 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
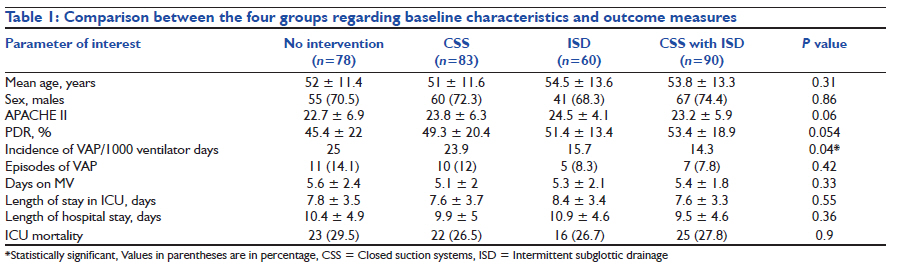
Indian Journal of Critical Care Medicine, Vol. 15, No. 3, July-September, 2011, pp. 168-172 Research Article Comparing influence of intermittent subglottic secretions drainage with/without closed suction systems on the incidence of ventilator associated pneumonia Deven Juneja, Yash Javeri, Omender Singh, Prashant Nasa, Rameshwar Pandey, Bhupesh Uniyal Department of Critical Care Medicine, Max Super Speciality Hospital, New Delhi, India Code Number: cm11042 DOI: 10.4103/0972-5229.84902 Abstract Context: Intermittent subglottic drainage (ISD) of secretions is recommended for prevention of ventilator-associated pneumonia (VAP) as it reduces microaspiration from the area around the cuff. Poor suction techniques can contribute to VAP, hence closed suction system (CSS) may have theoretical benefit in VAP prevention. Combination of these two techniques may provide added advantage.Aims: To study the influence of ISD with/without CSS on the incidence of VAP. Materials and Methods: Data from 311 patients requiring mechanical ventilation (MV) for more than 72 hours were collected retrospectively. They were divided into four groups as follows: group A, no intervention; group B, only CSS; group C, only ISD; and group D, ISD with CSS. These groups were compared with respect to incidence of VAP, duration of MV, length of ICU and hospital stay and ICU mortality. Results: Patients in the four groups were comparable with respect to age, sex ratio and admission Acute Physiology and Chronic Health Evaluation (APACHE) II scores. Incidence of VAP per 1000 ventilator days in groups A, B, C, and D were 25, 23.9, 15.7 and 14.3, respectively (P=0.04). There was no significant difference in the duration of MV (P=0.33), length of ICU (P=0.55) and hospital stay (P=0.36) and ICU mortality (P=0.9) among the four groups. Conclusions: ISD of secretions reduces the incidence of VAP. CSS alone or in combination with ISD has no significant effect on VAP incidence. Hence, ISD may be recommended for VAP prevention, but indications other than VAP prevention should determine the type of the suction system. Keywords: Closed suction system, intermittent subglottic drainage, ventilator-associated pneumonia Introduction Ventilator-associated pneumonia (VAP) is the most frequently acquired infection by patients admitted in intensive care units (ICUs). [1] It is also associated with increased morbidity which in turn leads to increased ICU and hospital stay and hence higher medical expenses. [2] The risk of nosocomial pneumonia increases by 6 to 20-fold in intubated patients. VAP affects between 20 and 70% of the ventilated patients and accounts for at least 10 episodes per 1,000 intubation days. [1] Patients developing VAP have high mortality rate ranging from 33 to 70% [2],[3],[4],[5],[6] and patients developing VAP are twice more likely to die than those without VAP. [7] Therefore, prevention of VAP has been regarded as the topmost priority in ICU infection control programs. [8] Among the various measures to prevent VAP, some like semi-recumbent position, subglottic secretion drainage, proper hand washing by staff, etc. have been proven to be beneficial and are generally recommended.- [9] Other measures like use of closed suction systems (CSSs ) have been advocated but are not currently recommended due to lack of conclusive evidence. [9] Aspiration of oropharyngeal pathogens, or leakage of secretions containing bacteria around the endotracheal (ET) tube cuff, have been identified as the primary routes of contamination of the lower respiratory tract. [10],[11],[12],[13] In ventilated patients, failure of proper suction and low cuff pressure can easily lead to aspiration, which may in turn cause VAP. [14] Aspiration of subglottic secretions can prevent bacterial contamination of the lower respiratory tract and can prevent VAP. [12],[15],[16] In addition, poor suction techniques can lead to exogenous contamination of the respiratory tract which in turn can again lead to VAP. Use of CSSs can prevent this exogenous contamination and hence can have a role in VAP prevention. [17] Though combined use of a set of evidence-based practices, called the "ventilator bundle", has been proposed [18] to prevent the occurrence of VAP, the combination of intermittent subglottic drainage (ISD) of secretions with CSS, with the other measures to prevent VAP remaining the same, has not been studied. Hence, we aimed to study the influence of ISD with/without CSS on the incidence of VAP. Materials and Method This was a retrospective study conducted in an eight-bed medical ICU of a tertiary care hospital. Our medical ICU is an advanced care unit with more than 650 admissions per year. It has a 24 hours on-site intensivist coverage, and a 1:1 nurse-to-patient ratio is maintained at all times. Data were collected from the records of 311 adult patients who were admitted during the 3-year period ranging from January 2006 to January 2009 and required mechanical ventilation (MV) for more than 72 hours. Patients were divided into four groups according to the type of suction and the type of ET tube they had, as follows: group A: no intervention; group B: only CSS; group C: only ISD; and group D: ISD with CSS. Patients in the no intervention group A had classical Portex® cuffed ET tube (Smiths Medical ASD, Keene, NH, USA) and the conventional open suction system was used. In group B, the patients had classical Portex® ET tube with closed suction apparatus Steri-Cath (SIMS Portex; Keene, NH). In group C, patients had open ET suction system along with the Hi-Lo® Evac ET tube (Hi-Lo Evac; Mallinckrodt; Athlone, Ireland) with subglottic secretion evacuation system through which intermittent suction was applied to drain the subglottic secretions. In group D, patients had both ET tube with subglottic secretion drainage system (Hi-Lo Evac) and closed suction apparatus (Steri-Cath). Other components of the VAP bundle remained the same in all the groups. These groups were compared with respect to incidence of VAP, duration of MV, length of ICU and hospital stay, and ICU mortality, with incidence of VAP being the primary outcome measure. VAP was diagnosed according to the clinical pulmonary infection score (CPIS), with a score equal to or more than 6 being as the diagnostic cut-off. [19] Severity of illness was measured by Acute Physiology and Chronic Health Evaluation (APACHE) II score, and the predicted death rate (PDR) was calculated according to the APACHE II reference equations. [20] Consistent level of nursing care was maintained throughout the 3 -year period and there were no major changes in the ICU team which managed these patients. Patients were managed with fixed VAP prevention protocols regarding head end elevation (30°- 45°), use of H-2 receptor blocking agents for stress ulcer prophylaxis, sterile suctioning techniques, proper hand hygiene, use of orotracheal tubes, use of heat-moisture exchange filters, use of naso-gastric Ryles tube, promotion of early enteral feeding, maintenance of adequate cuff pressure to prevent cuff leak, daily wake test and early weaning from MV. Utmost care was taken to prevent re-intubation and similar weaning protocols were followed during the study period. Selective gut or oral decontamination did not form a part of our VAP bundle, but chlorhexidine mouth wash was given regularly to all ventilated patients. Statistical analysis We used SPSS Version 16.0 for the statistical analysis. Means of continuous variables were compared using Student′s t-test and categorical variables were compared using chi-square test and Fishers Exact test, as appropriate. One-way analysis of variance (ANOVA) was applied to test the significance between and within the four groups. A P value of less than 0.05 was considered significant. Results A total of 378 patients required MV in the given time frame, but the data from a total of 311 (82.3%) patients, who fitted the inclusion criteria, were analyzed. Sixty-five patients were excluded as they required MV for less than 72 hours and two were excluded because of unavailability of complete data. There were 78 (25.1%), 83 (26.7%), 60 (19.3%) and 90 (28.9%) patients in groups A, B, C, and D respectively. Overall, the mean age of the patients was 52.7 ± 12.5 years (range 24-82 years); there were 223 male (71.7%) and 85 female (28.3%) patients and the mean APACHE II score was 24.1 ± 6. The patients in the four groups were comparable with respect to age, sex ratio and admission APACHE II scores [Table - 1]. The most common reason for intubation was severe sepsis in 131 (42.1%) patients, followed by respiratory failure in 95 (30.5%) patients, airway protection in 67 (21.5%) and cardiac arrest in 18 (5.8%) patients [Table - 2]. The incidence of VAP per 1000 ventilator days in groups A, B, C, and D were 25, 23.9, 15.7 and 14.3, respectively (P=0.04). There was no statistically significant difference in the duration of MV, length of ICU and hospital stay and ICU mortality among the four groups [Table - 1]. In the overall population, the incidence of VAP per 1000 ventilator days was 19.1, the total number of VAP episodes was 33 (10.6%) and overall ICU mortality was 27.7% (86 patients). Discussion Through this retrospective study, we could emphasize the fact that the use of intermittent subglottic secretion drainage is beneficial in preventing VAP. Closed suction drainage alone or in combination with ISD may not aid in preventing VAP and hence its use should not be encouraged for this purpose. Even though there was reduced incidence of VAP with use of ISD, it did not translate into any mortality benefit or reduced ventilator or ICU stay. We used the CPIS score to diagnose VAP as this is a validated tool for the diagnosis of VAP with a reported sensitivity and specificity of more than 90%. [19],[21],[22],[23] In addition, this being a retrospective study, it was easily available to us as we calculate CPIS score for all ventilated patients on a daily basis as a part of our VAP prevention protocol. Based on CPIS score, VAP occurred in 10.6% of the total population, ranging from 7.8% in patients having both ISD and CSS to 14.1% in patients without ISD and CSS, which is in accordance with the reported range of 9-27% in all intubated patients. [24],[25] In the National Nosocomial Infections Surveillance report, the median rate of VAP per 1000 ventilator days in various hospitals ranged from 2.2 to 14.7, [26] which is comparable to our overall VAP incidence of 19.1. Aspiration of the subglottic secretions is an effective measure to prevent VAP, with little risk involved. It has been shown to reduce the incidence of VAP by nearly half. In our cohort of patients too, addition of ISD to our existing VAP bundle significantly reduced the incidence of VAP from 25 to 15.7 episodes per 1000 ventilator days. It is especially proven to reduce the incidence of early-onset pneumonia (pneumonia occurring within 5-7 days after intubation). In addition, ISD has been shown to shorten the duration of MV and the length of stay in the intensive care unit. [27] Although in our study we could not demonstrate any significant reduction in mortality or reduction in days on MV or length of ICU stay, it could be due to our relatively small sample size. Nevertheless, there have been other reports too where ISD was not associated with reduced mortality or length of ICU stay despite being associated with decreased VAP rates. [28],[29] Even though ISD of secretions is well established and widely recommended as an essential measure to prevent VAP, it is still not widely applied in clinical practice. [30] Wider application of evidence-based practices should be advocated for better acceptance and application of this method for VAP prevention. CSS has several inherent advantages including no external handling by staff and hence it decreases airway contamination. [17] In addition, suctioning through CSS causes no loss of positive end-expiratory pressure (PEEP) and prevents de-recruitment which especially may be beneficial in patients with acute respiratory distress syndrome. [31],[32],[33] It may also have a lower risk of contamination of the ET system due to a protective sheath and a role in preventing exogenous spread of infection to other patients when it is used in patients infected with methicillin-resistant Staphylococcus aureus, or Mycobacterium tuberculosis. [34] It is also easy to use and saves nursing time. [33] Use of CSS causes fewer physiologic and hemodynamic disturbances compared to the conventional open suction systems. [33] Even though a few studies have suggested some benefits of CSS in VAP prevention, [17],[35],[36] a number of meta-analyses have shown that it has no beneficial effect on the VAP incidence, mortality and ICU length of stay [37],[38],[39],[40] and hence it is not currently recommended for VAP prevention. [9] In the present study too, there was only a marginal reduction in VAP incidence from 25 to 23.9 per 1000 ventilator days, when CSS was added to the existing VAP bundle. Even when CSS was used in combination with ISD, there was only a non-significant reduction in VAP incidence to 14.3 as compared to 15.7 per 1000 ventilator days when ISD was used alone. Limitations This was a single-center retrospective study and hence the results may lack wider generalization. In addition, the effect of circumstances (emergency or elective) and site of intubation (ICU or emergency) was not studied. But as the level of competency was maintained the same throughout the time period, we believe the effect of these factors to be minimal. The diagnosis of VAP was made according to the CPIS score, which itself has certain limitations. [41] Conclusions ISD of secretions reduces the incidence of VAP in patients receiving MV. CSS alone or in combination with ISD has no significant effect on the incidence of VAP. Hence, ISD may be recommended for VAP prevention, but indications other than VAP prevention should determine the type of the suction system in a mechanically ventilated patient. To show a mortality benefit, larger multicenter trials may be required. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11042t2.jpg] [cm11042t1.jpg] |
| |||||||||

{kind=link}
{kind=link}