 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
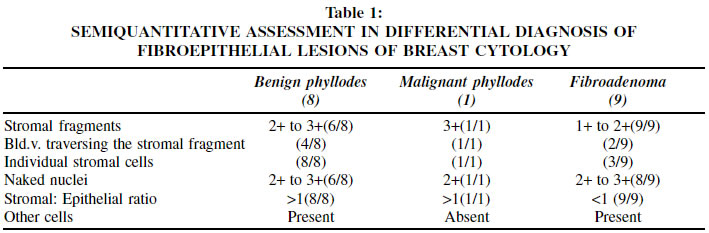
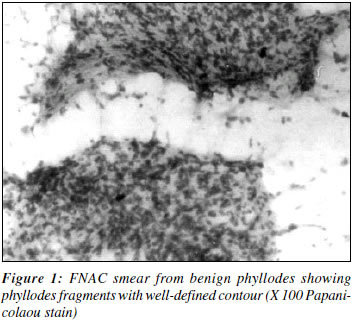
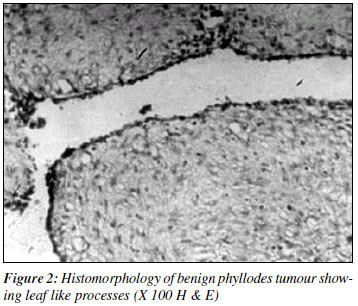
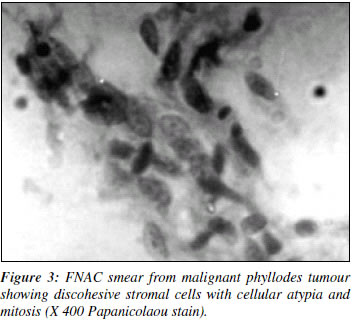
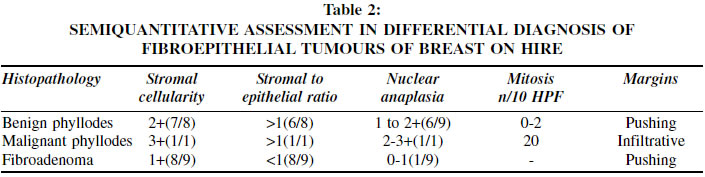
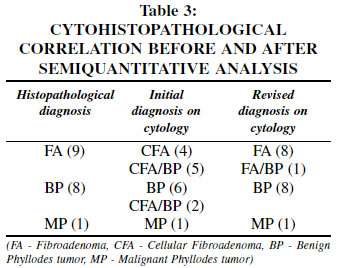
Indian Journal of Cancer, Vol. 39, No. 3, (July - September 2002), pp. 91-96 A STUDY OF FIBROEPITHELIAL TUMOURS OF THE BREAST Bhawana A. Badhe, M.D. Associate Professor, Krishnan R. Iyengar, M.D. Associate Professor, Nandakishor Alva, M.D.Senior Resident Department of Pathology, Jawaharlal Institute of Postgraduate Medical Education and Research Pondicherry 605 006, India. Code Number: cn02002 ABSTRACT Cytological parameters were studied in 18 fibroepithelial tumours of the breast including 8 benign phyllodes, 1 malignant phyllodes, and 9 fibroadenomas between 1999 to 2001. Cytology smears were studied without knowledge of previous cytodiagnosis by 3 different observers. Histopathologic parameters were studied in 18 fibroepithelial tumours by 3 observers. Cyto-histological correlation was carried out. Cytological criteria by Chinoy et al (1999) were utilized to give revised cytodiagnosis. Initial cytodiagnosis and revised cytodiagnosis were correlated with histopathological diagnosis. 8/9 cases of fibroadenoma (88%) studied were correctly diagnosed on FNAC after semiquantitative team approach as opposite to 44% initial cytodiagnosis. Cytological distinction between benign phyllodes and fibroadenoma was improved after semiquantitative approach to various parameters. Diagnosis of malignant phyllodes posed no problems in cytodiagnosis. Present study supports the role of FNAC in distinguishing benign from malignant phyllodes and distinguishing fibroadenoma from phyllodes tumour. The latter being a rare fibroepithelial tumour, its study is interesting. Key Words: Aspiration Cytology, Breast, Fibroepithelial tumours. INTRODUCTION With increased cancer awareness, palpable breast lump is a common diagnostic problem to general practitioners and to surgeons. In the past, excision biopsy was a common practice. With the advent of preoperative diagnosis by aspiration cytology, patients' anxiety can be relieved immediately. Fibroadenoma is common among the benign fibro epithelial tumours of the breast while phyllodes tumour is relatively a rare breast neoplasm, which can be diagnosed on FNAC. A team approach to differentiate benign from malignant breast lump has improved the accuracy. Present study was conducted to carry out cytohistopathological correlation in 18 fibro epithelial tumours of the breast. PATIENTS AND METHODS Study of fibroepithelial tumours of the breast was conducted from January 1999 to July 2001. Careful clinical examination, fine needle aspiration cytology and histopathology of 18 fibroepithelial tumours of female breast were carried out. Cytological criteria by Chinoy et al (1999)4 were utilised for cytodiagnosis of fibroepithelial tumours to give a preoperative diagnosis on breast lumps. Histopathological criteria used by Hawkins et al (1992) and Ward et al (1986)5 were utilised to grade phyllodes tumours. Clinico-cyto-histopathological correlation was done in 18 fibroepithelial tumours of the breast by three different observers. RESULT This study was conducted in the Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry from 1999 to 2001. Eighteen cases of fibroepithelial tumours of female breast included 8 cases of benign phyllodes, one case of malignant phyllodes and 9 cases of fibro adenomas. Patients with benign phyllodes were in the age group of 25-60 years; one case of malignant phyllodes was 42 years of age. Nine cases of fibroadenoma were of the age group of 18-42 years. All the patients presented with a lump in breast and duration of symptoms ranged from 3 months to 4 years. Patients were preoperatively diagnosed by FNAC using standard technique. Smears were stained by Papanicolaou and May Grunwald-Giemsa stain. Features utilised for diagnosis of fibroadenoma on cytology were high epithelial cell yield, large branching monolayered sheets of uniform epithelial cells, numerous single, bare, bipolar nuclei and fragments of fibromyxoid stroma. Criteria used for diagnosing phyllodes tumour on FNAC were predominance of stromal over epithelial elements, higher stromal cellularity, presence of phyllodes fragments (i.e. abundant leaf like stromal fragments), myxoid stroma and single bare nuclei. Atypia in stromal cells of fragments, bare nuclei and epithelial cells was noted if present. Malignant phyllodes was diagnosed on FNAC when discohesive sheets of abundant stromal cells with stromal cell atypia and more than occasional mitosis per smear was noticed. Semiquantitative assessment using scoring of parameters was carried out. Stromal fragments were scored 1+ to 4+, naked nuclei were scored as 1+ to 3+ and stromal to epithelial ratio was scored as <1, =1, >1 per case. Mitosis was scored as 0, 1+ (very occasional), 2+ more than occasional (Table 1). Table 1 shows semiquantitative assessment of cytological findings in our study. Fibroadenoma8 cases showed abundant epithelial cohesive clusters, scanty stromal fragments with blurred fuzzy indistinct contour, scanty stromal fragment cellularity, often showed apocrine cells, foam cells and giant cells. Stromal to epithelial ratio was less than one. One patient with 7 cm breast lump was diagnosed as phyllodes on cytology based on semiquantitative assessment, showed fibroadenoma on biopsy. Eight cases of benign phyllodes showed abundant knobby highly cellular stromal fragments, increased stromal to epithelial ratio. Occasional case showed foam cells and apocrine cells. Individual stromal cells were observed in all the cases (Figures 1 & 2). One case was diagnosed on FNAC as fibroadenoma, was diagnosed as benign phyllodes on histopathology. One case diagnosed on FNAC as fibroadenoma showed focal hypercellularity with atypia on histopathology and the diagnosis of benign phyllodes was given on histopathology. One case of malignant phyllodes diagnosed by FNAC showed very occasional small epithelial clusters, abundant discohesive stromal cell fragments with atypia (Figure 3). Stromal cells showed 3 mitotic figures in 2 FNAC smears studied. Bipolar nuclei, foam and apocrine cells were conspicuously absent in this case. Nine fibroadenomas were treated by lumpectomy. The treatment for phyllodes tumour comprised of wide excision (1 case) simple mastectomy with (3 cases) or without (4 cases) axillary resection. Malignant phyllodes was treated by radical mastectomy. Three out of eight cases were recurrent phyllodes. The period of recurrence was found to be 6 months to 3 years. Pathological assessment of fibroepithelial lesions was carried out to differentiate fibroadenoma, benign and malignant phyllodes. Phyllodes were larger than fibroadenomas. The outer surface of phyllodes showed projections as opposite to fibroadenoma. The surfaces of fibroadenomas were smooth. Phyllodes on cut section showed cleft like spaces in all eight phyllodes tumours studied. Three showed typical cut-cabbage appearance. One case showed gelatinous and mucoid areas. One case of malignant phyllodes showed areas of necrosis and haemorrhage. Microscopic examination was carried out with semiquantitative assessment of various parameters. Neoplastic stromal cells were scored 1 + to 4+, stromal to epithelial ratio >1, =1, <1, nuclear anaplasia was scored as 0-1+, 1-2+, 2-3+, mitotic activity was scored as <5/10 HPF and >5/10 HPF (Table 2). Stromal cellularity, nuclear atypia, mitosis and examination of margins helped to distinguish cellular fibroadenomas, benign and malignant phyllodes. Phyllodes showed predominantly intracanalicular growth pattern and stromal hypercellularity. One case had typical intracanalicular fibroadenomatous pattern with focal stromal hypercellularity with atypia indicating presence of phyllodes tumour. Malignant phyllodes showed higher nuclear anaplasia and showed 20 mitotic figures per 10 high power field and >95% infiltrative margins with areas of haemorrhage and necrosis. 3/8 benign phyllodes showed local recurrence suggesting incomplete excision at the first diagnosis. There was no diagnostic difficulty in distinguishing benign from malignant phyllodes. Table 3 shows cytohistopathological correlation of 18 cases of fibroepithelial tumours. Semiquantitative team approach improved the cytodiagnosis. Cytological differentiation between cellular fibroadenoma and benign phyllodes was improved. The diagnosis of malignant phyllodes posed no difficulty in cytodiagnosis. DISCUSSION Cytodiagnosis of fibroepithelial lesions of the breast is helpful in planning the extent of surgery. Biphasic fibroepithelial tumours arise from specialised stroma of the breast. Majority of them are fibroadenomas and less common fall in the category of phyllodes tumours. Phyllodes tumour is the term recommended by WHO for the tumors previously called as cystosarcoma phyllodes. Although phyllodes tumour show many features of fibroadenoma they are more likely, to recur and some are locally aggressive and can even metastasize. The recurrence of phyllodes is directly related to incomplete resection without adequate margin of normal breast tissue. Correct planning of surgery requires correct cytodiagnosis, the accuracy of which can be improved by applying semiquantitative assessment utilising selected criteria. Present study supports the importance of cytodiagnosis in distinguishing cellular fibroadenomas from benign phyllodes tumour and to distinguish benign from malignant phyllodes. Some authors suggested a borderline group where intermediate tumours of questionable malignancy were categorised as `borderline.4-6 However, validity of such histologic grouping is questionable, as the behaviour of these tumors has proven unpredictable.7 Several authors have attempted to define objective cytologic features that can help in distinguishing fibroadenomas from phyllodes tumors, with varying results.8-11 But the one feature that is uniformly observed in phyllodes tumor cytology is the abundance of stromal cells with many of them seen individually. Krishnamurthy et al have observed that presence of a significant proportion of long spindle nuclei (> 30%) among the background stromal cells is strongly indicative of phyllodes tumor whereas the stromal cell nuclei in fibroadenoma tends to be short and oval.8 The authors have stated that long spindle nuclei accounting for 10 - 30% of the background nuclei may be seen in both fibroadenomas and phyllodes tumors. They prefer the term `indeterminate' to designate such lesions. The present study did not quantify the individual stromal cells in the background, however these were present in fewer cases of fibroadenoma (3/9) as compared to phyllodes tumor (9/9) (Table 1). The single case where it was not possible to distinguish between the two lesions even after the semiquantitative evaluation should probably be categorized as `indeterminate'. The other case where a diagnosis of fibroadenoma was proved wrong by histopathology was one of sampling error, because the atypical features were evident only focally in the biopsy. These two cases were valuable in reminding the authors of limitations of fine needle aspiration cytology. Phyllodes tumor accounts for 1% of breast neoplasms and 2-3% of fibroepithelial tumours. Histopathological categorization between benign and malignant phyllodes is important, as 21-31% of cases are malignant.2 Kessinger and associates reported metastasis in 3-12% of cystosarcomas. Local recurrence has been noted in 24% in one series. Recurrence has been attributed to incomplete removal.2 Three out of eight cases in the present study were recurrent phyllodes. Larger size of the tumour necessitated total mastectomy. Simi et al1 studied 20 fibroadenoma, 4 benign and one malignant phyllodes tumor. This author found cytological semiquantitative assessment on cytology useful in accurate diagnosis of fibroadenoma, benign phyloides, and malignant phyllodes. Rama Rao et al3 categorized phyllodes in benign borderline and malignant by cytological semi quantitative approach to aid accurate preoperative diagnosis and recommended multiple site aspiration to detect focal hypercellularity in phyllodes tumour. This author found recurrent phyllodes to be more cellular with greater degree of atypia. Chinoy et al studied 10 benign, 2 borderline and 5 malignant phyllodes by cytological sub categorization using semi quantitative analysis by team approach. Present study supported above-mentioned studies. However, present study did not reveal questionable malignant borderline phyllodes tumour. Present study concludes that stromal overgrowth is the single most important criteria distinguishing phyllodes from fibroadenoma. Histological grading of phyllodes based on stromal cellularity, tumour margin and mitotic rate helps to distinguish benign from malignant phyllodes. Preoperative cytodiagnosis utilising clinical and semi quantitative assessment of cytological smear is necessary to plan treatment in phyllodes. However, it is interesting to note the results of Norris and Taylor. These authors found no single histopathological feature completely reliable in predicting clinical behaviour in phyllodes. Hart, Baur et al recommended all cystosarcomas to be regarded as more or less aggressive tumour and to append the designation "low grade" to those lacking overtly sarcomatous stroma.2 Recent advances in flow-cytometric analysis of ploidy and phase fraction may give valuable prognostic information in phyllodes. REFERENCES
Copyright 2002 - Indian Journal of Cancer. The following images related to this document are available:Photo images[cn02002t2.jpg] [cn02002f2.jpg] [cn02002t1.jpg] [cn02002t3.jpg] [cn02002f3.jpg] [cn02002f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}