 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
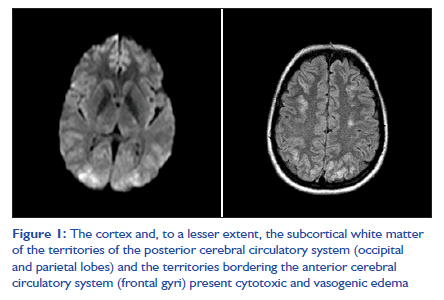
Indian Journal of Critical Care Medicine, Vol. 15, No. 4, October-December, 2011, pp. 227-229 Case Report Postpartum amaurosis in a woman with severe preeclampsia Mónica Mourelo1, Miguel Álvarez2, José L Díaz3, Teresa García4, Rita Galeiras1, David Freire1 1 Department of Intensive Medicine, Complejo Hospitalario Universitario A Coruña, A Coruña, Spain Code Number: cm11062 DOI: 10.4103/0972-5229.92077 Abstract The maternal and perinatal fetal prognosis of preeclampsia depends on the gestational age of the fetus at onset, the severity of the disease, the quality of care, and the presence of pre-existent medical conditions. One of the uncommon effects of severe preeclampsia on the eye is sudden loss of vision. The present case report is of a woman with severe preeclampsia exacerbated by delivery that coursed with difficult-to-control arterial hypertension and reversible cortical amaurosis without impaired consciousness or seizures. Keywords: Blindness, hypertension, posterior reversible encephalopathy syndrome Introduction Preeclampsia is a multisystem pathology. The incidence of preeclampsia is 5-7%, making it the foremost cause of maternal and fetal morbidity and mortality in industrialized countries. [1],[2] The pathogenesis of preeclampsia is complex, involving the interaction of genetic, immunologic, and environmental factors. Preeclampsia manifests with a heterogeneous clinical picture. [1] Case Report The patient was a 28-year-old woman with polycystic kidney disease and known arterial hypertension since her first pregnancy 5 years earlier, for which she was taking methyldopa. She was seen for hematuria in the obstetrics department in week 31 of pregnancy. Arterial hypertension (170/120 mmHg) detected in the physical examination motivated her hospitalization. The hematuria resolved in 24-48 hours, but high blood pressure (150/90 mmHg) persisted despite initial treatment with hydralazine. Proteinuria (0.93 g/24 h) and impaired renal function (creatinine 1.3 mg/dl) were present, but no evidence of hemolysis, elevation of transaminases or uric acid, or thrombocytopenia was found. In view of the patient′s preeclampsia and a nonreactive fetal pattern, the infant was delivered by cesarean section on day 7 of hospitalization. The patient, who intended to breast-feed, was assessed by the nephrology department for high blood pressure postpartum. She was started on nifedipine, but labetalol was later added due to poor control. On postpartum day 4, the patient presented a headache, vision loss that progressed to bilateral amaurosis, and bilateral nonreactive mydriasis. The retina and optic disc of both eyes were normal on ophthalmologic examination. Unenhanced cerebral computed axial tomography (CAT) showed no abnormalities. Cerebral nuclear resonance imaging (MRI) with a diffusion sequence revealed cytotoxic/vasogenic edema of the cortex and subcortical white matter [Figure - 1], which is consistent with posterior reversible encephalopathy syndrome (PRES). The patient was admitted to the intensive care unit and treated with antihipertensive agents with infusion of labetalol, nitroprussiate and valsartan, to which an alpha-adrenergic blocker, amlodipine, and hydrochlorothiazide were added. The patient recovered her sight 48 hours after admission to the ICU. The ocular examination disclosed symmetrical pupils that reacted slowly to light. Extraocular muscle function was unimpaired. The cornea was transparent and the anterior pole was normal. Examination of the ocular fundus revealed optic discs with clean, symmetrical margins and good coloring. The posterior pole was normal. Foveal reflex was normal. The patient did not present seizure or changes in consciousness. Intensive treatment for 2 weeks was required to control the blood pressure. Discussion Proteinuria and hypertension dominate the clinical manifestations of preeclampsia because the kidney is the target organ of the disease. [2] Even when full eclampsia does not develop, preeclampsia may lead to kidney failure, liver damage, intracranial hemorrhage, delayed fetal intrauterine growth, and fetal death. Despite the criteria for definition, many patients present without these clinical manifestations. There are no known biomarkers. The traditional criteria are not reliable in women with hypertension and proteinuria before week 20 of pregnancy, especially in women taking antihypertensive medication. The condition is more severe in women with chronic hypertension, pre-gestational diabetes mellitus, pre-existing thrombophilia, multiple pregnancy, or prior preeclampsia. [3] The criteria that define severe preeclampsia include blood pressure ≥160/110 mmHg, proteinuria ≥5 g/24 h, oliguria, lung edema, cerebral symptoms, epigastric pain, elevation of liver enzyme levels, microangiopathic hemolysis, thrombocytopenia, delayed fetal intrauterine growth, or oligohydramnios. [1] The three most common visual complications of severe preeclampsia are hypertensive retinopathy, exudative retinal detachment and cortical blindness. [4],[5] Cortical blindness refers to reduced vision from bilateral damage to any portion of the visual pathways posterior to the lateral geniculate nucleus. Eye examination is typically normal, including a normal pupillary light reflex. It occurs in up to 15% of preeclampsia and eclampsia. [4],[6] Currently, there are two competing theories for the cause of cerebral edema. One theory is that cerebral vasospasm induced by severe hypertension results in cerebral ischemia, and consequently, cytotoxic edema. The second theory is that acute hypertension induces a loss of autoregulation, causing passive dilatation of cerebral arterioles, as well as an increase in vascular permeability, and consequently, vasogenic edema. [6] To date, both vasogenic and cytotoxic edema have been observed in patients with cortical blindness. Management of preeclamptic patients who develop cortical blindness is the same as for women without this visual complication. [4],[6] The goal of treatment of a patient with preeclampsia is to minimize organ damage and prevent the development of eclampsia while maximizing fetal viability. [7],[8] The decision to induce delivery or proceed conservatively with the aim of improving the prognosis of the neonate which depends on stage of pregnancy, fetal status, and clinical situation of the mother. [1] Corticoids are safe and effective in reducing neonatal complications in women with severe preeclampsia before week 34 of pregnancy. Antihypertensive medication in women with preeclampsia and high blood pressure prevents cerebrovascular complications but does not change the course of the disease in women with mild preeclampsia. Hydralazine, labetalol, and nifedipine are the drugs most recommended for the control of acute severe hypertension in women with preeclampsia. [9] Magnesium sulfate prophylaxis may be useful before and after delivery in some women with severe preeclampsia; its benefits are not clear in women with mild preeclampsia. [9] Generally speaking, preeclampsia resolves with delivery. [1],[10] However, the condition exceptionally worsens in 48 hours after delivery. [1],[9] In the case reported here, prompt diagnosis led to immediate energetic treatment of the factor that triggered the condition, arterial hypertension, and the condition resolved clinically with 14 days of aggressive antihypertensive management in the ICU. In this clinical case, we found predisposing factors known to be associated with PRES. The most common clinical presentation is new-onset seizures, encephalopathy, headache, and visual disturbances. [11],[12] There may be abnormalities of vision such as hemianopia, visual neglect and cortical blindness. This patient did not present seizure or changes in consciousness, which is not frequently reported in the literature. The syndrome may not be completely reversible, is not always limited to the posterior regions, and may involve gray as well as white matter. [12],[13] Patients with an innocuous clinical picture may develop organ damage as a result of arterial hypertension. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11062f1.jpg] |
| |||||||||


{kind=link}