cases of spontaneous bacterial peritonitis, colonic perforations, peritonitis due to malignancy, trauma and corrosives, and postoperative peritonitis due to anastomotic leak were also excluded from the study. Patients who were deemed to be septic, that is, with more than two features out of tachycardia (heart rate > 90 beats/min), tachypnea (respiratory rate > 20 breaths/min or PaCO2 < 32 mmHg), hypo- or hyperthermia (temperature > 38°C or < 36°C), and total leukocyte count < 4000/cumm or > 12000/cumm or band forms > 10%, were included. The patients were investigated (complete hemogram, liver and renal function tests, serum electrolytes, random blood sugar, and blood gas analysis), and received a standard regime of broad spectrum antibiotics and their electrolyte and fluid status was optimized before surgery. All patients received general anesthesia with tracheal intubation and positive pressure ventilation. Intraoperatively, electrocardiogram (ECG), heart rate, oxygen saturation (SpO2), non-invasive blood pressure (NIBP), end-tidal carbon dioxide (EtCO2), temperature, urine output, and central venous pressure were monitored. The decision to extubate the trachea or continue ventilation postoperatively was clinical. Patients whose trachea was extubated were shifted to the post-anesthesia care unit (PACU), whereas, those ventilated were shifted to the Intensive Care Unit (ICU). The parameters studied were age and sex of the patients, associated comorbidities, duration of symptoms, delay in initiating surgical intervention, and preoperative biochemical parameters, such as, hemoglobin, random blood sugar, blood urea, serum creatinine, pH, base excess, and serum lactate levels. In addition to the above-mentioned parameters, the Mannheim peritonitis index (MPI), postoperative ventilation, and the duration of ventilation were also studied with respect to the outcome. In-hospital mortality was taken as the outcome. Data analysis The data were collected from the anesthesia charts of the patients. A commercial software package (SPSS version 17.0 LTD, Chicago, IL, U.S.A) was used to analyze the data. The nominal and ordinal categorical data such as sex, associated diseases, site of perforation, and need for postoperative ventilation were analyzed by Chi-square / Mann Whitney U test. Other data were analyzed using independent samples t-test using the Bonferroni correction. A P value of ≤ 0.05 was taken to be significant. The Receiver Operator Characteristic (ROC) curve analysis was performed to find sensitivity and specificity of each variable. The area under the ROC curve > 0.8 was considered to be a good predictor of mortality. A multiple regression (linear, enter) analysis was performed. All the factors with a P value < 0.05 were included and entered to find out the independent factors contributing to the mortality. As it was not possible to conduct a pilot study and pre-calculate the sample size, post hoc power analysis was done. Result Of the 84 patients studied, 45 (53.6%) were males and 39 (46.4%) were females (P=0.584). The mean age was 40.04 ± 14.81 years. The mean age of the survivors was 36.52 ± 13.32 years as compared to 56.2 ± 9.85 years of the non-survivors (P<0.001). The site of perforation in the gastrointestinal tract and the associated comorbidities are depicted in [Table - 1]. All patients were septic on admission. The mean duration of the symptoms was 3.42 ± 1.85 days; all the 15 patients who died had symptoms for more than three days (6.4 ± 1.55 days). Eighteen of the 69 survivors had symptoms for more than three days (2.78 ± 1.15 days, P<0.0001). The surgical intervention was initiated within the first 24 hours of admission in 63 (75%) of the patients. Twelve non-survivors (80%) were operated upon more than 24 hours after admission (1.8 ± 1.2 days), whereas 86.95% of the survivors (60 patients) were operated upon the same day (0.13 ± 0.33 days, P<0.001) [Table - 1]. The overall mortality rate was 17.86% (15 patients). The mean hemoglobin was comparable among the survivors (12.29 ± 2.33 gm/dl) and non-survivors (12.98 ± 2.36 gm dl-1, P=0.308). Sixty percent of the nonsurvivors were hypoglycemic (mean 82.6 ± 14.4 mg/dl, P=0.015). The survivors on the other hand were either euglycemic (56.53%) or hyperglycemic (26.08%), with a mean blood sugar level of 100.28 ± 26.53 mg/dl. The renal function tests too were deranged in the nonsurvivors, with mean blood urea levels of 88.92 ± 53.00 mg/dl and serum creatinine levels of 2.28 ± 0.96 mg/dl. The survivors had mean blood urea (46.95 ± 21.81 mg/dl, P<0.001) levels and serum creatinine levels (1.16 ± 0.39 mg/dl, P<0.001) in the normal range [Table - 2]. The arterial blood gases revealed pH to be in the range of 7.35 - 7.45 in 40% of the non-survivors and 52.18% of the survivors (P=0.856). The mean base deficit was -1.52 ± 3.16 and -2.61 ± 3.65 in the non-survivors and survivors, respectively (P=0.287). The lactate levels were higher in survivors with a mean of 2.6 ± 1.14 mg/dl as compared to non-survivors (2.24 ± 0.46 mg/dl, P=0.146) [Table - 3]. Survivors had a mean MPI of 24.69 ± 4.35 as compared to 32.2 ± 2.4 in non-survivors (P<0.001). Intensive care unit (ICU) admission was required in 46.4% of the patients. All the non-survivors (15 patients) were admitted to the ICU and had to be ventilated postoperatively. The duration of ventilation in non survivors was more (6 ± 3.27 days) as compared to the survivors (34.8%, 2.37 ± 2.28 days, P<0.001). Multiple linear (enter) regression of variables with P<0.05 identified age, duration of symptoms, preoperative blood sugar levels, blood urea, serum creatinine levels, MPI, and the delay in instituting surgical intervention as the predictors of mortality. The sensitivity, specificity, area under the curves (AUC) and observed power are displayed in [Table - 4]. Discussion Perforation peritonitis is a frequently encountered surgical emergency in tropical countries like India, most commonly affecting young men in their prime of life. Most of these patients present with perforation of the upper gastrointestinal tract, commonly of the duodenum (57.14% in our study). In a majority of the cases, presentation to the hospital is late with well-established generalized peritonitis with purulent / fecal contamination and varying degrees of septicemia. Assuming that the patients with peptic ulcer perforation are septic upon admission, [6] the determinants of mortality in sepsis should hold true for perforation peritonitis as well. It is necessary to recognize patients at risk preoperatively and prepare for an intensive postoperative management strategy. This becomes more significant in our setup, where the intensive care facilities are limited and overwhelmed by the number of patients. Among others, age, [3],[6],[7],[8],[9],[11] sex, [9],[18] site of perforation, [5],[18],[19],[20],[21] preoperative shock, [3],[5],[18],[19],[20],[21] hypoglycemia, [26],[27] renal dysfunction, [3],[5],[6],[18],[19],[20],[21] the duration of symptoms, [3] and delay in surgical treatment, [3],[5],[9],[10],[11],[18],[19],[20] have been reported as the determinants of mortality in patients with perforation peritonitis. Similarly hyperlactatemia, [12],[13],[14],[15] lactic acidosis, [6],[15] increased Tumor necrosis factor (TNF), [28] procalcitonin levels, [29] and intramucosal gastric pH, [14] have been used as markers of hypoperfusion resulting from sepsis and are considered as indirect determinants of sepsis. Studies have shown that the results of elective surgery in elderly patients seem largely favorable, while those of emergency surgery are not. [30],[31] Cohen [9] and Seo et al., [8] have reported a high risk of mortality in persons over 60 due to multiple pathological processes proceeding concomitantly. Multivariate analysis in our study put forth age as one of the predictors of mortality. However, in contrast to age > 45 [Table - 1], age > 65 years had a sensitivity of just 20%, but a specificity and positive predictive value (PPV) of 100% for mortality. Most of our patients (39.29%) presented late to the hospital (after > 3 days of the appearance of symptoms). This is due to the fact that many of them were from the lower socioeconomic strata. They waited for the symptoms to improve by themselves or had taken traditional medicinal (Ayurveda, Unani) cures till they were referred to us or had to travel long distances to reach a referral center. Jhobta [3] and Afridi et al., [32] have stressed that delayed presentation to the hospital accounts for significant mortality. Kocer et al., [10] reported that patients who were admitted after 24 hours had a 3.4 times higher morbidity risk than patients admitted before 24 hours. The MPI also considers the duration of peritonitis > 24 hours as one of the factors contributing to mortality. Svanes et al., [11] have reported that a delay of more than 24 hours increases lethality from seven-fold to eight-fold, complication rate to three-fold, and length of hospital stay to two-fold, compared to a delay of six hours or less. The Receiver Operator Characteristic (ROC) curve analysis shows that the duration of symptoms of > 4 days is 100% sensitive and 95.65% specific for mortality. Similarly any delay in initiating the surgical treatment is 80% sensitive and 86.96% specific [Table - 4]. Only three out of 84 of our patients were anemic (Hb < 8 gm dl -1 ; 3.57%, P=0.308) and anemia was not found to be an indicator of mortality. Hypoglycemia during hospitalization occurs in patients with and without diabetes and has been associated with in-hospital increased mortality. [33],[34] Sepsis, starvation, [26] malignancy, and low serum albumin levels were risk factors for developing hypoglycemia. Depleted glycogen stores, impaired gluconeogenesis, and increased peripheral utilization may all be contributing factors. We found that hypoglycemia (< 80 mg/dl) was an independent predictor of mortality [Table - 4]. This becomes significant as none of the previous indices have included blood sugar level measurements. Starvation, frequent vomiting, and third space loss may lead to renal function derangement in patients with perforation peritonitis. Most of the scoring indices address this as an important marker for mortality. MPI [5],[18],[19],[20],[21] and MOF score include serum creatinine levels as one of the markers. Moller et al., [6] have also reported renal insufficiency on admission as an independent risk factor related to mortality, in patients operated for peptic ulcer peroration. ROC analysis of blood urea levels in our study (> 78 mg/dl) showed a sensitivity of 60% and a specificity of 91.30% with a PPV of 60%. However for levels > 92 mg/dl the specificity and PPV were 100%. Similarly the ROC analysis of serum creatinine levels of > 2.1 mg/dl showed a sensitivity of 60% and a specificity of 100% with a PPV of 100%. Resuscitation of surgical patients has traditionally been guided by the normalization of vital signs. However, these endpoints have revealed the inadequacy of relying solely upon vital signs in the resuscitation of critically ill patients. [35] Elevated blood lactate levels have been used to define the prognostic value of occult hypoperfusion in critically ill patients without signs of clinical shock. [36] Vorwerk et al., [12] reported a specificity of 74.3% for mortality with lactate levels of ≥ 4 mmol/ l in patients with sepsis. In a recent study, Mikkelsen et al., [13] reported that intermediate and high lactate levels are independently associated with mortality in severe sepsis, independent of organ failure and shock. We, however, found no correlation between initial lactate levels and mortality. Other markers of acidosis such as base deficit and bicarbonate levels have been considered as important outcome markers in conventionally resuscitated patients. [16] The standard base excess (SBE) can reflect a great amount of disturbances secondary to sepsis and resuscitation; [37] and low values at admission are associated with higher mortality in the ICU. [16],[17] However, serum lactate levels and base deficit do not appear to be always linked. Abnormalities in the acid base environment have been postulated as causes for this uncoupling. Lee et al., [15] and Moller et al., [6] however, ascertain metabolic acidosis as an independent predictor of mortality. Lee et al., [15] further maintain that serum lactate levels are closely related to metabolic acidosis in septic patients; lactic acidosis and not hyperlactatemia has been found to predict mortality in severe sepsis and septic shock patients. We, however did not find either the pH (P=0.856) or SBE (0.287) to be a predictor of mortality. Several scoring indices have been compiled to predict the prognosis of patients with sepsis. The Boey score encompasses only three factors - major medical illness, preoperative shock, and longstanding perforation ≥ 24 hours. The mortality rate increases progressively with an increasing number of risk factors: 0, 10, 45.5, and 100% in patients with none, one, two, and all three risk factors, respectively. [5] The MOF score considers the various organ systems and is tedious to apply. The MPI has eight parameters and a score ranging from 0 to 57. Accuracy of the MPI is comparable or slightly superior to that of other sepsis classification systems. [38],[39] Patients with a score < 21 have a reportedly low mortality (0 - 2.3%) as compared to those with a score > 29 (100%). Notash et al., [18] have reported a sensitivity of 79% and a specificity of 96% for an MPI of 29, as compared to a sensitivity of 60% and a specificity of 95.65% for an MPI of 30, in our study. Even though MPI has been shown to be an appropriate objective prognostic factor in patients with peritonitis [5],[19],[20],[22] it fails to take into account the delay in presentation to the hospital. Moreover, it takes the intraoperative findings into consideration. Our study aims to primarily look at the preoperative factors affecting mortality. This becomes advantageous for the anesthesiologist in deciding the intraoperative management and optimum postoperative management. Moreover, the factors included in our study are the basic laboratory investigations that are usually done before taking up the patient for surgery. In-hospital mortality rate due to perforation peritonitis has been reported to range widely from 9 [10] to 60%. [19] Although advances in intensive care and aggressive surgical techniques have been made, recent studies suggest an operative mortality rate ranging from 10 - 30%. [3],[6],[18],[32] The mortality rate of 17.8% in our study can be explained on the basis of delayed presentation (39.29% presented after three days of symptoms), elderly population, and delay in initiating surgical treatment (80% of those who died were operated upon > 24 hours after admission). In conclusion, there are various indices mentioned in literature to predict morbidity and mortality due to sepsis. However, only a few are specific for perforation peritonitis, but none of them take into account the preoperative factors and laboratory investigations. We conclude that the age of the patient, the duration of symptoms, delay in surgical intervention, preoperative blood sugar, blood urea, and serum creatinine levels are independent predictors of mortality in patients with perforation peritonitis. Recognizing such patients early may help anesthesiologists in risk stratification and in providing an early goal-directed therapy and optimal perioperative care; thus reducing the morbidity and mortality rates. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11040t1.jpg] [cm11040t4.jpg] [cm11040t3.jpg] [cm11040t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}