 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
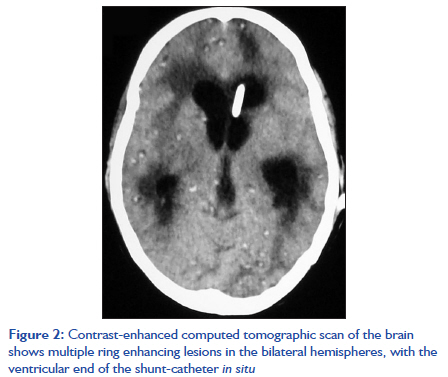
Indian Journal of Critical Care Medicine, Vol. 15, No. 3, July-September, 2011, pp. 185-187 Case Report Neurocysticercosis: Acute presentation and intensive care management of two cases Aanchal Sharma1, Charu Mahajan1, Girija P Rath1, Sarita Mohapatra2, Uma P Padhy3, Lokesh Kumar4 1 Department of Neuroanesthesiology, MKCG Medical College, Berhampur, Orissa, India Code Number: cm11047 DOI: 10.4103/0972-5229.84899 Abstract Neurocysticercosis (NCC), a common helminthic infestation in developing countries, may cause acquired epilepsy and neurological morbidities. Acute symptomatic seizure is the most common manifestation. The other clinical conditions include headache, hydrocephalus, chronic meningitis, focal neurological deficits, and psychological disorders. Altered sensorium and raised intracranial pressure (ICP) may require ventilatory support in an intensive care unit (ICU). Definitive diagnosis is made by identification of parasites in tissues or by a radiological demonstration of the scolex in cystic lesions. Antiepileptic drugs are used to control seizures after NCC. Steroids are generally administered along with antihelminthics, in order to control the edema and intracranial hypertension that may occur as a result of antiparasitic medications. In patients with intracranial hypertension, the priority is to manage the ICP before considering other treatment options. Antiparasitic drug treatment is never the mainstay of treatment, especially in the setting of elevated ICP. Here, we present the ICU management of two such cases.Keywords: Cerebral edema, intensive care management, intracranial pressure, neurocysticercosis, seizures Introduction Neurocysticercosis (NCC) is one of the most common helminthic infestations affecting the central nervous system (CNS). It is caused by the larval stage of the tapeworm Taenia solium. [1] The clinical manifestations of the disease may vary with the size and location of cysticerci and the intensity of the host′s immune response. Acute symptomatic seizures are the most common manifestations. The other clinical conditions include headache, hydrocephalus, chronic meningitis, focal neurological deficits, and psychological disorders. [2] Altered sensorium and raised intracranial pressure (ICP) may require ventilatory support in an intensive care unit (ICU). Here, we present the intensive care management of two such cases. Case Reports Case 1 A 41-year-old male, presented with history of fever, headache, and episodic seizures for one month. The neurological examination and routine investigations were normal, except for eosinophilia. A computed tomographic (CT) scan of the head showed numerous tiny hypodense foci scattered throughout the brain parenchyma. Cerebrospinal fluid serology was negative for antigens of herpes simplex, tubercular, and Japanese Encephalitis. Electroencephalography showed generalized slowing of the waves. The patient was managed with broad spectrum antibiotics and supportive treatments, but without any improvement. One week later magnetic resonance image (MRI), revealed numerous tiny lesions scattered throughout the brain parenchyma, with relative predilection for a gray-white junction and basal ganglia. The lesions were hyperintense on a T2-weighted image, without associated parenchymal edema. On contrast administration, none of these lesions showed enhancement. There was no intraventricular cyst or hydrocephalus [Figure - 1]. Similar lesions were also noted on the scalp, tongue, extraocular muscles, muscles of the face, neck, trunk, and limbs. The diagnosis of cysticercosis was confirmed after a skin and muscle biopsy was taken, which showed cysticercus surrounded by an intense inflammatory infiltrate. The patient was treated with pyrantal pamoate, mannitol, steroids, and sodium valproate. However, the sensorium deteriorated with a Glasgow coma score (GCS) of E2V1M4 . The trachea was intubated for ventilatory support, in the ICU. Two days later, the motor response deteriorated further (M2). Repeat MRI of the brain done two weeks later showed similar findings without any parenchymal edema. In view of the prolonged mechanical ventilation, percutaneous tracheostomy was done. He was gradually weaned off from the ventilator. In spite of continued supportive treatment, there was no neurological improvement. Oral albendazole was added to the treatment regimen. At present, after two months of treatment, the patient is on room air with a GCS of E4VTTM2 . Case 2 A 35-year-old male, non-vegetarian by diet, was diagnosed as having neurocysticercosis six months back, for which he received oral phenytoin 300 mg, daily. However, non-compliance with the treatment led to three episodes of generalized seizures and altered sensorium. In view of further neurological deterioration, the trachea was intubated and he was put on ventilatory support. Investigations including a hemogram and biochemistry were within normal limits. A contrast-enhanced CT scan of the brain showed multiple ring enhancing lesions of NCC in the bilateral hemispheres, with left ventricular hydrocephalus [Figure - 2]. External ventricular drainage (EVD) was done, but without much improvement in the sesorium. The patient underwent surgery the next day after admission, for endoscopic removal of the ventricular neurocysticerci followed by insertion of a ventriculoperitoneal shunt. The lungs were ventilated till the GCS improved to full score, following which the trachea was extubated. Postoperatively, the medical management included administration of phenytoin and steroids; cysticidal therapy was not given considering the presence of an intraventricular cyst. He was discharged after three weeks of hospital stay with advice for follow-up. Discussion Neurocysticercosis (cyst lodged in the CNS) is the most common form of human cysticercosis, with the brain parenchyma being the most common site. It is the main cause of acquired epilepsy and neurological morbidity in many of the developing countries. [1],[2] As per the estimation by the World Health Organization (WHO), over 50 000 deaths occur due to NCC each year, and many times an equal number of people have active epilepsy, with all the social and economic consequences that this implies. [3] Clinically, diagnosis is usually difficult due to varied presentations. MRI is considered the best neuroimaging tool for the detection of degenerating and innocuous (viable) cysticerci, while CT is better for calcified lesions. [2] The added advantage of MRI is that it can differentiate the stages of the parasite, which CT fails to do. Tissue biopsy showing cysticercus larvae remains the most accurate means of diagnosis. Several serological tests have been used to detect specific antibodies. Enzyme-linked immunoelctrotransfer blot (EITB) with 100% sensitivity and an overall 98% specificity is used, currently, in most of the centers. [2] Chadha et al.[4] described disseminated cysticercosis in a 21-year-old male, who recovered following treatment. Cases of human cysticercosis with such extensive dissemination, involving all possible sites, namely, the brain, spinal cord, eyes, muscles, and subcutaneous tissues simultaneously, are indeed very rare. We report case with extensive involvement of brain parenchyma, muscles of thorax, abdomen, and thigh (Case 1). In this case, sudden neurological deterioration required tracheal intubation and mechanical ventilation. Although the patient received antihelminthic, antiepileptic, and steroid medications, there was no significant neurological improvement. After tracheostomy the patient was gradually weaned off the ventilator and was able to maintain a normal saturation of arterial oxygenation, on room air. Llompart Pou et al. reported a case, who came to the Emergency Department with complaints of severe headache for six hours. [5] The patient became unconscious after a cardiorespiratory arrest during one hour of observation. Intraventricular NCC was implicated for the cause of death. The cyst possibly caused obstruction to the flow of CSF by migration through the aqueduct of Sylvius. Altered sensorium was due to a resultant increase in ICP and associated cerebral edema. These patients might require immediate control of the airway with ventilatory support. During a two-to-five day antiparasitic therapy, exacerbation of neurological symptoms occurred, which was attributable to local inflammation, following the death of the larvae.[6] For this reason, both albendazole and praziquantel were generally given along with steroids for the control of cerebral edema that may occur after antiparasitic therapy. Seizure is the most common symptom occurring in 70 - 90% of the patients with NCC. It was the sole clinical presentation, in our second patient. Seizures secondary to NCC usually responded well to first-line antiepileptic drugs. However, non-compliance to treatment in our patient led to repeated episodes of seizures, with altered sensorium. In patients with intracranial hypertension secondary to NCC, the priority is to manage the ICP before considering other treatment options. [6] Antiparasitic drug treatment is never the primary treatment modality, especially in the setting of elevated ICP. For intraventricular cysts, endoscopic surgery is the procedure of choice. Hydrocephalus is managed with a ventriculoperitoneal shunt, but these shunts suffer frequent blockade by small cysts or inflammatory exudates, and require multiple revisions. [7] NCC is a preventable disease; however, control of intracranial hypertension or epileptic syndromes are the mainstay of management during acute presentations. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11047f1.jpg] [cm11047f2.jpg] |
| |||||||||

{kind=link}
{kind=link}