 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
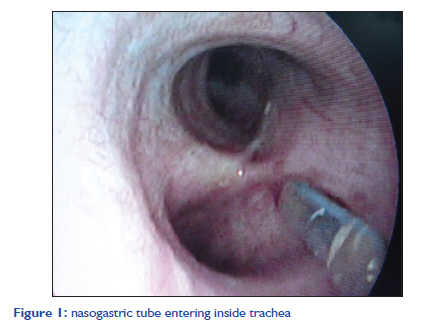
Indian Journal of Critical Care Medicine, Vol. 15, No. 4, October-December, 2011, pp. 237-238 Letter to the Editor An uncommon cause of intraoperative airleak Kapil Dev Soni, Babita Gupta, Pramendra Agrawal, Nita D«SQ»souza, Chandni Sinha Department of Anaesthesia, Jai Prakash Narayan Apex Trauma Centre, All India Institute of Medical Sciences, New Delhi, India Code Number: cm11066 DOI: 10.4103/0972-5229.92072 Sir, An airleak around endotracheal tube (ETT) may make maintenance of adequate ventilation difficult and it may lead to aspiration. We encountered a case wherein malpositioned nasogastric tube (NGT) caused airleak around the ETT. A 45-year-old man was brought with foreign body impalement of the face and cervical spine. Transoral exploration and disimpaction of iron rod (in supine posture) and posterior fixation (in prone posture) of occiput (C2-C3 with screw and rod fixation) was planned. Awake fiberoptic bronchoscopy (FOB)-assisted orotracheal intubation was done with flexometallic ETT. There was no airleak around the ETT and this was confirmed with end tidal CO2 monitor and pressure volume loop graphs. After removal of iron rod by transoral approach, NGT tube was inserted by the surgeon. Soon thereafter, airleak appeared on pressure volume graph along with audible leak. Seeking a cause for airleak, the pilot balloon of flexometallic tube was checked and was found to be intact. Air entry was bilaterally equal. Breathing circuit and ventilator were examined but no abnormality was identified. FOB was again performed to rule out ETT displacement. It was noticed that NGT, which was inserted at the end of the first part of the surgery, entered into the trachea alongside the intact cuff, reaching up to the carina [Figure - 1]. The NGT was pulled out and the airleak resolved. The insertion of NGT is a common procedure in anaesthesia and intensive care setting. Unnoticed insertion of the NGT into the tracheobronchial tree may be associated with serious complications such as pneumonia, atelectasis, bronchopleural fistula, pneumothorax, empyema, hydrothorax and even death. [1],[2],[3] Large studies have shown an incidence of tracheal malpositioning of approximately 2%. [3] The nature of presentation of this complication makes this case intriguing. Normally once the endotracheal tube cuff is inflated, it completely secures the airway. However, in this case nasogastric tube went alongside the intact inflated cuff (as evident by distended pilot baloon) into the trachea and caused air leak. NGT is usually inserted under vision with the help of direct laryngoscopy and magill forcep. However in this case, it was inserted blindly since there was involvement of cervical spine. Moreover FOB successfully identified the unexplained cause of airleak. Commonly accepted clinical signs for proper NGT placement are auscultation, fluid aspiration, absence of coughing [4] and visual inspection of gastric aspirate. [5] Bubbling sounds may be absent, especially in air-filled stomachs or are heard in the epigastrium while tubes are localized intrapulmonary or in the pleural space. In most cases of tracheal malpositions, NGTs were considered to be properly placed by auscultation. To conclude, low pressure inflated endotracheal cuff may not completely secure the airway and NGT can still negotiate alongside it causing airleak. We may suspect malpositioned NGT if an airleak occurs immediately after NGT insertion. FOB does increase the sensitivity to identify source of airleak and confirm malpositioned NGT. References
Copyright 2011 - Indian Journal of Critical Care Medicine The following images related to this document are available:Photo images[cm11066f1.jpg] |
| |||||||||

{kind=link}