 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
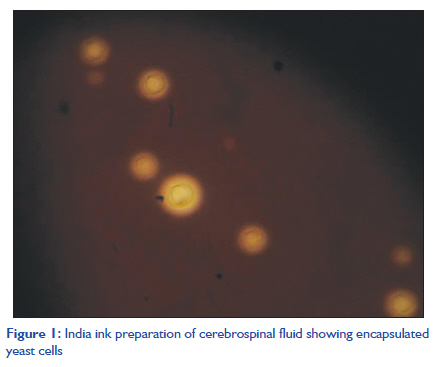
Indian Journal of Critical Care Medicine, Vol. 15, No. 3, July-September, 2011, pp. 176-178 Case Report Fulminant intracranial hypertension due to cryptococcal meningitis in a child with nephrotic syndrome Leena Nagotkar, Preeti Shanbag, Anupama Mauskar, Syed Ahmed Zaki, Chaya A Kumar Department of Pediatrics and Microbiology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India Code Number: cm11044 DOI: 10.4103/0972-5229.84905 Abstract Cryptococcus neoformans has a worldwide distribution. Meningoencephalitis is the most common manifestation of cryptococcosis. The outcome of a patient with cryptococcal infection depends on the immune status of the host. Patients with nephrotic syndrome are particularly susceptible to cryptococcal infection not only due to innate changes in their immune system but also because of the immunosuppressive agents used in the treatment. We report an 8-year-old boy with nephrotic syndrome, who developed cryptococcal meningitis and died of fulminant intracranial hypertension.Keywords: Cryptococcal meningitis, intracranial hypertension, nephrotic syndrome Introduction The fungus Cryptococcus neoformans can cause common opportunistic infections in immuno-compromised patients, with meningoencephalitis being the most common manifestation. Virulence of the organism plays a relatively small role in determining the outcome of an infection. The crucial factor is the immune status of the host, especially patients with defective cell-mediated immunity such as patients with the acquired immunodeficiency syndrome (AIDS), organ transplant recipients, patients with nephrotic syndrome and those on immunosuppressive regimens including corticosteroids. [1] We describe a fatal case of cryptococcal meningitis with fulminant intracranial hypertension in a child with nephrotic syndrome. Case Report An 8-year-old boy presented with a 4-day history of fever, facial puffiness and abdominal pain. The child had been diagnosed to have nephrotic syndrome 2 years earlier and was receiving low-dose steroids (0.5 mg/kg of prednisolone on alternate days) for a frequently relapsing course. On examination, the child was febrile and had generalized edema. The pulse was 90/minute; the respiratory rate was 36/minute and the blood pressure was 100/60 mm of Hg. The abdomen was distended with a fluid thrill and mild tenderness in the hypogastrium. Peristaltic sounds were normally heard. Respiratory system examination revealed dullness on percussion and diminished breath sounds in the left infra-axillary region. Central nervous system (CNS) examination revealed a conscious alert child with no signs of meningeal irritation or focal neurological deficit. Cardiovascular system examination was normal. Investigations showed hemoglobin of 12.5 g/dL, a total WBC count of 16,800/mm 3 , and a differential count of polymorphs 78% and lymphocytes 22%. Urine examination showed 4 WBCs/mm 3 with albumin 4+. The serum sodium was 126 mmol/L, serum potassium was 5.6 mmol/L, the blood urea nitrogen was 9 mg/dL and serum creatinine was 0.7 mg/dL. Total serum protein was 3.9 g/dL with a serum albumin of 2.0 g/dL. Chest X-ray showed bilateral pleural effusion, more on the left side. An ascitic tap showed 36 cells, all lymphocytes. The child was started on intravenous cefotaxime and amikacin on a presumptive diagnosis of peritonitis, but ascitic fluid culture was subsequently sterile. Prednisolone was continued in a dose of 0.5 mg/kg daily. The child continued to have high-grade fever and was shifted to intravenous piperacillin on the fourth day since urine culture grew Escherichia coli >10 5 colonies sensitive to piperacillin. The child became afebrile 3 days later and edema decreased. After an afebrile period of a week, he complained of severe headache and vomiting. Physical examination at this stage revealed a heart rate of 78/minute and blood pressure of 108/80 mm of Hg. CNS examination revealed an irritable child with no neck stiffness or neurological deficit. Deep tendon reflexes were exaggerated bilaterally with extensor plantar reflexes. Fundus examination showed no papilledema. A computed tomography (CT) scan of the brain was normal. A lumbar puncture showed an opening pressure of 26 cm of water on manometry. Cerebrospinal fluid (CSF) examination showed 38 cells with 26 lymphocytes and 12 polymorphs, a protein of 60 mg/dL and glucose of 54 mg/dL, with a blood glucose level of 179 mg/dL. CSF bacterial culture was sterile. An India ink examination of CSF revealed capsulated, budding yeast cells measuring 5-20 μm, suggestive of C. neoformans. CSF fungal culture on Sabouraud′s dextrose agar grew mucoid, cream-colored colonies after 72 hours. The isolate was confirmed as C. neoformans [Figure - 1] by a positive urease test and brown-colored colonies on bird seed agar. The antibiotic sensitivity by disc diffusion method showed sensitivity to amphotericin B. Species identification showed C. neoformans var. neoformans. Urine and blood fungal cultures showed no growth. The patient was started on intravenous amphotericin B (0.7 mg/kg/day), oral flucytocin (100 mg/kg/day), mannitol and dexamethasone. Daily lumbar puncture was done for relief of raised intracranial tension, but headache and vomiting persisted. Four days later, the child developed generalized tonic-clonic seizures following which he started to gasp and became unresponsive. Systolic blood pressure dropped to 60 mmHg. He was intubated, stabilized and transferred to the intensive care unit for mechanical ventilation. Fundus examination at that stage showed early papilledema. A repeat CT scan brain showed mild dilatation of the ventricles. Neurosurgeons were consulted for insertion of a ventriculoperitoneal shunt, but continuation of conservative management was advised. However, the child continued to deteriorate over the next 12 hours and sustained a cardiac arrest from which he could not be resuscitated. Discussion Patients with nephrotic syndrome have defective cell-mediated immunity. Therapy with steroids and other immunosuppressive therapies contribute to their increased susceptibility to a variety of infections. [2] Qadir et al. described disseminated cryptococcosis in a patient with nephrotic syndrome, who was not on immunosuppressive therapy. [3] Our patient, however, had been on long-term low-dose steroids. C. neoformans is a ubiquitous organism, exposure to which is common. Infection with C. neoformans is acquired by inhalation of the organism from environmental sources. Pulmonary infection due to cryptococcosis is often asymptomatic though Nakayama et al. described pulmonary cryptococcosis in a case of necrotizing glomerulonephritis presenting with nephrotic syndrome. [4] If uncontained, there is hematogenous spread to other sites, in particular, the central nervous system. [5] Meningitis is the most frequent manifestation of cryptococcosis. Patients usually present with headache, fever, malaise and altered mental status. Signs are often absent, but may include meningism, papilledema, cranial nerve palsies and other focal neurological deficits, and depressed consciousness level. [1],[5] Cryptococcal meningitis is invariably fatal if untreated. In non-HIV-infected, non-transplant hosts with cryptococcal meningoencephalitis, amphotericin B (0.7-1.0 mg/kg/day IV) plus flucytosine (100 mg/kg/day orally in four divided doses) for at least 4 weeks (6 weeks in the presence of neurological complications) is recommended in the induction phase. Oral fluconazole is given at a dose of 12 mg/kg/day for 8 weeks during the consolidation phase, followed by 3 mg/kg/day for 6-12 months in the maintenance phase. [6] Significantly raised CSF opening pressure (>25 cm H2O) occurs in >50% of immunocompromised patients with cryptococcal meningitis. This may exist at presentation or develop during mycologically successful therapy. It is associated with worsening headache, altered mental status, visual and hearing loss, other symptoms and signs of raised intracranial pressure, and increased mortality. [7] A CT or magnetic resonance imaging (MRI) scan of the brain usually shows normal ventricular size. The causes of the raised opening pressure are poorly understood and the mechanism is hypothesized to be the obstruction of CSF outflow by a large burden of yeasts and polysaccharide plugging the arachnoid villi. [8] What causes such rapid evolution of Intracranial hypertension in cryptococcal meningitis, as occurred in our patient, is unknown, but the most critical determinant of outcome for cryptococcal meningoencephalitis is control of CSF pressure. Medical treatment using acetazolamide has not been shown to be effective. [9] In a retrospective analysis, steroids did not appear to be helpful. [6] Acute elevated symptomatic CSF pressure should be managed aggressively by decompression. Daily serial lumbar punctures with withdrawal of large volumes of CSF to achieve a closing pressure of ≤20 cm H 2 O or 50% of initial opening pressure have been recommended. This aggressive approach may be inadequate to control severely elevated opening pressures. Insertion of a temporary lumbar drain, which can safely remove over 200 ml CSF daily in a controlled fashion, may be a much more effective means of pressure control if expertise and facilities allow. Ventriculostomy may be tried in selected patients. Neurosurgical shunting is recommended for patients with classical obstructive hydrocephalus provided it is done after starting antifungal therapy. [6] In conclusion, a child with nephrotic syndrome represents an immunocompromised host and cryptococcal infection should be considered in the differential diagnosis of an indolent febrile illness in such a patient. Routine measurement of opening CSF pressures by manometry, and aggressive decompression may decrease morbidity and mortality in patients with cryptococcal meningitis. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11044f1.jpg] |
| |||||||||


{kind=link}