 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
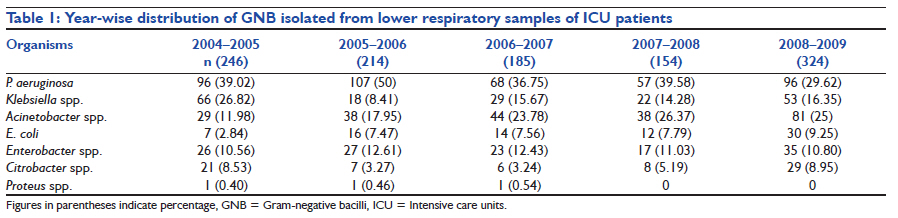
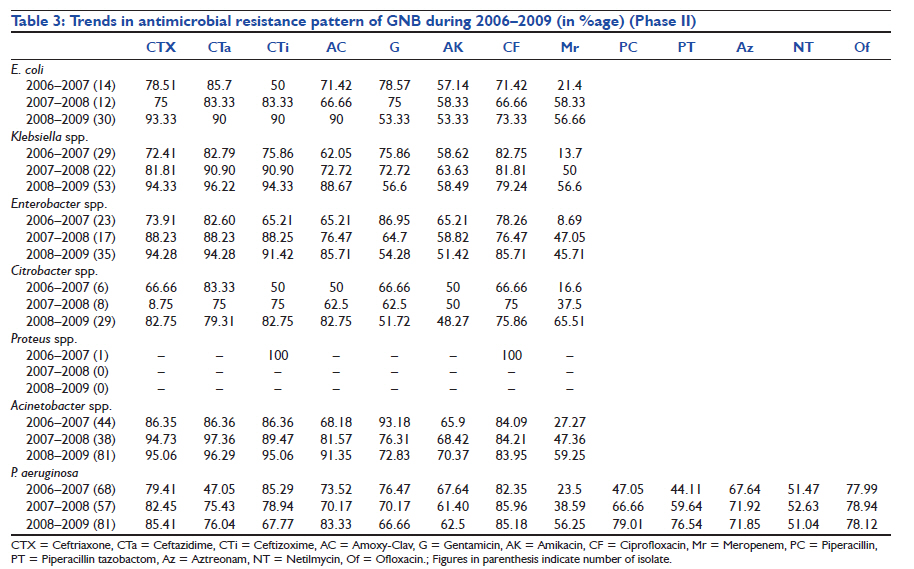
Indian Journal of Critical Care Medicine, Vol. 15, No. 3, July-September, 2011, pp. 164-167 Research Article Changing trend of antimicrobial resistance among gram-negative bacilli isolated from lower respiratory tract of ICU patients: A 5-year study Deep Gagneja, Nidhi Goel, Ritu Aggarwal, Uma Chaudhary Department of Microbiology, Pandit Bhagwat Dayal Sharma Post Graduate Institute of Medical Sciences, Rohtak, India Code Number: cm11041 DOI: 10.4103/0972-5229.84900 Abstract Background: Lower respiratory tract infections (LRTIs) are the most frequent infections among patients in intensive care units (ICUs).Aim: To track the resistance rate among the causative agents causing LRTI in the ICU patients. Design and Settings: This is a retrospective study done in a tertiary care hospital. Materials and Methods: Transtracheal or bronchial aspirates from 2776 patients admitted to the ICU were cultured and identified, and antibiotic sensitivity was performed by standard methods. Results: Of 2776 specimens, 1233 (44.41%) isolates were recovered, of which 1123 (91.07%) were gram-negative bacilli (GNB) and 110 (8.92%) were gram-positive organisms. From 2004 to 2009, Pseudomonas aeruginosa remained the most common pathogen. In phase I, high level of resistance (79-98%) was observed against all GNB. During phase II increasing trend in resistance to cephalosporins and declining trend in resistance to aminoglycosides against most GNB were observed. Multidrug resistance (resistance to three or more than three drugs) was observed in 83% of total isolates. Conclusions: Gram-negative organisms are the predominant pathogens causing LRTI in ICU. The increasing trend of resistance to cephalosporins and carbapenems in gram-negative organisms is very disturbing. Judicious use of antimicrobial agents is essential to prevent the emergence of multidrug-resistant bacteria in the ICU. Keywords: Gram-negative bacilli, intensive care unit, resistance trend Introduction Lower respiratory tract infections (LRTI) are the most common bacterial infections among patients in intensive care units (ICUs), occurring in 10-25% of all ICU patients and resulting in high overall mortality, which may range from 22 to 71%. [1],[2] A multicenter study conducted in 13 European countries indicated that respiratory tract samples (39%) were the most frequent source of bacterial isolates followed by blood (21%) and urinary tract (17%). [3] Most common bacterial agents of LRTI in the ICU are Pseudomonas, Acinetobacter, Klebsiella, Citrobacter, and Escherichia coli. [4],[5],[6] The incidence and associated mortality due to LRTI can be influenced by several factors including characteristics of the population at risk, standard of the healthcare facilities available, immunosuppressive drugs, inappropriate antibiotic therapy, distribution of causative agents, and prevalence of antimicrobial resistance. These factors may vary from one geographical region to the other. In almost all cases, eradication of causative agents requires initiation of antimicrobial therapy before obtaining culture report; however, during the last few years, the increase in antibiotic resistance has compromised the selection of empirical treatment. [7] The knowledge of likely prevalent strains along with their antimicrobial resistance pattern will help in better management of patients and framing the antibiotic policy. This study was conducted with the aim of tracking resistance rate among the causative agents of LRTI in ICU patients. Materials and Method The present retrospective study was conducted at the Microbiology Department of a teaching tertiary care hospital over a period of 5 years (July 2004-July 2009). Transtracheal or bronchoscopic aspirates were collected aseptically from the patients of all age groups and sex admitted to respiratory intensive care unit, who were on mechanical ventilation for at least 3 days. Samples of only new patients who were enrolled for the first time were included in the study. Single or mixed growth from one patient and consecutive samples from the new patients were included in the study. If the repeat sample was received from the same patient who was already enrolled, it was not included in the study. All the specimens received were immediately plated on the blood agar and Mac-Conkey agar by semiquantitative method and incubated aerobically overnight at 37°C. Organisms were identified as commensal or pathogen as per protocol. Tracheal aspirates showing less than 10 5 cfu/ml and bronchial secretions with less than 10 4 cfu/ml by semiquantitative culture were regarded as commensal or contaminant. Single or mixed growth (two or more than two isolates per specimen) isolated from all the eligible consecutive samples were identified by observing the colony characteristic on the blood, Mac-Conkey agar plate, and biochemical reactions using standard microbiological methods. [8] Isolates from repeat culture of previously recruited patients and isolates identified as commensal or contaminants were excluded. The study was conducted in two phases: phase I (2004-6) and phase II (2006-9). During phase I, activity of ampicillin, cefuroxime, gentamicin, ciprofloxacin, cefotaxime, amikacin, and ceftizoxime was tested. During phase II, activity of ceftriaxone, ceftazidime, ceftizoxime, amoxy-clav, gentamicin, amikacin, ciprofloxacin, meropenem, piperacillin, piperacillin tazobactom, aztreonam, netilmycin, and ofloxacin was tested. Susceptibility testing was done by disc diffusion method. [9] The following antibiotics (Hi-Media Disc in μg) were tested: ampicillin (10), piperacillin (100), ceftazidime (Cz) (30), ceftizoxime (Ck) (30), cefuroxime (30), cefotaxime (30), ceftriaxone (30), amoxycillin/clavulanic acid (Ac) (20/10), piperacillin/tazobactum (TZP) (100/10), aztreonam (Ao) (30) , meropenem (Mr) (10), gentamicin (10), amikacin (Ak) (30), ciprofloxacin (Cf) (5), ofloxacin (Of) (5), and imipenem(I) (10). Zone diameter was measured and interpreted as per the Clinical and Laboratory Standards Institute guidelines. For quality control of disc diffusion tests, ATCC control strains of E. coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 strains were used. Results During the study period, laboratory data of 2776 patients whose LRTI specimens were received in our laboratory were evaluated. Male to female ratio was 1:1. About 21.61% of patients were in age group of less than 17 years, 42.15% in 18-64 years, and 36.38% were of more than 65 years of age. Out of 2776 specimens, 1125 (40.52%) were culture positive, whereas 1651 (59.47%) specimens showed no growth. Out of 2776 specimens, 1233 (44.41%) isolates were recovered. A total of 1017 samples showed single isolation, whereas from 108 samples, 2 isolates per specimen were recovered. Out of the total 1233 isolates identified, 1123 (91.07%) were gram-negative bacilli (GNB) and 110 (8.92%) were gram-positive organisms. Aerobic GNB remained the predominant cause of LRTI in ICU patients throughout the study period. [Table - 1] shows year-wise distribution of GNB isolated from the lower respiratory tract. During the 5-year span, P. aeruginosa remained the most common pathogen. Trends of antimicrobial resistance among the leading pathogens causing LRTI were studied in two phases, i.e., from 2004-2006 (phase I) and 2006-2009 (phase II). Pattern of antimicrobial resistance in phase I is shown in [Table - 2]. During the second phase, few new antimicrobials were added in the panel. Phase II showed a increasing trend in resistance to cephalosporins and declining trend in resistance to aminoglycosides against most GNB. Sensitivity to quinolones was relatively stable among GNB [Table - 3]. In 2006-2007, resistance to ceftriaxone and ceftazidime ranged from 66 to 97% and it increased to 80 to 97%in 2008-2009. But in contrast to other gram-negative isolates, Acinetobacter isolates were more resistant to ceftriaxone, ceftizoxime, and ceftazidime (85-97% in 2006-207), but it also increased to 95-97% in 2008-2009. As far as resistance to aminoglycosides is concerned, resistance to gentamicin was relatively high when compared with amikacin in all the 3 years of phase II. But resistance to both these drugs decreased continuously during phase II [G, 66-79% (2006-2007) to 51-57% (2008-2009)], [AK, 50-65% (2006-2007) to 48-53% (2008-2009)]. About 93% of Acinetobacter isolates showed resistance to gentamicin in 2006-2007 which reduced to 72.83% in 2008-2009. In contrast, Acinetobacter isolates showed increasing trend of resistance to amikacin (65.9-70.37%). Multidrug resistance (resistance to three or more than three drugs) was observed in 83% of total isolates during study period. Discussion In this study, GNB were the predominant organisms causing LRTI. During the study period of the 5 years, P. aeruginosa remained the most common organism (30-50%) followed by Klebsiella spp., but from 2005 to 2006 onward, the rate of isolation of Acinetobacter spp. increased from 11.78% (2004-2005) to 25% (2008-2009) becoming the second most common isolate. Lokhart et al[10] reported P. aeruginosa as the most common isolate from lower respiratory tract specimens in ICU, but Kumari et al[11] reported non-fermenting GNB other than P. aeruginosa as the most common pathogens. During phase I, high level of resistance was observed to ampicillin (97-98%), cefuroxime (90-93%), gentamicin (79-80%), and amikacin (70-71%) against all the GNB, so during phase II some new drugs such as ceftriaxone, ceftazidime, and amoxicillin-clavulanic acid were added to the panel for GNB other than P. aeruginosa. For P. aeruginosa, other additional drugs tested were ofloxacin, piperacillin, piperacillin/tazobactam, netilmycin, and aztreonam. We observed an alarming increasing trend of resistance to third-generation cephalosporins and amoxycillin/clavulanic acid during phase II (2006-2009). During 2006-2007, piperacillin and piperacillin/ tazobactam were found to be relatively effective against P. aeruginosa with susceptibility ranging from 52.95 to 55.89%, but susceptibility rapidly decreased to 20.99 and 23.46%, respectively, in 2008-2009. Another important observation of this study was increasing sensitivity trend of aminoglycosides against majority of GNB. During phase I, almost 70-80% of isolates were resistant to aminoglycosides, whereas during phase II about 50-60% isolates were resistant to aminoglycosides. Navneeth et al[4] and Jafari et al[7] also reported increased sensitivity to aminoglycosides against GNBs. Kumari et al reported in their study on analysis of resistance pattern of tracheal and bronchial GNB isolates from the lower respiratory tract specimens of the ICU-admitted patients, the highest mean resistance to cefazolin (98.8%) and ampicillin (97.6%) while the lowest mean resistance to amikacin (48.5%). In our study, there was increasing trend of resistance to cephalosporins and amoxycillin/clavulanic acid and declining trend of resistance to aminoglycosides might be due to the selective influence of extensive usage of cephalosporins and amoxycillin/clavulanic acid when compared with aminoglycosides. During the year 2006-2007, meropenem was found to be quite effective against all the GNB with sensitivity ranging from 75 to 90%. Shehabi et al[12] and Lokhart et al[10] also reported carbapenems as the most effective drug for patients in ICUs, but we observed constant decrease in sensitivity during 2007-2009. Carbapenems are frequently used as the last choice in treating serious infections caused by GNB, and there is diminishing number of new antimicrobial drugs in the pharmaceutical pipeline so the observation of this study is of great clinical concern. We conclude that gram-negative organisms are the predominant pathogens causing LRTI in ICU patients. The increasing trend of resistance in gram-negative organisms is very disturbing. Judicious use of older and newer antimicrobial agents is essential to prevent the emergence of multidrug-resistant bacteria in the ICU. The development of newer therapeutic alternatives to address the problem of MDR GNBs is needed. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11041t3.jpg] [cm11041t1.jpg] [cm11041t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}