 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
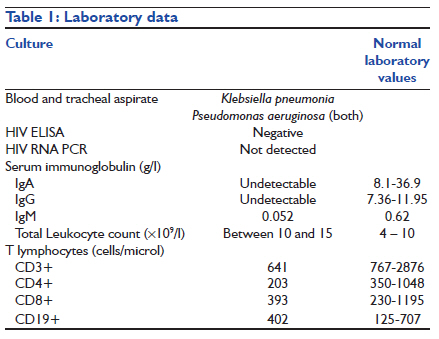
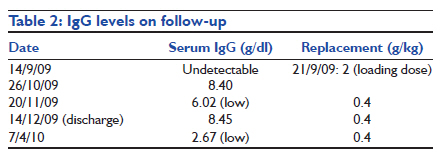
Indian Journal of Critical Care Medicine, Vol. 15, No. 3, July-September, 2011, pp. 179-181 Case Report Primary immune deficiency in the intensive care unit: It is never too late to diagnose and treat Rucha S Dagaonkar1, Tiyas Sen1, Zarir F Udwadia1, Mukesh B Desai2 1 Department of Pulmonary Medicine, P D Hinduja National Hospital and MRC, Mumbai, India Code Number: cm11045 DOI: 10.4103/0972-5229.84903 Abstract Common variable immunodeficiency disorders (CVIDs), a heterogeneous group of primary immune deficiencies, can present at all age. Our patient with a hitherto undiagnosed CVID, symptomatic since middle ages, presented with severe pneumonia. Specific management of his CVID in addition to standard therapy was life-saving.Keywords: Adult primary immune deficiency, common variable immune deficiency, intravenous immunoglobulin, late onset common immunodeficiency, non-resolving pneumonia Introduction Common variable immunodeficiency disorders (CVIDs) are a heterogenous group of immune deficiencies characterized by hypogammaglobulinemia. The diagnostic criteria are: History of recurrent infections, decreased IgG levels (less than two standard deviations below the lowest normal level), one more immunoglobulin deficiency, and failure to mount sufficient antibody response to antigen challenge (with pneumococcal or HiB vaccines). [1],[2] Pulmonary complications are common. [3] We report a case of severe pneumonia eventually diagnosed to have a CVID. Case Report A 42-year-old man presented to our center with high-grade fever, chills, productive cough since six weeks, weight loss (6 kg over four weeks), and diarrhea since two weeks. In mid-July, a chest radiograph (CXR) showed right middle zone consolidation. Sputum culture grew Klebsiella pneumoniae. Antibiotics were started (levofloxacin, amikacin, metronidazole, fluconazole) without response, at another center. Empiric anti-tuberculosis therapy (ATT) was started. When there was no response, he was referred to our hospital (13/9/09). He was asymptomatic until 5 years ago after which he had recurrent upper respiratory tract infections (RTIs) since 2005: pneumonia (2006), and was treated for pulmonary tuberculosis twice (2005, 2007). Since 2007, he had monthly episodes of watery diarrhea. Childhood and family history were insignificant. Examination revealed fever, tachycardia, tachypnea (respiratory rate 36/min), blood pressure of 110/60, and bilateral crepitations on chest auscultation. PaO2 was 58 mm Hg on arterial blood gas analysis. He was admitted to the intensive care unit (ICU) where CXR showed right middle and lower zone consolidation. Non-resolving pneumonia (NRP) was diagnosed and meropenem and levofloxacin were started, ATT being discontinued. Endotracheal intubation was soon required. By day 5 in ICU, CXR showed bilateral alveolar shadows with PaO2 /FiO2 of 59/1 (<200). Ventilation with ARDS protocol was started. Noradrenaline was given at ceiling doses. Antibiotics were changed (targocid, colistin) as per sensitivity reports, and empiric amphotericin-B was added. Trimethoprim-cotrimoxazole prophylaxis was started. Underlying primary immune deficiency (PID), a CVID, was suspected. Intravenous immunoglobulin (IVIG) was given (2 g/kg on 21/9/09), over five days for the hypogammaglobulinemia [Table - 1]. By day 2 of IVIG administration, the patient became afebrile for the first time in eight weeks. FiO2 requirements reduced (35% by 6/10/09). Tracheostomy was done (30/10/09), with subsequent decannulation (26/10/09). CXR showed clearing of alveolar shadows, with residual bronchiectasis. He was ambulatory on discharge (December) and follows up (irregularly, due to cost constraints) for replacement IVIG and chest physiotherapy. Discussion Our initial diagnosis was an NRP with Gram-negative sepsis. Serum immunoglobulin level measurement done as a part of the workup for NRP [Table - 1] showed hypogammaglobulinemia. Low CD4 T lymphocyte counts suggested T lymphocyte dysfunction. HIV infection was ruled out. There was also history of recurrent RTIs and diarrhea, beginning 5 years prior to presentation. There was infection with two organisms (Klebsiella pneumonia and Pseudomonas aeruginosa) at presentation. These points suggested an underlying adult-onset PID with antibody deficiency, [4] and possibly, T lymphocyte dysfunction. [5] High-dose IVIG was commenced (2 g/kg loading dose, over 5 days), as serum IgG levels were undetectable, [6] and significant improvement followed, within 72 hours. Although theoretically this could be attributed to the effect of IVIG on systemic inflammatory response in sepsis, [6],[7] repeat IgG levels, after 8 and 12 weeks of loading dose, continued to decline [Table - 2], improving only after replacement doses (0.4 g/kg) were given, thus confirming the diagnosis of a CVID. [1] Recurrent RTIs are the most common manifestation in CVIDs, [3],[4],[8] complicated with sequelae like chronic sinusitis, lung fibrosis, and bronchiectasis (12.2%). [6] Granulomatous Interstitial Lung Disease can shorten survival in CVIDs. [9] Other manifestations include autoimmune phenomena and systemic lymphocytic infiltration. Antibody deficiency [10] predisposes to infections with encapsulated bacteria. This is preventable with regular IVIG replacement. [2] Treatment of hypogammaglobulinemia is replacement with a monthly dose of 0.4 g/kg, even on outpatient basis. [2],[11],[12] Maintenance of serum IgG trough level >0.8 g/l, in patients with pulmonary complications is recommended.- [6] Antibody failure precludes the use of vaccines. [2] It is a common misconception that PIDs are mainly a pediatric problem. CVIDs can present at any age, with onset peaking in the first and third decades. [3] Our patient became symptomatic in the fourth decade (age 37 years), and was diagnosed in the fifth decade (age 42 years). He also had low CD4 lymphocyte counts. He could therefore fall into the late-onset common immune deficiency category, as per the DEFI study. [5] NRPs occur even in immunocompetent patients, frequently causing sepsis. ICU mortality of severe pneumonias was 36.8% in one series. [8] PIDs may easily be missed as a cause of NRPs, as other causes (malnutrition, HIV infection, tuberculosis, inappropriate use of antibiotics) are common, while the exact incidence of CVIDs is unknown, although it is the most common PID encountered in clinical practice. [2],[4],[11] The pneumonia in our patient deteriorated despite appropriate antibiotics, mechanical ventilation, and inotropes, improving only when his underlying PID was diagnosed and treated. The learning point that emerges is, CVIDs are an important cause of severe pneumonia even in adults. Correct diagnosis and prompt treatment of the underlying CVIDs, even in patients on maximum life support, can reduce the mortality of severe pneumonia. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11045t2.jpg] [cm11045t1.jpg] |
| |||||||||

{kind=link}
{kind=link}