 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
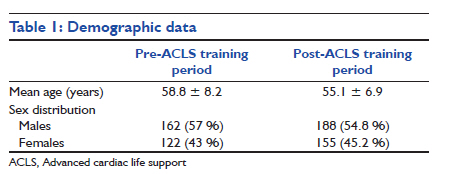
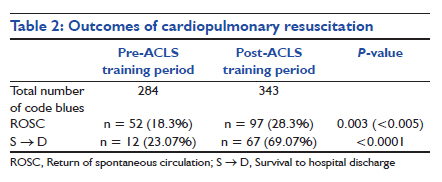
Indian Journal of Critical Care Medicine, Vol. 15, No. 4, October-December, 2011, pp. 209-212 Research Article Impact of advanced cardiac life support training program on the outcome of cardiopulmonary resuscitation in a tertiary care hospital Kanwalpreet Sodhi1, Manender Kumar Singla2, Anupam Shrivastava3 1 Department of Critical Care, S. P. S. Apollo Hospitals, Ludhiana, India Code Number: cm11059 DOI: 10.4103/0972-5229.92070 Abstract Background: Guidelines on performing cardiopulmonary resuscitation (CPR) have been published from time to time, and formal training programs are conducted based on these guidelines. Very few data are available in world literature highlighting the impact of these trainings on CPR outcome.Aim: The aim of our study was to evaluate the impact of the American Heart Association (AHA)-certified basic life support (BLS) and advanced cardiac life support (ACLS) provider course on the outcomes of CPR in our hospital. Materials and Methods : An AHA-certified BLS and ACLS provider training programme was conducted in our hospital in the first week of October 2009, in which all doctors in the code blue team and intensive care units were given training. The retrospective study was performed over an 18-month period. All in-hospital adult cardiac arrest victims in the pre-BLS/ACLS training period (January 2009 to September 2009) and the post-BLS/ACLS training period (October 2009 to June 2010) were included in the study. We compared the outcomes of CPR between these two study periods. Results: There were a total of 627 in-hospital cardiac arrests, 284 during the pre-BLS/ACLS training period and 343 during the post-BLS/ACLS training period. In the pre-BLS/ACLS training period, 52 patients (18.3%) had return of spontaneous circulation, compared with 97 patients (28.3%) in the post-BLS/ACLS training period (P < 0.005). Survival to hospital discharge was also significantly higher in the post-BLS/ACLS training period (67 patients, 69.1%) than in the pre-BLS/ACLS training period (12 patients, 23.1%) (P < 0.0001). Conclusion : Formal certified BLS and ACLS training of healthcare professionals leads to definitive improvement in the outcome of CPR. Keywords: Cardiopulmonary resuscitation, basic life support, advanced cardiac life support Introduction During the recent years, cardiopulmonary resuscitation (CPR) has received much attention. Various internationally and nationally accepted guidelines for CPR have been published, and formal training programs based on these guidelines are being conducted by certified training centers. [1] The aim of these training courses is to impart both cognitive knowledge and psychomotor skills of CPR and to provide a standardised care to cardiac arrest victims in accordance with the specific guidelines. [2] A lot of literature is available on survival after CPR in different clinical settings, but very few studies have been conducted to assess the effectiveness of formal resuscitation training programs on the outcome of CPR. We designed a retrospective study to evaluate the impact of an American Heart Association (AHA)-certified basic life support (BLS) and advanced cardiac life support (ACLS) training course on the outcome of CPR in our hospital. Materials and Methods Clinical setting Our hospital is a 250-bedded tertiary care hospital in India. All healthcare professionals are provided in-hospital BLS training. They initiate CPR whenever there is a cardiac arrest in the hospital and continue till the arrival of the code blue team. The hospital has a designated code blue team that responds to all in-hospital cardiac arrest alarms, announced through the public announcement system. The code blue team consists of an anesthesiology registrar, a medicine registrar, on-duty resident medical officer, attending staff nurse and nursing supervisor of the shift. The hospital policy is to always initiate CPR in a cardiac arrest victim. Do not resuscitate (DNR) policy is not legal in India. A code blue running sheet is filled by a record keeper during the course of CPR. Intervention Before the intervention, the code blue team followed AHA guidelines for CPR, but no formal training had been conducted. With the aim of improving CPR skills, an AHA-certified 3-day BLS and ACLS provider course was conducted in our hospital in the first week of October 2009. The course included lectures and hands-on training of periarrest case scenarios, which were followed by a written test and skill assessments. All the anesthesiologists and doctors working in the emergency and intensive care units participated in the course and got certified. Study design After getting approval from the hospital ethics committee, we designed a retrospective study to evaluate the effectiveness of the above intervention on the outcome of CPR in in-hospital cardiac arrest victims. Cardiac arrest was defined by the absence of a detectable pulse (pulselessness), by patient′s unresponsiveness or by any arrest rhythm noticed on the monitor. [3] We identified all cases of in-hospital cardiac arrest in adults (>14 years of age) that occurred over an 18 months period between January 2009 to June 2010. Data regarding each cardiac arrest were collected from the code blue running sheets. We compared the code blue data from January 2009 to September 2009, i.e. pre-ACLS training period, with post-ACLS training period from October 2009 to June 2010. The patients on whom CPR was started outside the hospital or on arrival in the emergency ward were not included in the study. When a patient suffered several cardiac arrests in the hospital, only the first episode was included in the analysis for avoiding falsely elevated rate of successful CPR, or falsely diminished rate of survival to hospital discharge. Data entry consisted of patient demographic data and the outcomes of CPR. The outcomes of interest were immediate survival after CPR and survival to hospital discharge. Immediate survival was defined as the return of spontaneous circulation (ROSC) for more than 20 min. Statistical analysis The relevant data was entered in the excel sheet and was analysed using Epi Info software. Chi square test was used to compare the immediate survival rates (ROSC) and survival to hospital discharge rates in the pre-BLS/ACLS training period and post-BLS/ACLS training period. For all statistical analysis, P <0.05 was considered to be significant. Results A total of 627 adult patients suffering in-hospital cardiac arrest for the first time over the study period were included in the study. CPR was attempted in 284 patients during the pre-BLS/ACLS training period and in 343 patients in the post-BLS/ACLS training period. Demographic data is as shown in [Table - 1]. There was no significant association between either the age or sex with the outcomes in the study. Of the 284 cardiac arrest victims during the pre-BLS/ACLS training period, 52 patients (18.3%) had ROSC, while during the post-BLS/ACLS training period, 97 patients (28.3%) of 343 patients had ROSC. On statistical analysis, this was considered to be a significant difference in the immediate survival rate (P = 0.003) [Table - 2]. Of the 52 patients who survived during the pre-BLS/ACLS training period, only 12 patients (23.1%) were discharged from the hospital. During the post-BLS/ACLS training period, 67 patients (69.1%) were discharged of the 97 cardiac arrest victims who had ROSC. The survival to hospital discharge rate in the post-BLS/ACLS training period was statistically significant (P < 0.0001) when compared with the pre-BLS/ACLS training period [Table - 2]. Discussion In-hospital cardiac arrest is an emergency situation that requires teamwork and the appropriate sequential actions to rescue the patients. [4] The outcome of cardiac arrest and CPR is dependent on critical interventions, particularly early defibrillation, effective chest compressions and assisted ventilation. [5] Over the last 50 years, after the introduction of modern CPR, there have been major developments and changes in the performance of resuscitation. [6] But, despite considerable efforts to improve the treatment of cardiac arrest, most reported survival outcome figures are poor. [5] Even in the hospitalised patients, the rate of successful CPR has been reported by some studies to be as low as 2-6%, although most studies report successful CPR outcome in the range of 13-59%. [6],[7] The lack of resuscitation skills of nurses and doctors in basic and advanced life support has been identified as a contributing factor to poor outcome in cardiac arrest victims. [8] In an effort to improve cardiac arrest outcomes, recent investigations have focussed on the timing and quality of CPR. Several guidelines on performing CPR have been published and certified training courses based on these guidelines have become a standard in medical professionals′ training in many parts of the world. [1] The aim of these courses is to provide information and hands-on practice in the management of periarrest situations in accordance with the latest guidelines. Although life support courses are widely advocated, their effectiveness has been little studied. Very few studies are available in the literature on comparative CPR outcomes after formal resuscitation training. An in-hospital investigation demonstrated that cardiac arrest detected by an ACLS-trained nurse was strongly associated with a four-fold increase in survival to discharge (38% vs. 10%) than those detected by a nurse without ACLS training. [9] This indicates that ACLS-trained nurses provided an independent contribution to increased survival rate. The results of the present study show that the rate of immediate survival was 18.3% during the pre-BLS/ACLS period, which increased to 28.3% during the post-BLS/ACLS period. The rates of ROSC during both the study periods were not much different from those of previous studies of in-hospital cardiac arrests. [3],[4],[6],[10],[11] But, our study clearly shows an improved rate of immediate survival after the formal BLS/ACLS training (P < 0.005). A Brazilian study by Moretti et al. also shows a significant increase in ROSC from 27.1% to 43.4% even on inclusion of a single ACLS-trained personnel in the resuscitation team. [12] Another study by Sanders′ also reported improved resuscitation success in a rural community hospital after an ACLS provider course. [13] A study by Borimnejad et al. also showed that initial survival after CPR improved significantly with the CPR-trained emergency team (18.4-30%). [6] Although a previous study by Olasveengen reported a weak trend with survival to discharge rates improving only from 11% to 13% after implementation of the modified 2005 CPR guidelines, the study by Moretti et al. reported a statistically significant increase in survival to discharge in patients resuscitated by the CPR team having an ACLS-trained personnel versus the team having no ACLS personnel (20.6% vs. 31.7%). [6],[14] Our study also reports markedly improved survival to hospital discharge rates (23.1% vs. 69.1%) after formal BLS/ACLS training (P < 0.0001). The survival to discharge rates during the pre-BLS/ACLS period of our study are almost comparable to that reported in the literature (11.7-32.2%), but the significant increase in survival to discharge rates after the BLS/ACLS training to 69% highlights that formal training of code blue team members enormously improved the skills of CPR and their level of competence in resuscitation. [1],[3],[12],[15],[16],[17] This also shows that the quality of CPR performed might be better after ACLS training. This highlights the importance of certified hands-on training program on the outcome of resuscitation. Limitations of the study A few limitations of our study should be acknowledged. First, because this study was conducted at a single institution, external validity is relative and uncertain. Thus, other multicenter studies are required to ascertain the validity. Second, our results might be biased because of increased attention on resuscitation during the post-training period. Conclusions Successful resuscitation after cardiac arrest requires early recognition of cardiac arrest, rapid activation of trained responders, timely initiation of BLS, early defibrillation and early ACLS. [18] In accordance with a few data available in the literature, our study reveals that formal training of the CPR team drastically improves the survival rates and survival to hospital discharge rates following resuscitation of cardiac arrest victims. We conclude that formal certified BLS and ACLS training courses with hands-on practice and their periodic renewal are crucial in improving the outcomes of CPR. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11059t2.jpg] [cm11059t1.jpg] |
| |||||||||

{kind=link}
{kind=link}