 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
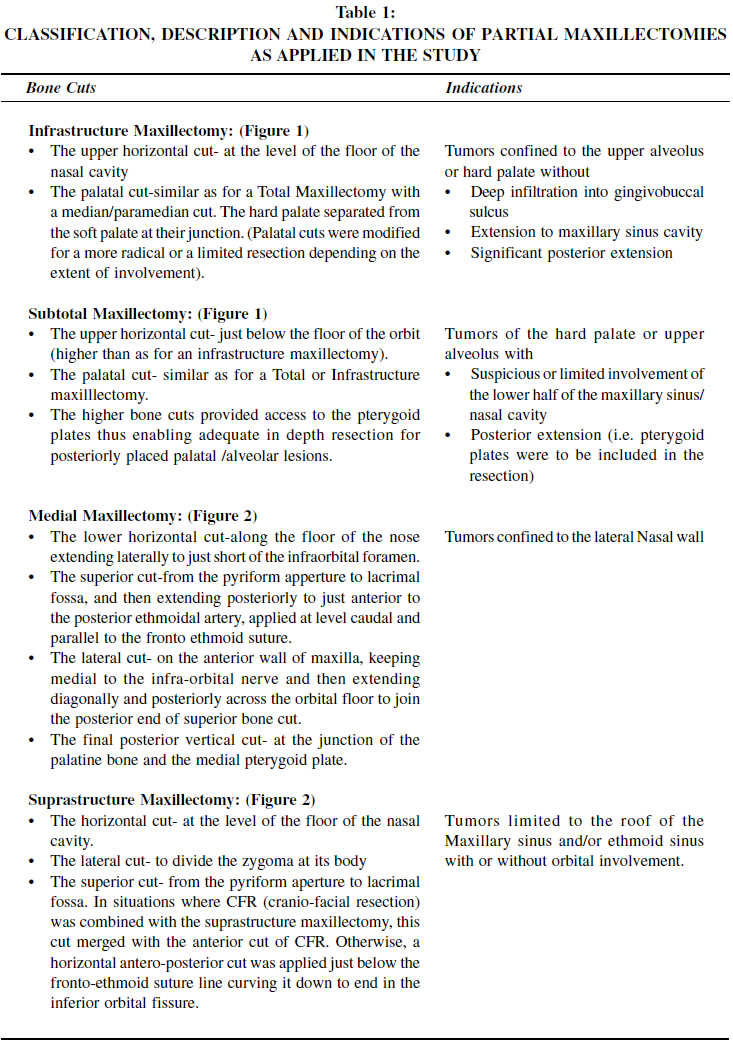
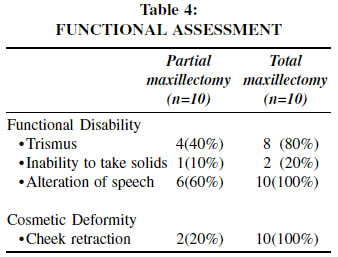
Indian Journal of Cancer, Vol. 39, No. 3, (July - September 2002), pp. 83-90 Partial Maxillectomy for Malignant Neoplasms of Para Nasal Sinuses and Hard Palate Bubul C. Roy, Sudhir Bahadur, Alok Thakar Dept. of Otorhinolaryngology & Head and Neck Surgery, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110 009. Code Number: cn02001 ABSTRACT BACKGROUND: The universal application of sectional imaging to the evaluation of para nasal sinus neoplasms has indicated that many of the regions encompassed in a total maxillectomy are often uninvolved and are perhaps unnecessarily resected. METHODS: A set of guidelines was formulated regarding the indications and techniques of partial maxillectomies. These guidelines were then tested on a prospective cohort of 20 cases. The adequacy was judged by histological evaluation of all resection margins. Morbidity was assessed in terms of functional parameters (trismus, swallowing disturbances, speech disturbances) and cosmetic parameters (cheek retraction). RESULTS: As per the pre-formulated guidelines a partial maxillectomy (PM) was suitable in ten and was undertaken. The same was unsuitable in the other ten and these therefore had a total maxillectomy (TM). Four of ten cases in each group had an involved resection margin. All such cases had additional treatment for the microscopic residual disease. In the four cases in the PM group with involved resection margins in none was this at the area with the limited resection. The status of the resection margins in these cases would not have been different even if they had had a total maxillectomy. Morbidity in the PM group was significantly less than in the TM group. CONCLUSION: By careful case- selection based on imaging, partial maxillectomy can provide for equivalent oncologic clearance as with a Total Maxillectomy, and significantly reduced morbidity. Key Words: Para Nasal Sinus Neoplasms, Palatal Neoplasms. INTRODUCTION Though head and neck cancer comprises nearly 30 percent of all malignancies in India, the proportion of neoplasms of the para nasal sinuses are small (0.8 to 2.7 percent).1-3 They usually present late as these malignancies become clinically manifest only when they cause bone erosion or extend beyond the confines of the sinuses.4 In view of the usual advanced extent of these lesions the standard surgical treatment has been a total maxillectomy. The morbidity of a total maxillectomy in terms of trismus, swallowing and speech disturbances, and cheek retraction is formidable A small subgroup of patients by virtue of the location of tumour may however present early. Moreover, with the universal application of imaging with CT/ MR in recent years it is increasingly obvious that some patients even with locally destructive disease do not have involvement of the entire complex that is routinely sacrificed in a total maxillectomy. In this subgroup of patients a total maxillectomy may be unnecessary and a partial resection may be oncologically adequate. Recent years have therefore seen a trend from radical to conservation surgery. Spiro and Strong (1997) reported that among all maxillectomies done between 1984 -1993 about 91% were partial maxillectomies.5 The availability of nasal endoscopes and sophisticated bone cutting tools has also contributed to the technical feasibility of these surgical procedures. Nevertheless there remain no universally established guidelines with regard to the indications for these procedures. The literature also presents a confounding array of nomenclatures and surgical modifications. The present study attempts to classify and to demarcate the indications for the various partial maxillectomies, as also to demonstrate their oncologic safety and functional and cosmetic benefits. PATIENTS AND METHODS The present prospective study included 20 biopsy proven and resectable cases of carcinoma of maxillo-ethmoid complex and hard palate who underwent surgical treatment in the department of Otorhinolaryngology & Head and Neck Surgery, All India Institute of Medical Sciences, New Delhi from June 1998 to June 2000. The nomenclature, surgical limits, and indications for the partial maxillectomies were clearly laid down prior to the recruitment of cases. These were based on the clinical and radiological evaluation. The indications for, and the exact extent of each surgical procedure are listed in Table 1. There were eleven males and nine females. Age at presentation ranged from 21 years to 72 years (mean age at presentation 46.05 years). The commonest histological variety was squamous cell carcinoma (9 cases-45%), followed by adenoid cystic carcinoma (5), mucoepidermoid carcinoma (3), adenocarcinoma (2) and olfactory neuroblastoma (1). Imaging (CT/ MRI) was undertaken in all cases. Staging was as per the AJC (1997) classification and based on clinical and radiological evaluation. Eighty five percent of patients (17/20) presented with advanced disease (T3/T4/ Kadish stage C) Table 2. The maxillectomy types undertaken are listed in Table 2. In all cases with a total maxillectomy and also the cases with subtotal maxillectomy, a split skin graft was used to line the cheek flap. The resected palate was replaced with an acrylic palatal prosthesis at the initial surgery itself. The cavity was meticulously attended to in the post-operative period. All surgical specimens were examined histopathologically to assess for tumor free resection margins and also to confirm the preoperative histological diagnosis. Seven cases had pre-operative radiotherapy and eleven had postoperative radiotherapy. Follow up ranged from 3.5 to 24 months (mean follow up 12 months) and consisted of regular clinical and periodic radiological evaluation. Recurrences were dealt with by either additional surgery, chemotherapy or radiation therapy. All cases were specifically assessed for functional morbidity (trismus, inability to swallow solids/liquids, alteration of speech), and for cosmetic deformity (cheek retraction). RESULTS Adequacy of resection In the study period 10 of the 20 cases operated had a partial maxillectomy (PM), while the other ten were not judged suitable for the same and had a total maxillectomy (TM). Four of ten cases in each group had histologically positive resection margins. Of the four cases with positive margins in the partial maxillectomy group, the histological status of the margins would not have differed even if they had had a total maxillectomy. Because these were in areas that are not included in standard bone cuts of a total maxillectomy. Adjuvant therapy was administered to all with positive resection margins. All four in the partial maxillectomy (PM) group and two of four in the total maxillectomy (TM) group had post-operative radiation (56 Gy). The other two cases in the TM group had had pre-operative radiation. One was treated by an additional local boost of radiation (15Gy) to the incriminated site and the other had an additional surgical excision of margin. The details of these cases and their eventual outcome are summarized in Table 3. Among the 12 cases with negative histological margins, 2 cases (one each from the PM and TM groups) developed subsequent recurrences. Overall, with the mean follow up of 10.7 months, disease free status was noted in 8/10 (80%) patients with partial maxillectomy as well as 8/10 (80%) patients with total maxillectomy. The results in terms of oncological resection and disease free status were therefore similar in both groups. Morbidity The functional and cosmetic morbidity in the two groups is summarised in Table 4. Some degree of cheek retraction and alteration of speech was invariable in all cases (10/10) of the total maxillectomy group. Trismus was also frequent (8/10) in this group. This was in spite of close attention to cavity hygiene, the provision of a palatal prosthesis and skin grafting of the cheek flap. In the partial maxillectomy group, cheek retraction was noted only in 20%(2/10) cases and occurred; following suprastructure maxillectomy and no other. Alterations of speech were noted in 60%(6/10) cases of the PM group and observed only in cases with palatal resection (infrastructure and subtotal). Trismus was also rare in this group (2/10). Swallowing problems were unusual (1/10). DISCUSSION Many variables enter into the decision regarding the best therapy for a patient with a malignant para nasal sinus neoplasm. The varieties of histological types and the complicated anatomy along with the significant consequences of their surgical extirpation are major considerations. The role of adjuvant radiation or chemotherapy is greatly dependent on the histological type. Many tumours are already judged unresectable by conventional techniques at presentation. Nevertheless surgery is sometimes undertaken with the hope that, in conjunction with the available adjuvant therapies, it would yield benefits and possibly cure. It is near impossible to have a scientifically designed study wherein all such variables are accounted for, especially keeping in mind the overall paucity of such cases. Many of the previous reports on partial maxillectomy are not directly relevant to the current situation as they relate to the era prior to routine CT and MR imaging. The present study seeks to clearly define partial maxillectomies into various types and to lay down the indications and limitations of each. It has been conducted as a prospective audit of a predefined practice and seeks to validate this defined practice (Table 1). It indicates that by adhering to the defined set of indications for each partial maxillectomy, a comparable oncological resection can be achieved and the morbidity significantly reduced. There is strong evidence that for cancers of the maxillary complex, a combination of surgery and radiotherapy yields the best results.6-9 The standard surgical treatment for carcinoma of maxilla is a total maxillectomy (with or without orbital exenteration) with its consequent functional morbidity and cosmetic deformity. The 5-year survival rate after combined treatment varies from 44% to 59% in recent publications. 10,11 The role of partial maxillectomy for carcinoma of maxilla is not well defined. There is no consensus in the literature on the nomenclature for less than total maxillectomies. In many publications the term `partial' and `subtotal' have been used interchangeably. Spiro et al (1997) divided maxillectomies into limited, subtotal and total depending on whether the resection involved predominantly one wall, at least two walls including the palate, or the entire maxillas. In the present study we have retained the term `partial' by which we mean anything less than a total resection. The various maxillectomies included under the heading of partial maxillectomy in the present series were infrastructure (where only the upper alveolus and hard palate below the level of nasal floor were removed), medial (where medial wall of maxilla medial to the infraorbital nerve along with the medial 1/3rd of inferior orbital wall and the medial orbital wall were removed), suprastructure (where all the walls of maxilla, except hard palate and upper alveolus, were removed) and subtotal (where all the walls of maxilla, except the orbital floor and the zygomatic buttress, were removed) (Table 1, Figures 1 & 2). Sessions and Larson (1977) described medial maxillectomy as an enbloc resection of the ethmoid labyrinth and medial aspect of maxilla from the cribriform plate to the nasal floor inferiorly, and from the anterior extent of the ethmoidal cells back to the area of the optic nerve. In the procedure they preserved the ascending process of maxilla, the nasolacrimal apparatus and the bony orbital rim. In a subsequent modification (1983) they transected the lacrimal sac and cannulated it with 14-gauge polyethylene tube and re-approximated the medial palpebral ligament.12 While we do re-approximate the medial palpebral ligament, we have not stented the lacrimal apparatus. Neither has been associated with an adverse cosmetic result or with epiphora. Also, it is not always possible to remove all the ethmoid cells enbloc, and some additional clearance of these cells is required after the initial resection. Stern et al (1993) described infrastructure maxillectomy as a procedure where the portions of maxilla below the level of the infra-orbital nerve along with the hard palate were removed.13 Truit et al (1999) however have limited this term to a resection restricted to the maxilla below the level of the nasal floor.14 The bone cuts of infrastructure maxillectomy as employed in the present study are similar to that by Truit et al. An antrotomy prior to the resection is necessary to confirm that the maxillary sinus is uninvolved. The pterygoid plates need to be separated from the maxillary tuberosity to deliver the specimen. Spiro et al (1997) designated a subtotal maxillectomy as one where at least two walls of maxilla along with the palate are removed, but the posterior wall is spared.5 Cocke et al (1990) described extended subtotal maxillectomy as one where orbital floor was preserved removing all other wall of the maxillary sinus along with pterygoid plates.15 In the present study by subtotal maxillectomy we meant removal of all other walls of maxilla preserving the orbital floor and zygomatic buttress. Extension of this procedure to include pterygoid plates or nasal septum was possible and was specified. In a suprastructure maxillectomy the lower horizontal cut was given at the level of the nasal floor. The rest of the bone cuts were applied similar to a total maxillectomy. It was possible to combine orbital exenteration or craniofacial resection with this procedure. The preservation of the hard palate was associated with improved functional results in terms of ability to swallow and quality of speech. Adequacy of oncological resection is judged by the histopathological examination of the resected margins. Unfortunately this is not assured even with a total maxillectomy. By relying on a meticulous radiological evaluation, and well-defined and strict indications for partial maxillectomies, we did not find any compromise in the adequacy of resection. In the 4 cases of partial maxillectomy wherein positive histological margins were encountered, these were at areas, which are usually not included even in the en bloc resection of a standard total maxillectomy. All these 4 patients received postoperative radiotherapy and 3 of them are surviving free of disease. Out of 6 patients with negative margins, 5 patients were surviving free of disease and one patient developed regional recurrence. These results were similar to those achieved with a total maxillectomy. Previous workers have opined that provided histological margins are free and radiotherapy is also employed, there may be no difference in cure rates between partial, total or radical maxillectomy.16-18 The various reported survival figures with such a policy of a partial maxillectomy combined with pre or postoperative radiation and have ranged from 44% to 85%.14,18-20 While the diversity of the disease location, staging and histology in these reports does defy a simple interpretation, nevertheless we believe that the use of adjuvant treatment with radiotherapy is prudent in almost all such cases - whether treated by partial or total maxillectomy. Though the functional and cosmetic problems following a total or radical maxillectomy is known to all, very little attention has been paid in the literature to their assessment factors. Most of the literature has focussed on the complications of the eye when preserved and the complications of a craniofacial resection. In this present study, functional morbidity has been assessed in terms of trismus, inability to take solids and alteration of speech and the cosmetic deformity in terms of cheek retraction. In spite of meticulous attention to cavity care and hygiene and the provision of a palatal prosthesis in the immediate post-operative period, such problems were extremely frequent in the total maxillectomy group. Morbidity in the partial maxillectomy group was significantly reduced. Trismus and swallowing and speech disturbances however did occur following subtotal and infrastructure maxillectomy but to a much less degree. Preservation of the palate in suprastructure and medial maxillectomy seems to have the greatest role in reducing functional morbidity. Cheek retraction only occurred following suprastructure maxillectomy. The post-operative cosmetic appearance was significantly better in partial maxillectomy than in total maxillectomy group. The preservation of the zygomatic buttress seems to be the most important in this regard. CONCLUSION Surgical resection of PNS neoplasms is often unsatisfactory. Current practices involve the use of imaging in the selection of the surgical procedure. A classification of partial maxillectomies is proposed and the respective indications and limitations of each have been clearly defined. By adherence to these defined indications, partial maxillectomy seems to offer comparable oncological resection as a total maxillectomy, and also significantly limits functional and cosmetic disability. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02001t4.jpg] [cn02001f1.jpg] [cn02001t2.jpg] [cn02001t1.jpg] [cn02001t3.jpg] [cn02001f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}